
Abstract
Neoplastic diseases are typically diagnosed by biopsy and histopathological evaluation. The pathology report is key in determining prognosis, therapeutic decisions, and overall case management and therefore requires diagnostic accuracy, completeness, and clarity. Successful management relies on collaboration between clinical veterinarians, oncologists, and pathologists. To date there has been no standardized approach or guideline for the submission, trimming, margin evaluation, or reporting of neoplastic biopsy specimens in veterinary medicine. To address this issue, a committee consisting of veterinary pathologists and oncologists was established under the auspices of the American College of Veterinary Pathologists Oncology Committee. These consensus guidelines were subsequently reviewed and endorsed by a large international group of veterinary pathologists. These recommended guidelines are not mandated but rather exist to help clinicians and veterinary pathologists optimally handle neoplastic biopsy samples. Many of these guidelines represent the collective experience of the committee members and consensus group when assessing neoplastic lesions from veterinary patients but have not met the rigors of definitive scientific study and investigation. These questions of technique, analysis, and evaluation should be put through formal scrutiny in rigorous clinical studies in the near future so that more definitive guidelines can be derived.
Keywords
The pathology report provides critical information that ultimately guides clinicians' decisions in determining optimal management of the cancer patient. Successful exchange of information requires an integrated relationship and open communication between the diagnostic pathologist and clinician/oncologist. Transfer of information begins with sample submission where communication is provided both verbally on the submission form and nonverbally via tissue demarcation. This information significantly affects gross specimen tissue trimming, which ultimately determines the areas evaluated microscopically by the pathologist. Other information provided, including signalment, anatomic location, lesion description, and lesion progression, may affect the histopathological diagnosis and prognostic information. In addition to providing the most accurate diagnosis possible, the report should furnish the clinician with parameters that may predict biological behavior when applicable, such as tumor grade, mitotic index, assessment of vascular invasion, and a detailed margin description. These parameters are important for the oncologist to make informed decisions but are often not reported, possibly because of inappropriate sample submission or simply omission by the pathologist.
This consensus paper establishes a standardized approach to tumor biopsies by providing recommended guidelines for sample submission, tissue trimming, margin evaluation, and reporting. These guidelines were developed through an initiative of the American College of Veterinary Pathologists' Oncology Committee and have been reviewed and endorsed by the World Small Animal Veterinary Association. The guidelines are not mandated but rather have been established to assist the primary veterinarian, oncologist, and veterinary pathologist optimize their roles in managing the veterinary cancer patient.
Sample Submission
An optimal pathology report begins with the submitting clinician. Appropriate handling of the specimen from time of acquisition until it arrives at the laboratory is essential to maintain proper tissue preservation and prevent unwanted tissue artifact or autolysis, which could preclude diagnostic evaluation entirely. The quality of the microscopic evaluation and interpretation is further dependent upon the information provided by the clinician, both verbally on the submission form and nonverbally via images and tissue demarcation (ink, sutures, other).
Sample Fixation and Packaging
Specimens should be placed in 10% neutral buffered formalin (NBF) directly following surgical excision unless tissue manipulation, such as inking or suturing, is required. These procedures should occur as soon as possible but at most within 30 minutes of excision to limit tissue artifacts. Detailed information on tissue demarcation is presented in the section titled Identification of Surgical Margins. Select tissue types (eg, eyes, testes) may benefit from fixation in other fixatives (eg, modified Davidson’s or Bouin’s solution). Check with the laboratory for specific fixation recommendations.
