
Abstract
The elbow joint is one of the feline appendicular joints most commonly and severely affected by degenerative joint disease. The macroscopic and histopathological lesions of the elbow joints of 30 adult cats were evaluated immediately after euthanasia. Macroscopic evidence of degenerative joint disease was found in 22 of 30 cats (39 elbow joints) (73.33% cats; 65% elbow joints), and macroscopic cartilage erosion ranged from mild fibrillation to complete ulceration of the hyaline cartilage with exposure of the subchondral bone. Distribution of the lesions in the cartilage indicated the presence of medial compartment joint disease (most severe lesions located in the medial coronoid process of the ulna and medial humeral epicondyle). Synovitis scores were mild overall and correlated only weakly with macroscopic cartilage damage. Intra-articular osteochondral fragments either free or attached to the synovium were found in 10 joints. Macroscopic or histologic evidence of a fragmented coronoid process was not found even in those cases with intra-articular osteochondral fragments. Lesions observed in these animals are most consistent with synovial osteochondromatosis secondary to degenerative joint disease. The pathogenesis for the medial compartmentalization of these lesions has not been established, but a fragmented medial coronoid process or osteochondritis dissecans does not appear to play a role.
Keywords
Appendicular degenerative joint disease (DJD) is a condition commonly present in domestic cats. Prevalence of radiographic signs of appendicular DJD in this species varies with age and has been reported to range from 16.5% to 91%. 5,12,15,19,29 Joints reported to be most commonly affected in prospective studies are hip and stifle 19 or shoulder and elbow. 29 Radiographic evidence of DJD in the elbow joint in cats has a prevalence of approximately 41%, and bilateral disease has been reported in 28% of cases. 19
The predominant cause of DJD in the cat has not been identified, 18 and it is suggested that most cases of feline DJD are primary or idiopathic. 4,5,12 The elbow joint is commonly affected by DJD in dogs as well, 20 but unlike cats, most canine patients with elbow joint DJD have known underlying predisposing factors such as a fragmented medial coronoid process (FMCP) or osteochondritis dissecans (OCD). To date, these forms of elbow dysplasia have not been proven to be present in cats. One report suggested the occurrence of elbow dysplasia (FMCP) as a cause of elbow disease in a feline patient after removal of several osteochondral fragments from both elbow joints. 31 As part of a separate study, we have observed similar fragments in cats with elbow DJD, in which evidence of macroscopic cartilage damage is present but with apparently intact coronoid processes of the ulna on macroscopic examination. 11 The presence of free ossified fragments has been identified in shoulder, stifle, and elbow joints in cats and considered either osteophytes that have not been completely incorporated within the epiphysis or “osteochondromas” resulting from hyperplasia of the synovial membrane and synovial chondrometaplasia. 2,32 In neither of these studies was a thorough histopathological evaluation of the free osteochondral fragments, medial coronoid process, or synovial membrane reported. Histological changes of the humeral condyle in cats with and without DJD have recently been published and suggested concentration of the lesions in the medial part of the humeral condyle, 28 but this work did not evaluate other articular surfaces or the synovial membrane, and it was not designed to look for possible causes of feline elbow DJD.
Even though the prevalence of radiographic signs of DJD in the elbow joint in cats is high and FMCP has been suggested to be present in this species, the etiology of feline elbow DJD is unknown, and the presence of feline elbow dysplasia has not been confirmed. The objective of this study is to report the histological characteristics of the articular surfaces, synovial membranes, and intra-articular osteochondral fragments in elbow joints from cats with and without DJD and compare the findings with those reported to be present in dogs with FMCP. We hypothesized that elbow joints with macroscopic evidence of DJD and the presence of intra-articular osteochondral fragments had histological evidence of a fragmented coronoid process (similar to dogs) and that the degree of macroscopic and histological damage of the articular surfaces correlated with the severity of synovial inflammation and hyperplasia.
Materials and Methods
This study was a prospective study using autopsy material.
Animals
Thirty adult cats, scheduled for euthanasia at a local animal shelter, were included. These animals were part of a previous study performed by the same laboratory. 11 Selection of these animals was such that will increase the likelihood of finding animals with different degrees of osteoarthritis (eg, selecting for older animals to increase the chance of finding joints with DJD). Animals were euthanized with an overdose of barbiturates for reasons unrelated to this study (population control). Age and sex of the cats were recorded. Clinical history of these animals prior to euthanasia was not known.
Macroscopic Examination
Immediately after euthanasia, both elbow joints of each cat were opened and the joints were visually inspected for the presence of macroscopic lesions as described previously. 11 The articular cartilage of the humerus, radius, and ulna of each joint was evaluated grossly for fibrillation and/or erosion of the cartilage surface using India ink 23 as previously reported. 11 Briefly, after gross observations were recorded, the cartilage surfaces were painted with India ink twice, rinsing the cartilage with water 3 minutes after the ink was applied. The severity of surface damage of the articular cartilage was scored based on ink retention and graded according to the scale described in a previous study: 33 grade 1—intact surface: surface appears normal and does not retain any ink; grade 2—minimal fibrillation: site appears normal before staining but retains India ink as elongated specks or light gray patches; grade 3—overt fibrillation: the cartilage is velvety in appearance and retains ink as intense black patches; and grade 4—ulceration: loss of cartilage exposing the underlying bone. Only severity of cartilage damage was graded, independently of the extent of the lesion.
