
Abstract
While thymomas are uncommon but well-known mediastinal masses, collagen-rich variants are exceedingly rare. Thymofibrolipoma and sclerosing thymoma tumor variants have been recently recognized in medical pathology, and thymofibrolipoma has been only rarely reported in dogs. A cranial thoracic mass was identified in a 6-year-old Labrador Retriever that was characterized by robust collagenous stroma dissected by thin cords of cytokeratin-positive neoplastic epithelial cells and bordered by mildly pleomorphic epithelial cells with occasional lymphocytic aggregates and rare Hassall corpuscles. To the authors’ knowledge, this is only the second report of thymofibrolipoma in veterinary medicine and the first to describe a variant with a mitotically active and relatively pleomorphic, adjacent thymic epithelial population.
A thymoma is an uncommon neoplasm defined as a neoplastic proliferation of thymic epithelial cells accompanied by a variably sized population of nonneoplastic lymphocytes (thymocytes) with a propensity for paraneoplastic syndromes. 3,9 The World Health Organization system of classification categorizes human thymomas primarily based on epithelial morphology and secondarily on lymphocyte content, ranging from the essentially benign type A to the early carcinoma-like type B3. 7 In humans, thymomas with abundant collagenous stroma are exceedingly rare and include the sclerosing thymoma, thymofibrolipoma, and thymic lipofibroadenoma. 7
Thymomas are uncommon in domestic animals but have been reported in a variety of species, with fewer than 33% of reported tumors considered malignant with respect to metastasis or local invasion. 3 Animals with thymomas may be asymptomatic, present with respiratory or cardiovascular dysfunction secondary to the mass effect, or present with thymoma-associated paraneoplastic syndromes, including but not limited to myasthenia gravis, hypercalcemia of malignancy, arrhythmias, and their sequelae. 1 In domestic animals, collagen-rich thymic masses are rare. Herein we report a case that, to our knowledge, represents only the second report of veterinary thymofibrolipoma.
Case History
A 6-year-old intact male Labrador Retriever was presented to the North Carolina State University College of Veterinary Medicine for treatment of a suspected thymoma. The mediastinal mass filled approximately 85% of the thoracic cavity and was initially discovered by the referring veterinarian when evaluating a complaint of labored breathing following a dog attack. No confirmatory diagnostics were performed before institution of therapy. Surgical removal was performed following failure of palliative radiation or prednisone therapy to elicit any change in the size of the mass over the course of 5 months as determined via repeated thoracic computed tomography. Paraneoplastic syndromes were not diagnosed, and the dog was negative for acetylcholine receptor autoantibodies.
Methods
Subsequent to surgical removal, the tissue was partially incised and submitted to the surgical pathology service in 10% neutral buffered formalin. Representative sections were trimmed, fixed, processed, sectioned at 5 μm, and stained with hematoxylin and eosin for histologic examination. Immunohistochemistry was performed on serial sections with a polymer-based method (EnVision Kit, Dako, Carpenteria, CA) employing the following primary antibodies: cytokeratin AE1/AE3 (N1590, Dako, 1:50 dilution), CD79a (M7051, Dako, 1:50 dilution), and CD3 (A0452, Dako, 1:150 dilution). For positive controls of cytokeratin, canine skin was used, and a lymph node was used as a positive control for the cell surface markers. For negative controls, normal mouse serum was substituted for the cytokeratin and CD79a primary antibodies and rabbit serum for the CD3 antibody.
Gross and Histologic Findings
The 1.78-kg mass was submitted as 7 round to irregular, tan, firm lobules ranging from 4 cm in diameter to 20 × 15 × 6 cm (Fig. 1). All sections were similar and exhibited an unencapsulated, heterogeneous mass composed of neoplastic epithelial cells embedded within abundant collagenous stroma centrally and forming thymus-like aggregates peripherally (Fig. 2). Centrally, approximately 80% of the mass comprised exuberant, dense, paucicellular, fibrous connective tissue with variably sized bundles of both fine and coarse collagen fibers with rare individual or clustered adipocytes (Fig. 3). These collagen pseudolobules widely separated the embedded trabeculae of epithelium, characterized by polygonal to elongate epithelial cells with indistinct cell borders, with a mild to moderate amount of pale eosinophilic cytoplasm, and with an oval, finely stippled nucleus with 1 to 2 prominent nucleoli. Centrally, there was minimal epithelial pleomorphism and zero mitotic figures observed. In contrast, the peripheral aggregates of epithelial cells exhibited mild anisocytosis and anisokaryosis with 15 mitotic figures observed in 10 high-magnification fields (400×) (Fig. 4). These peripheral aggregates appeared organotypic, or thymus-like, due to the admixture of low to moderate numbers of lymphocytes and rare Hassall corpuscles. The loosely scattered lymphoid population varied from zero to approximately 50% of cells within a given 400× field and occasionally formed de novo follicle-like clusters.