Containers for sample submission are often provided by individual diagnostic laboratories and should be used when possible. The following guidelines are recommended for containers used for routine biopsy submissions: An appropriately labeled wide-mouthed, plastic container containing no more than 1 liter of 10% NBF at a 1:10 tissue/formalin volumetric ratio. The lid should be secure and sealed to prevent leakage. The jar neck should be wider than the specimen being submitted. Whereas fresh tissue is malleable, formalin-fixed tissue is rigid and difficult to manipulate through a narrow opening. Glass is not recommended given the increased likelihood of breakage in transport. The container should be placed in a secured sealed plastic bag (eg, a commonly available food storage bag) to contain any leakage during shipment and should be surrounded by absorbent packing material. To avoid tissue freezing artifact in very cold environments, an insulated shipping container should be used or isopropyl alcohol added to the formalin fixative (1 part alcohol to 10 parts formalin). Of note, clinics should be cognizant of the carrier’s shipping restrictions and regulations, since the shipper, and not the receiving laboratory, is responsible for any problems. For oversized specimens (eg, amputated limbs, spleens), overnight shipping of the entire prerefrigerated fresh tissue sample using ice packs or other cooling materials will help to avoid autolysis. Do not freeze the specimen, and do not ship on dry ice, which may induce substantial artifact. Oversized items can also be prefixed for 48 to 72 hours, double-bagged, and shipped chilled without submersion in formalin. Partial parallel incisions approximately 1 cm apart (“bread loafing”) to facilitate fixation should be made through the mass without compromising tissue orientation or margins. Samples too large to fix on site as a whole can be sectioned into portions and submitted in separate appropriately labeled formalin jars. An annotated digital image or sketch of the original specimen to depict sectioning and orientation should accompany the samples. Additionally, a single portion of the specimen can be submitted for tumor diagnosis but this will preclude margin evaluation. Remaining tissue should be held at the clinic until the final pathology report is received. Very small samples, such as endoscopic or pinch biopsies, should be placed in screen cassettes labeled with a #2 pencil, if necessary, and then put in a formalin container for shipping. Do not use gauze sponges or cardboard because tissue may become compromised upon retrieval. Very small samples may, at times, yield insufficient artifact-free sections for diagnosis; therefore, submission of multiple specimens from a single lesion is preferable. For luminal organs (eg, intestine, uterus, large vessels), flush the intact lumen with formalin. For long sections of luminal tissues, either a partial longitudinal incision can be made while leaving areas of interest (eg, resection sites, mass) intact, or 3 labeled sections (cranial/proximal, mass and caudal/distal) can be submitted. Thin flat samples (eg, urinary bladder, stomach, diaphragm) should be placed in a tissue cassette with a foam pad to minimize tissue curling. Larger samples can be tacked onto a flat piece of cardboard presoaked in formalin or water with suture through edges of tissue not needed for examination. Staples are not recommended because they are difficult to remove without destroying tissue. Needles should not be used at any time, because this is hazardous to laboratory personnel handling tissue specimens. Draining lymph nodes associated with limb amputations warrant microscopic evaluation but may be difficult to identify postoperatively. To ensure evaluation, the submitting clinician should consider dissecting the node perioperatively and submitting it with the limb in a separate, appropriately labeled container.
Shipping of specimens can be complicated when dealing with very small or very large tissue samples that cannot be sent routinely. If there is uncertainty how to submit a specimen, contact the respective laboratory for guidance. The following guidelines address these issues:
Submission forms and any additional paper documents should be sent concurrently but should be placed in a separate plastic bag (or compartment) for protection from potential formalin leakage. All sample containers (not lids) should be labeled with a unique patient name/case number and tumor site (or number, if submitting multiple masses from a single patient). The same information should also be included on the submission form. When multiple tumors from a single patient are submitted, each mass should be placed in an individual jar or uniquely identified (eg, blue suture = right lateral thorax) if included in the same jar. Written information relative to any tissue demarcation should be included on the submission form for each respective mass. A gross description is unreliable to differentiate tumors placed in the same jar, as these characteristics (ie, size, color, texture) change upon formalin fixation. All masses excised from a patient should be submitted for histologic examination, regardless of the number of tumors found or the preliminary results of cytologic examination. For example, multiple mammary tumors might have different tumor types with different prognoses, so all should be submitted.