Early during the dissection, the medial coronoid process was also grossly evaluated for the presence of cartilage fissures or intra-articular fragments that could be secondary to medial coronoid fragmentation.
Histopathology of Elbow Joints
Following macroscopic examination, a section containing the articular surfaces of the proximal ulna and radius and distal humerus, as well as a sample of the joint capsule/synovium, was immediately placed in 10% neutral buffered formalin for at least 48 hours. Decalcification of the bone specimens was achieved using 10% formic acid solution for a variable time length (7–14 days) depending on the size of the samples. After decalcification, sections perpendicular to the articular surfaces of each bone were cut making sure the area with the most severe macroscopic cartilage fibrillation was included. These sections were performed so that they included the coronoid and anconeal processes of the ulna in all cases following a parasagittal plane. Sections of the humerus and radius were performed in the frontal plane. Two serial sections of the bone specimens were mounted onto glass slides and stained with hematoxylin and eosin (HE) and Safranin-O (SO). Sections of joint capsule/synovium were stained with HE. Osteochondral fragments found within the joint or attached to the joint capsule were collected, processed, and stained in the same manner as the bone specimens.
The bone, joint capsule, and osteochondral fragments were evaluated microscopically (Olympus microscope BX41TF [Olympus America, Center Valley, PA]; Nikon microscope camera DS 2Mv [Nikon, Tokyo, Japan]). A descriptive approach was used to evaluate the histological changes present in the articular cartilage and subchondral bone, using combination of the Mankin and OARSI (Osteoarthritis Research Society International) histological and histochemical scoring systems to create a unique scoring system relevant to this study (Suppl. Table S1). 21,26 This enabled semi-quantitative evaluation of structural changes in all layers of the uncalcified hyaline cartilage, calcified cartilage zone, tidemark integrity, and the intensity of SO staining as well as changes identified in the subchondral bone. The sections were evaluated at different magnifications for the individual parts of the scoring system. The degree of synovitis was evaluated and graded using the grading system previously described by Krenn et al 17 (Suppl. Table S2). Changes observed in 3 histologic structures (synovial lining cell layer, stroma cell density, and inflammatory infiltrate) were assigned a numerical score: none (0), slight (1), moderate (2), and strong (3). These individual scores were summed to determine a final total score, and the final scores for each sample were interpreted as follows: 0 to 1, no synovitis; 2 to 4, low-grade synovitis; and 5 to 9, high-grade synovitis. Evaluation was performed at the area of the specimen with the most marked histopathological alterations.
Statistical Analysis
The mean ± standard deviation (SD) macroscopic and microscopic cartilage damage scores of the ulna, humerus, and radius were compared using the Wilcoxon signed-rank test. Bonferroni correction for multiple comparisons was used, and results were considered significantly different when P < .016. Spearman’s rank correlation coefficient was used to assess correlation between synovitis scores of each joint and the worse macroscopic and microscopic cartilage damage scores (the highest score of the 3 bones of each joint). Values of P < .05 were considered significant.
Results
A total of 30 animals were included in the study. There were 19 females and 11 males. Age was known in 18 animals and ranged from 7 to 19 years. Because of unknown previous history, age was speculated in 12 animals; 9 were considered young adults (age range approximately between 2 and 7 years), and in 3, age was suspected to be at least between 10 and 13 years.
Macroscopic Findings
Twenty-two of the 30 cats (73.3% of cats; 39 elbow joints; 115 of 180 bones; 64% of all articular surfaces) had macroscopic lesions of the articular cartilage that ranged from mild fibrillation to complete ulceration of the cartilage with exposure of the subchondral bone. Sixty-five articular surfaces (36%) were grossly normal, and there was no retention of India ink (grade 1); 78 (43%) had mild macroscopic cartilage fibrillation (grade 2); 19 (11%) had severe macroscopic cartilage fibrillation (grade 3); and 18 (10%) had complete ulceration of the articular cartilage with exposure of the subchondral bone (grade 4) (Table 1; Fig. 1).
Details of the Severity Grades of Macroscopic Cartilage Damage of the Humerus, Radius, and Ulna Articular Surfaces.
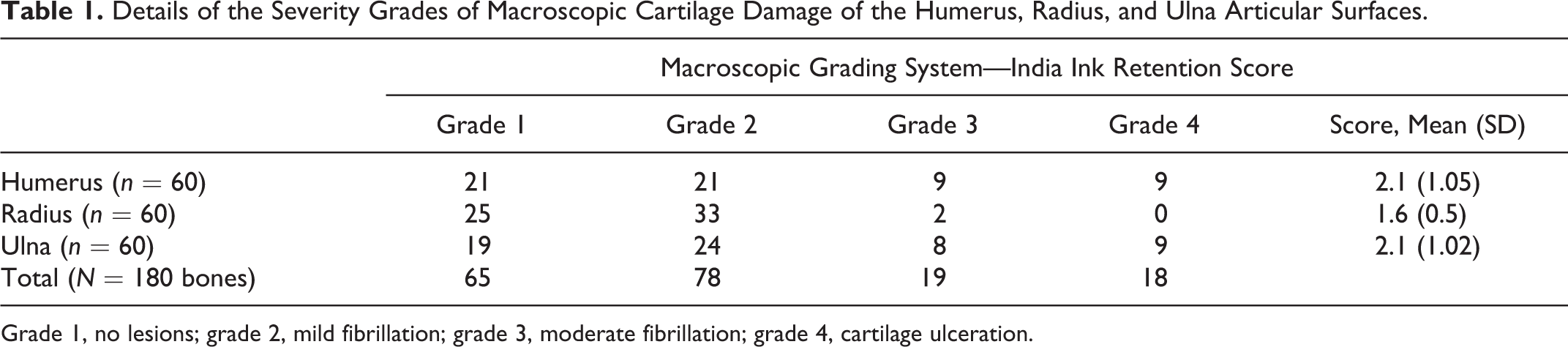
Grade 1, no lesions; grade 2, mild fibrillation; grade 3, moderate fibrillation; grade 4, cartilage ulceration.