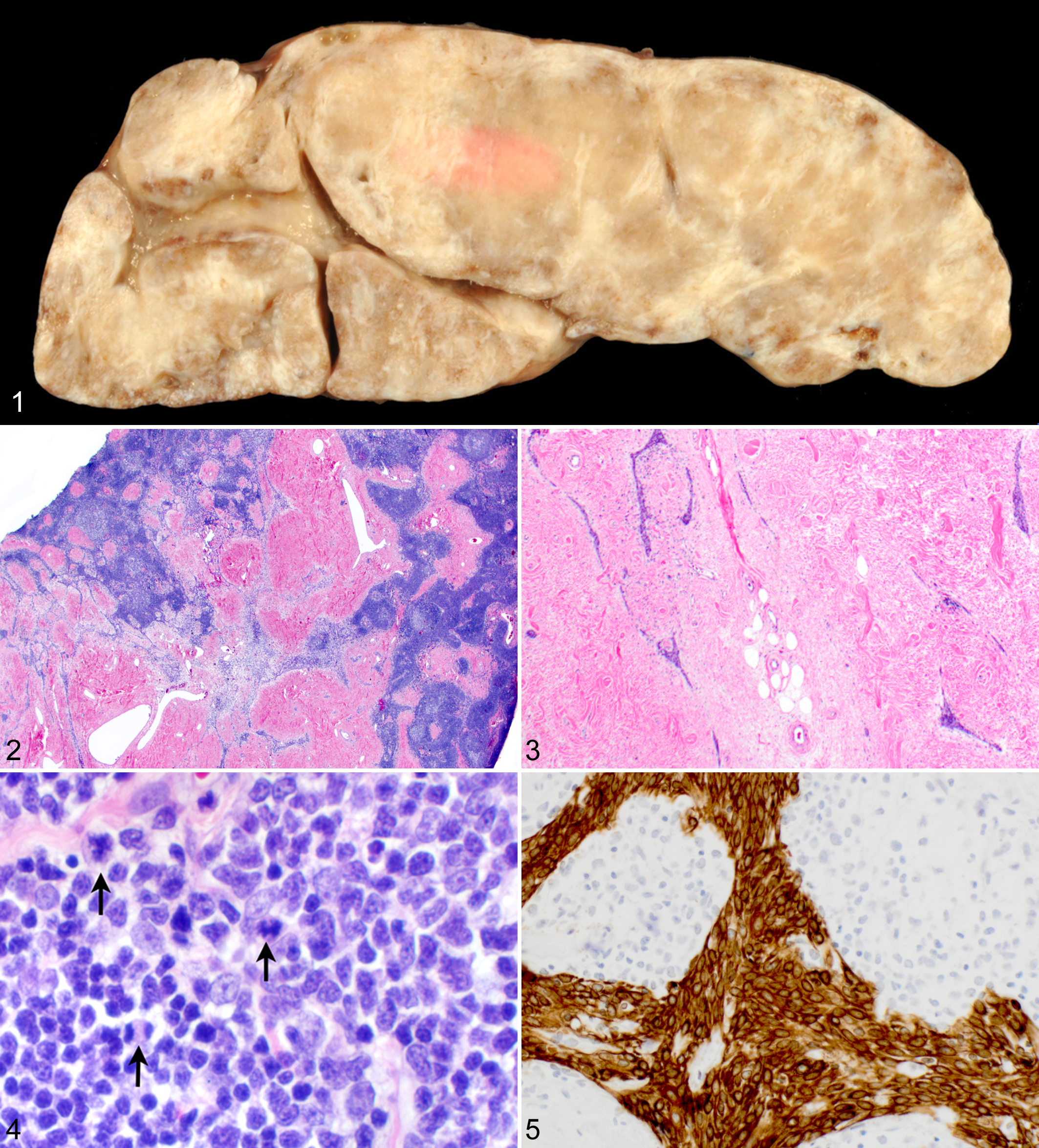
Thymofibrolipoma; dog. The very firm multilobular mass exhibits abundant tan-gray mottling on cut surface. Approximately 72 hours postfixation with 10% neutral buffered formalin.