Macroscopic cartilage lesions were bilateral when present, and the degree of damage to the articular surfaces was similar in both elbow joints. Macroscopic lesions of the articular cartilage with the most severe degree of cartilage erosion were located in the medial compartment of the joints (articular surface of the medial coronoid process and medial aspect of the humeral condyle). All animals that did not have macroscopic lesions were young adults (estimated between 2 and 7 years of age), and the most severe lesions with ulceration of the cartilage were found only in animals older than 10 years.
Microscopic Findings
The articular surface of 180 bones (radius, ulna, and humerus of each elbow joint) was evaluated grossly, with 176 bones evaluated histologically (4 specimens were not processed appropriately and slides were not considered of sufficient quality for evaluation). These 176 samples represent 1 section from each of the 3 bones comprising the elbow joint, taken bilaterally from 30 cats.
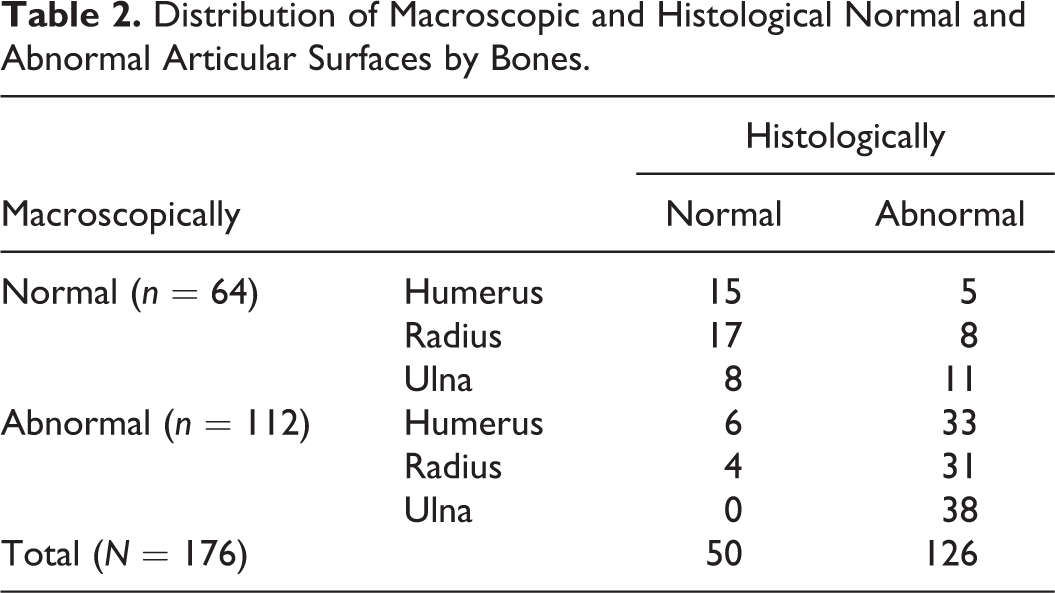
Of the 64 grossly normal articular surfaces that were evaluated histologically, 40 were histologically normal and abnormalities were detected in 24 specimens. Of the 112 grossly abnormal articular surfaces evaluated histologically, 10 were histologically normal and 102 were histologically abnormal (Table 2). Histological abnormalities are described below.
Distribution of Macroscopic and Histological Normal and Abnormal Articular Surfaces by Bones.
Histological Characteristics of Macroscopically Normal Samples
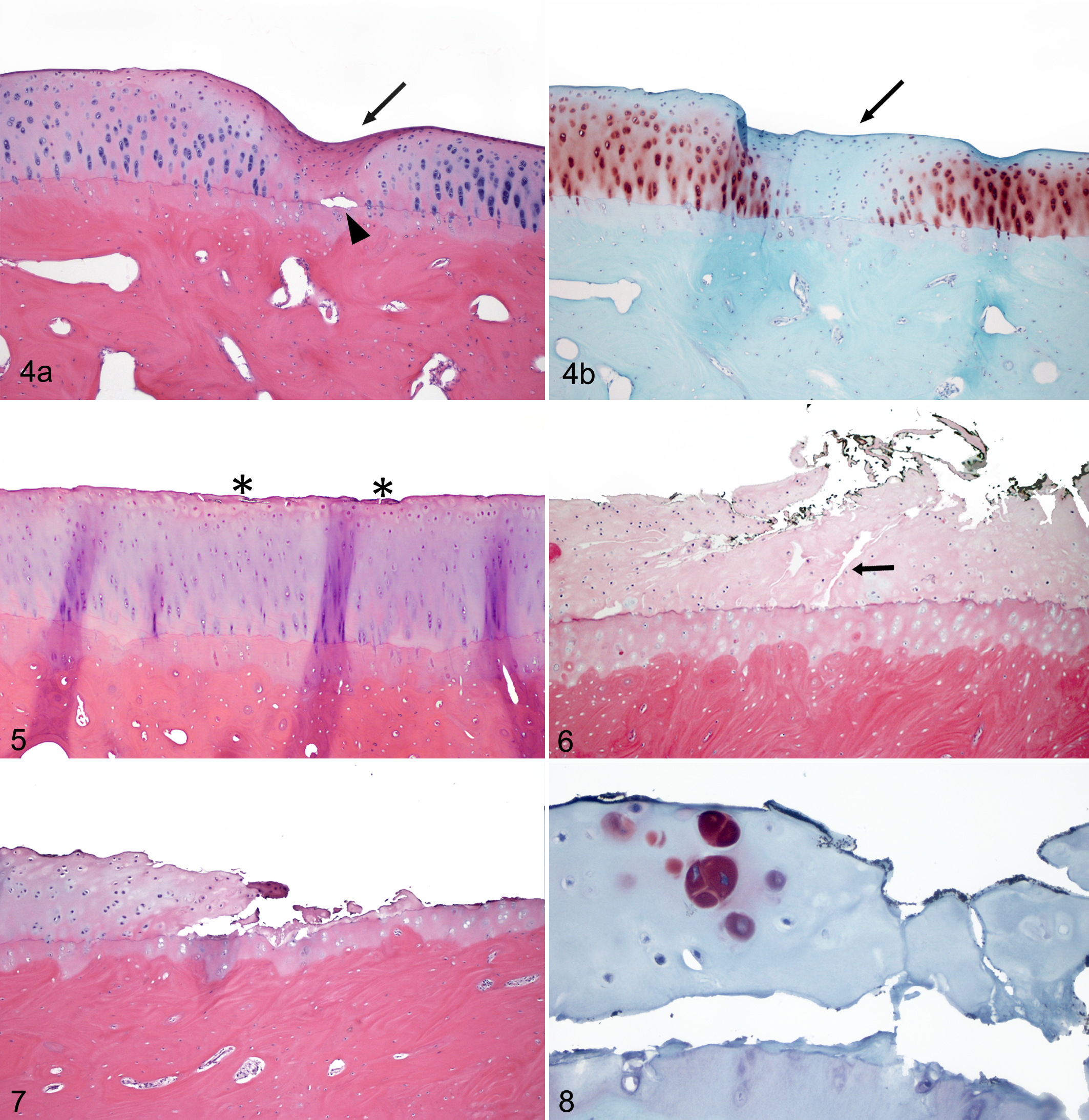
Sixty-four samples with no India ink retention by the cartilage were evaluated histologically; of those, 40 samples were also considered microscopically normal. These samples were characterized by the absence of cartilage fibrillation, normal density and number of chondrocytes organized in columns, normal intensity of SO staining, a single tidemark not crossed by blood vessels, and absence of changes in the subchondral bone, such as no increase in woven bone or islands of cartilage or fibrosis in the bone marrow spaces (Suppl. Figure S1). Microscopic lesions were observed in 24 samples without any evidence of macroscopic fibrillation of the cartilage (no India ink retention by the cartilage surface). These lesions were characterized by moderate to severely decreased SO staining, decreased number and size of chondrocytes, and occasionally deep fissures separating the hyaline cartilage from the deeper calcified cartilage (at the level of the tidemark; 4 specimens) (Fig. 4). No superficial fibrillation of the hyaline cartilage was present in these cases. These lesions were always observed as focal, particularly in the ulna, located in the articular cartilage covering the coronoid process. Fissures or microfractures of the subchondral bone at this level that could indicate deeper lesions or diseases involving the subchondral bone were not observed. Adjacent to the focal lesions, which were approximately 400 to 500 μm in length, the articular cartilage was normal.
Histological Characteristics of Macroscopically Abnormal Samples
Macroscopic fibrillation of the articular surfaces was accompanied by microscopic lesions in 102 of the 112 macroscopically abnormal samples evaluated. Ten specimens with macroscopic fibrillation of the cartilage were considered normal histologically. Histological lesions were characterized by different degrees of fibrillation of the hyaline cartilage, decreased intensity of SO staining, decreased number and size of chondrocytes as well as disorganization of the chondrocyte columns, and changes in the subchondral bone.
In cases with mild or moderate degrees of macroscopic cartilage damage (India ink retention grades 2 and 3), the histological lesions were also relatively mild or moderate and consisted of cartilage surface discontinuity with vertical fissures extending into the superficial, mid, or deep zones; occasionally, fissures extending into the calcified cartilage zone or the subchondral bone were also observed. Cell death was identified adjacent to the fissures, but chondrocyte proliferation was not appreciated in those areas. SO staining in areas of cartilage fibrillation was of variably decreased intensity, from slightly decreased to no staining at all (Figs. 5, 6). Lesions observed in the subchondral bone immediately below the articular cartilage were classified as mild and were characterized by fibrosis in the bone marrow spaces with occasional foci of cartilage islands. The amount and distribution of woven bone in the subchondral bone was considered abnormal in 3 cases with macroscopic cartilage damage classified as grade 3.