Immunohistochemistry
Approximately 100% of the polygonal to elongate epithelial cells within the thin trabeculae and within the peripheral organotypic aggregates had strong, diffuse, cytoplasmic to membranous expression of cytokeratin AE1/AE3 (Fig. 5). The low to moderate numbers of admixed lymphocytes exhibited strong, cytoplasmic to membranous expression of either CD79a (50%) or CD3 (50%). Those lymphocytes noted to form follicle-like clusters were predominantly those exhibiting CD79a immunoreactivity. The positive and negative controls labeled appropriately.
Discussion
The pattern of collagenous lobules separated by strands of thymic epithelium with a rare fatty component is consistent with a thymofibrolipoma. 7 Thymofibrolipomas have previously been described in a male mixed-breed dog and spayed female pit bull terrier. 6 First described in people by Moran et al in 1994, a thymofibrolipoma is considered a fibrous variant of the benign, slowly progressive thymolipoma. 5 Thymolipomas, which are characterized by abundant adipose with a minor component of interspersed thymic tissue, have been reported in 1 male domestic shorthair cat and 1 spayed female miniature pinscher. 8,10 A clear distinction is not evident between a thymofibrolipoma and a thymic lipofibroadenoma. The latter was first described by Kuo et al in reporting a mass arising from an adjacent thymoma. 7 Interestingly adding to the variation observed within thymic tumors, 2 thymomas have been reported recently with abundant intratumoral amyloid deposition in a spayed female Himalayan and male domestic cat. 2
In the previously reported cases of thymofibrolipoma and thymolipoma, a normal thymic remnant bordered the mass without evidence of proliferation described. In our case, the bordering tissue resembles thymus due to the aggregation of the epithelial and lymphoid cells; however, the epithelial population exhibits relatively increased pleomorphism and a markedly elevated mitotic rate. This unexpected feature prompted consideration of sclerosing thymoma. Sclerosing thymomas are a variant of thymoma characterized by abundant collagenous stroma. 7 The largest human case series of sclerosing thymomas consisted of 4 women and 6 men ranging from 27 to 73 year olds. 4 Consistent with the typical spectrum of thymoma-associated presenting complaints, 5 patients were asymptomatic, 4 exhibited shortness of breath or chest pain, and 1 presented with myasthenia gravis. This case series refuted initial proposals that the fibrous component was due to tumor regression. In our case, no hemorrhage, necrosis, or pigment accumulation was noted to suggest a component of tumor regression. Ultimately, after consultation with acknowledged expert medical pathologists in human thymic neoplasia (A. Weissferdt, personal communication), a final diagnosis of thymofibrolipoma was reached.
Though rare, thymofibrolipoma should be considered in the differential diagnoses for a canine mediastinal mass. Furthermore, caution may be warranted before an inappropriate diagnosis of a typical thymoma or even thymic carcinoma due to the presence of proliferative foci adjacent to a stromal-rich thymic mass. The heterogeneity of thymic masses is paramount when considering tissue sampling and evaluation, especially antemortem needle biopsies, as the available tissue may not be wholly representative of the mass. At this time, a grading scheme is not yet applicable to stromal-rich variants in human or veterinary medicine. Due to the scarcity of these thymic masses, additional cases are necessary to better assess tumor behavior in dogs, cats, and humans and to determine if thymofibrolipoma, thymolipoma, and even sclerosing thymoma may represent a phenotypic spectrum or if they are distinct entities.
Footnotes
Acknowledgements
We thank Annikka Weissferdt, MD, FRCPath, assistant professor in the Department of Pathology at MD Anderson Cancer Center, Houston, Texas, for her consultation.