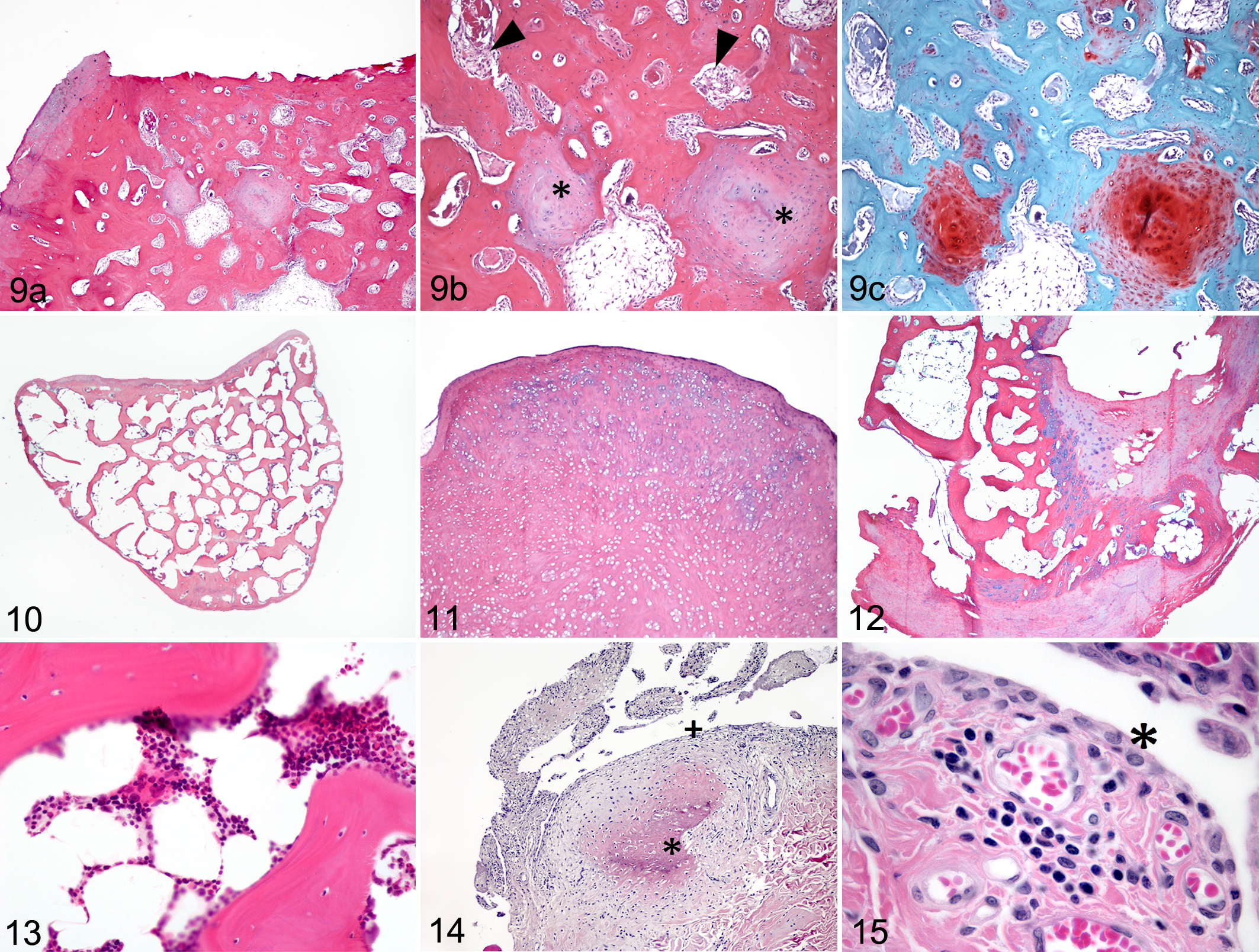
Cases with the most severe degree of macroscopic cartilage damage (India ink retention grade 4) showed complete ulceration, with hyaline cartilage matrix loss exposing the calcified cartilage zone or the subchondral bone to the intra-articular space (Fig. 7). Cell death was identified adjacent to the fissures and hypertrophic chondrocytes were occasionally seen adjacent to areas of severe cartilage fibrillation, but chondrocyte proliferation was not identified in those areas (Fig. 8). SO staining adjacent to the areas of severe cartilage fibrillation was severely decreased in intensity or absent in all cases. Changes in the subchondral bone (fibrosis/cartilage islands and/or woven bone) were present in all cases with grade 4 macroscopic cartilage fibrillation. Fibrosis and cartilage islands in the subchondral bone ranged from mild to severe. These areas appeared as discrete foci of hypertrophic chondrocytes embedded in the chondroid matrix (“cartilage islands”) and/or fibrovascular granulation tissue filling bone marrow spaces in close proximity to the exposed subchondral bone surface (Fig. 9). Replacement of mature lamellar bone by woven bone was detected by polarizing light in 8 of 18 cases with severe macroscopic cartilage damage, and in these cases, the articular surface was completely ulcerated and the subchondral bone exposed. Woven bone was always surrounding the areas of cartilage islands and bone marrow spaces that were filled with fibrosis.
Changes in the density of the subchondral bone were not appreciated. The tidemark was intact, single, and not crossed by blood vessels in any case, including those with severe damage of the articular cartilage.
Medial Coronoid Process
Visual inspection of the medial coronoid process did not reveal the presence of fissures in the cartilage, in situ fractured coronoid fragments, or free fractured fragments within the joint. In those joints in which intra-articular osteochondral fragments were present, the coronoid process was macroscopically intact. Microscopically, fissuring of the subchondral bone of the medial coronoid process was not identified in any cases, neither in cases with intact overlying articular cartilage nor in cases with severe cartilage damage. Subjective evaluation of cartilage thickness, osteocyte density of the subchondral bone, and bone porosity in the subchondral bone of the coronoid process was normal.
Relationship of Macroscopic and Microscopic Lesions Between Different Bones Within a Joint
Macroscopic cartilage damage scores (mean ± SD) using the India ink grading system were significantly higher for the ulna (2.1 ± 1.02; P = .0001) and the humerus (2.1 ± 1.05; P < .0002) compared with the radius (1.6 ± 0.5). No differences were found when the ulna and humerus were compared (P = .7) (Table 1). Macroscopic cartilage lesions were bilateral, and the degree of damage of the articular surfaces was similar in both elbow joints. The location of the lesions with the most severe cartilage fibrillation indicated the presence of disease in the medial compartment of the elbow joint with the articular surface of the medial coronoid process and the medial epicondyle of the humerus having the most severe degree of cartilage fibrillation.
Microscopic cartilage damage scores (mean ± SD) were significantly higher for the ulna (5.54 ± 4.3) compared with the radius (2.5 ± 2.6; P < .0001) and the humerus (3.8 ± 3.9; P < .0001). Microscopic cartilage damage scores were also significantly higher for the humerus compared with the radius (P = .007).
Intra-articular Osteochondral Fragments
A total of 16 intra-articular osteochondral fragments were evaluated grossly and histologically. Those fragments were found in 10 joints (affecting 6 different animals). The articular cartilage was ulcerated in at least one of the bones in all of those joints except in 2, in which the macroscopic cartilage damage was scored as 2 (mild cartilage fibrillation). Six joints had single fragments and 4 joints had multiple fragments. These fragments were either attached to the synovial membrane or free as intra-articular bodies. Macroscopically, the osteochondral fragments where white to pink, flat oval to round, and ranged from 3 to 6 mm (maximum length) (Figs. 2, 3). Microscopically, these fragments contained different amounts of well-organized cancellous bone with marrow spaces that occasionally contained hematopoietic cells. Some fragments also contained hyaline cartilage and fibrocartilage. Different stages of endochondral ossification were present in those areas of mixed tissue types. The outermost layer was commonly a thin layer of dense fibrous tissue. More commonly, a mixture of different tissue types was found, but occasionally fragments were exclusively of either fibrocartilage or organized trabecular bone (Figs. 10–13).
Synovial Membrane Findings
A total of 56 synovial membrane tissue samples were evaluated histologically (from 56 different elbow joints). Four samples from elbow joints of 4 different animals were not considered of appropriate quantity or quality for histological evaluation and were not graded. Overall, there was only mild inflammation in the synovium, very little synovial hyperplasia, and only weak correlation of synovial lesions with severity of macroscopic and microscopic cartilage lesions. Final synovitis scores of all samples evaluated ranged from 0 to 5 (maximum possible score = 9).
Synovial membrane samples considered normal (final score 0–1; n = 32) were characterized by normal synovial lining cell layer thickness, normal cellularity of the synovial stroma, and no inflammatory infiltrate present (Suppl. Table S2). The macroscopic cartilage damage score (the highest score of the 3 bones) of those joints with normal synovial membrane samples ranged from 1 to 4 (normal to severe cartilage fibrillation). Synovial membrane samples with the highest synovitis scores (4–5; n = 9) were characterized by moderate enlargement of the synovial lining layer (score 2), mild increase in density of resident cells (score 1), and mild inflammatory infiltrate (score 1). Inflammatory infiltrates consisted of lymphoplasmacytic micronodules located perivascularly in the synovial stroma (Fig. 15). The macroscopic cartilage damage score (the highest score of the 3 bones) of those joints with the highest microscopic scores for the synovial membrane samples ranged from 2 to 4 (mild to severe cartilage fibrillation).
The synovial lining was never ulcerated, and multinucleated cells were never seen in the synovial lining cell layer or in the synovial stroma, even in cases in which the subchondral bone was denuded of articular cartilage. None of the samples had inflammatory infiltrates graded as severe (score 3), and only 2 synovial membrane samples (joints from the same animal) had an inflammatory infiltrate graded as moderate (score 2).
Microscopic changes different from those evaluated for the synovitis severity score were observed. Chondroid metaplasia of the synovial stroma was identified in 2 cases. These areas appeared as micronodules of metaplasia of the hyperplastic synovium into cartilage, of varying stages of differentiation that seemed to undergo endochondral ossification to form bony nodules in some cases. These areas of metaplasia were not associated with inflammatory infiltrates (Fig. 14).
Synovitis severity scores were significantly but weakly and moderately correlated with the highest macroscopic (r2 = 0.3768; P = .0042) and microscopic (r2 = 0.4226; P = .0012) cartilage damage scores of the joints, respectively.
Discussion
Results of this study are the first description of the histopathological characteristics of feline elbow joints with and without macroscopic DJD lesions. Lesions were present bilaterally, and the ulna was the bone with the most severe degree of cartilage damage in both macroscopic and microscopic cartilage damage scoring systems. Cartilage lesions ranged from superficial fibrillation of the cartilage to complete ulceration with exposure of the subchondral bone. The most severe macroscopic as well as histological lesions of the articular surfaces were identified within the medial compartment of the elbow joint, specifically in the medial coronoid process of the ulna and the medial epicondyle of the humerus. Medial compartmentalization of the lesions in feline elbow joints has been documented macroscopically elsewhere, 2 and concentration of microscopic lesions in the medial part of the humeral condyle also has been documented. 28 Medial compartment elbow disease is well recognized in dogs as a result of elbow dysplasia (FMCP and OCD of the medial humeral epicondyle). 3,9,24 However, our observations did not reveal any of the features that are reported in dogs with a fragmented coronoid process (microcracks in the subchondral bone, increased porosity, and loss of osteocytes). 6,13 Histomorphometry was not performed in our study, but increased porosity and decreased osteocytes were seen only in the areas of microcracks of the subchondral bone in dogs, and microcracks were not present in our specimens. It is possible that fissures may have been missed during processing of the samples for histopathological evaluation. Nevertheless, since no evidence of FMCP or a histologic reaction to an adjacent microfracture was present in any of the specimens and fissuring or fracture of the coronoid process was not seen during macroscopic evaluation of any joints, we conclude that fragmentation of the coronoid process is not part of the pathogenesis of feline elbow DJD in the cases described in this study. Some of the changes observed in the subchondral bone in the samples evaluated in this study are similar to those described in the subchondral bone of the medial coronoid process from dogs with FMCP disease (cartilage islands and fibrosis of the bone marrow spaces). 13 These lesions are nonspecific responses of bone to a variety of insults and are not unique to FMCP. Unlike lesions in the canine coronoid processes, subchondral bone changes in the feline samples evaluated here were present only when cartilage erosion was so severe that the hyaline cartilage was ulcerated. In the canine study by Goldhammer et al, 13 hyaline cartilage was still present on the articular surface of the medial coronoid process in cases with cartilage islands in the subchondral bone. The cartilage islands within the subchondral bone lesions were likely secondary reactions to the disease that leads to medial coronoid fragmentation, unlike in our samples in which subchondral bone findings were likely consequence of the degree of cartilage degradation rather than pathology originating in the subchondral bone.
The cause of elbow DJD in cats with this pattern of medial compartmentalization is unknown. One of the theories proposed for the pathogenesis of FMCP in dogs is the presence of abnormal loading forces in the elbow joint resulting from asymmetric growth of the radius and the ulna, which causes increased loads in the coronoid process and subsequent fragmentation. Perhaps the same theory could explain why the lesions are concentrated in the medial compartment of the elbow joints in cats. However, further investigation will be necessary to elucidate why fragmentation of the medial coronoid process does not happen as a result of these theoretical abnormal loadings in feline species. One possibility is that cats do not have underlying lesions of OCD in their coronoid processes, since we did not see evidence of osteochondritis or OCD in any of the samples examined. A less likely possibility is that erosion of the cartilage of the medial coronoid process and medial humeral epicondyle is due to contact with the intra-articular osteochondral fragments, which were commonly located craniomedial in the elbow joint in close proximity to the coronoid process. However, this pattern of medial compartmentalization of the cartilage damage was also observed in joints without intra-articular osteochondral fragments, so this does not fully explain the pattern of cartilage damage observed herein.
Histopathological characteristics of the free intra-articular osteochondral fragments and changes observed in the synovial stroma (chondroid metaplasia and endochondral ossification) seem to indicate that those fragments originate from the synovial membrane and therefore are consistent with synovial osteochondromatosis secondary to DJD. Unlike primary synovial osteochondromatosis, in the secondary form, the intra-articular nodules are less numerous and often mixed with other forms of synovial proliferation and metaplasia, as well as with erosive changes in the articular cartilage that are more marked than is the degree of synovial proliferation, 22,25 which is consistent with our findings. A few cases of synovial chondromatosis in canine species are described in the literature, affecting shoulder, stifle, elbow, and tarsal joints. 1,7,8,10,14,30 Mention of feline synovial chondromatosis in the literature is scarce. In older publications, diagnosis was made based on radiographic findings without gross or histopathological confirmation. 16 In more recent reports, intra-articular mineralizations found in shoulder and elbow joints are referred to as “osteochondromas,” but macroscopic and histopathological characteristics are consistent with synovial osteochondromatosis as described in this study. 2 These intra-articular fragments may not be visible radiographically depending on their degree of calcification, and so it is possible that synovial osteochondromatosis with articular cartilage erosion may be present in some joints without radiographic evidence of DJD as has been published previously. 11
Severe synovial inflammation was not seen in any of the samples evaluated, and overall there was only mild inflammation in the synovium and very little synovial lining hyperplasia even in those elbow joints in which the articular cartilage was ulcerated. This suggests that the elbow lesions in our cases were not primarily inflammatory in origin. The joints with the most severe cartilage fibrillation tended to have the highest synovitis scores, but correlations of the degree of synovitis with macroscopic and microscopic cartilage damage scores were only weak and moderate, respectively. Goldhammer et al 13 reported the degree of synovitis in dogs with different degrees of cartilage fibrillation secondary to FMCP, and similar to our study, the synovitis scores were low, even in cases with ulceration of the articular cartilage. These results are consistent with synovitis scores reported by Krenn et al, 17 in which the mean synovitis score of patients diagnosed with osteoarthritis was only 2 (range, 0–6). It is not surprising, then, that ulceration of the epithelial lining of the synovial membrane or severe inflammatory infiltrate of the synovial stroma was not seen in our samples since these features seem to correspond only with reactive or rheumatoid arthritis. The degree of synovitis present in dogs with synovial osteochondromatosis has not been reported, but clinically these animals have pain on manipulation of the joints. If the degree of synovitis is mild, as we found in the feline samples, the source of pain in these patients may be coming from a source other than the inflamed synovial membrane.
Twenty-four samples considered normal macroscopically were found to be abnormal on histopathologic evaluation. The lesions observed histologically could be considered early changes in the process of cartilage degradation, before any abnormalities are detected on the cartilage surface. Initially, clefts deep in the hyaline cartilage without any superficial fibrillation were suspected to be processing artifacts, as has been suggested in other studies. 13 However, a decrease in the number of chondrocytes and a decrease in SO staining in those areas were also seen, and so the changes were considered real. These results are in agreement with a recent publication in which diffusion parameters (diffusion-weighted spin-echo magnetic resonance imaging sequences) were used to assess disease progression of the articular cartilage, and results suggested that collagen architecture in the deep cartilage is altered early in the process of cartilage damage. 27 These recent findings conflict with the current histopathological grading systems, which are based on the assumption that cartilage damage is initiated at the cartilage surface and propagates deeper into cartilage as osteoarthritis progresses. On the other hand, 10 samples evaluated were graded normal histologically but abnormal macroscopically (Indian ink was retained by the articular surface). In these cases, the area and the degree of ink retention was minimal, and it may represent only mechanical disruption of the articular surface rather than the result of altered collagen architecture and cartilage degradation. In addition, the areas of cartilage fibrillation were so small that it is possible that they were missed during processing.
In addition to subjective comparisons between the lesions present in elbow joints of our cats with lesions reported in other species, we used established scoring systems to grade the changes present in our samples of cartilage, bone, and synovium. After evaluation of articular surfaces that had lesions of varying severities, it was noted that some of the features used to differentiate severity grades in established grading systems were not present in our samples. The grading system by Mankin et al 21 considers features such as chondrocyte cloning, presence of pannus, or blood vessels crossing the tidemark as indicators of cartilage degradation, and these were not identified in the specimens we evaluated; also, the Mankin system does not evaluate subchondral bone changes. In the same way, the OARSI system 26 establishes grades of cartilage degradation using some features that could not be observed in the samples we evaluated (eg, cartilage edema, chondrocyte clustering), and even though this system included evaluation of changes in the subchondral bone, the changes to be evaluated also differed from our observations. For these reasons and since these systems have not been validated in feline species, we developed a scoring system relevant for this study that considered features observed in the specimens evaluated. The modification of the scoring system proposed here may be a useful reference for the evaluation of cartilage damage in other animal species for which the previously reported systems are not fully applicable as in feline joints.
On the basis of our results, we reject the hypothesis that elbow joints with macroscopic evidence of DJD and the presence of intra-articular osteochondral fragments have histological evidence of a fragmented coronoid process. The degree of synovitis was correlated with the degree of cartilage damage, but this correlation was weak or moderate, and overall the degree of inflammation of the synovium was mild, even in cases with hyaline cartilage ulceration. The presence of intra-articular osteochondral fragments in the elbow joint in cats is consistent with synovial osteochondromatosis secondary to DJD. Articular cartilage erosion is more severe in the medial compartment of the joint (medial coronoid process of the ulna and medial epicondyle of the humerus), for which no explanation has been identified. The lack of synovial inflammation even in cases with severe cartilage erosion could explain the previously reported absence of pain on manipulation of joints with radiographic signs of DJD in some cats. In addition, the presence of pain on manipulation of joints with DJD may not be explained by synovitis.
To our knowledge, this is the first report of macroscopic and histologic lesions of the elbow joint in cats, and even though our study was not designed to look at the prevalence of elbow DJD, we know from previous studies that feline elbow DJD is a condition that can be seen radiographically in 41% of cases. We believe this is an underestimation of the prevalence of this disease since most lesions of the cartilage seen grossly and histologically are grades 1 and 2 (mild/moderate), which will not be seen radiographically unless other degenerative changes are present in the joint, such as osteophytes. The most severe macroscopic as well as histological lesions of the articular surfaces were identified within the medial compartment of the elbow joint, and they occur without evidence of primary inflammatory disease, OCD, or FMCP. Cartilage damage ranged from superficial fibrillation to complete ulceration, and in the most severe cases, subchondral bone lesions such as cartilage islands and fibrovascular granulation tissue filling bone marrow spaces were identified. The degree of inflammation of the synovium was mild, even in cases with hyaline cartilage ulceration, and correlation with the degree of cartilage erosion was weak to moderate. Intra-articular osteochondral fragments found within the elbow joint were most consistent with synovial osteochondromatosis secondary to DJD. This is a common degenerative disease of the elbow joint in cats that has been overlooked, and the etiology is unknown.
Footnotes
Acknowledgements
We gratefully acknowledge the competent assistance of Mrs Monica Mattmuller of the Histology Laboratory of the Veterinary College of North Carolina State University for the preparation of the histological sections and special stains.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Comparative Pain Research Laboratory at North Carolina State University and a grant from Novartis Animal Health (Global Fellowship Program). Mila Freire was receiving salary support from Morris Animal Foundation during the preparation of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.