Tissue shrinkage subsequent to formalin fixation does occur. 4,13 For cutaneous biopsies, shrinkage can be as much as 30%. 5,13 Tissue shrinkage is also associated with inherent postexcisional tissue retraction as well as dehydration steps during processing. These changes may result in reported surgical margins that seem to be significantly less than the surgeon believed were obtained at the time of surgery.
Information Provided by the Clinician
Submission form
The submission form is mandatory since it is the essential communication piece between the clinician, laboratory personnel, and pathologist. Submission forms are commonly available from the pathology laboratory and are often available on-line. The submission form should be typed or computer generated, if possible, and should contain patient information including, but not limited to, the following Signalment (age, sex, reproductive status, and breed) Lesion-specific clinical history (eg, anatomic site, date first noticed, rate of growth) Potentially lesion-associated clinical signs (eg, lameness, vomiting) Type of lesion (eg, new lesion, recut following incomplete excision, excisional biopsy following previous incisional biopsy, local recurrence) General clinical history—previous neoplastic diseases, previous or current nonneoplastic conditions of relevance Treatment history—local and systemic, current and previous (eg, chemotherapy, radiation, corticosteroids) Previous unrelated treatments or potential tumor-inducing historical events at tumor site (eg, previous radiation, vaccination, implants) CBC, biochemical, and hormonal (eg, hyperinsulinemia) abnormalities Results of prior lesion-associated diagnostic tests—cytology, prior biopsy reports, imaging (radiographs, ultrasound, magnetic resonance imaging, computed tomography); access to radiographs may be especially important for bone and gingival tumors.
The submission form should also provide a working clinical diagnosis and/or list of differentials as well as a thorough gross lesion description, descriptions of any iatrogenic tissue markings (eg, ink, sutures), and an indication whether the submitted sample is an incisional or excisional biopsy. Excisional biopsy indicates assessment of surgical margins is necessary, whereas for incisional biopsies the margin evaluation is null. Anatomic site should be thoroughly described, such as “dermal/subcutaneous mass of the left anterior carpal region” instead of “leg mass.” Concurrently, location can be notated on a provided animal diagram and/or shown with digital images. Features appreciated during diagnostic imaging or perioperatively should be described, including the tissues involved or associated with the mass (eg, thyroid mass invading subjacent skeletal muscle).
When submitting multiple masses, a clear indication of the number of masses submitted and their respective anatomic locations can be achieved by using a numbered list (ie, mass 1, mass 2). Lists are not necessary for multiple pinch biopsies of a single mass.
Identification of surgical margins
At times, assessment of surgical margins may be more desirable information for the clinician than the diagnosis itself. 7 Assessment of surgical margins is the best determinant of adequate surgical treatment, and completeness of surgical excision is one of the best predictors of treatment outcome. The surgical margin is any region of the biopsy specimen that was adjacent to or contiguous with tissue that remains in vivo. Primary means of indicating surgical margins on tissue specimens include the application of surgical ink and/or placement of sutures. It remains imperative that a corresponding written explanation of these tissue demarcations be provided. An example might be “yellow ink denotes the deep margin and black ink denotes the lateral margin.” An example using sutures could be “1 suture is dorsal and 2 sutures are cranial.”
There are 3 basic reasons to use ink on submitted tumor samples: (1) to orient samples, allowing specific margins to be referred to in the report; (2) to visibly identify all surgical margins at the time of gross and microscopic evaluation; and (3) to denote areas of greatest concern. It is recommended that clinicians ink margins before submission since they performed the surgery and can best identify these areas. Additionally the tissue has not yet been altered from fixation. Inking can be performed by laboratory trimming personnel, but this approach is less ideal. The following are guidelines for appropriately inking tissues. Inking before fixation is recommended but may also be done after formalin fixation. Postfixation artifacts (shrinkage, conformational changes) may alter true margins. Inking must be performed with official surgical ink or waterproof drawing ink to ensure retention and persistence throughout tissue processing (Fig. 1a)
The tissue is placed on absorptive material and blotted dry prior to inking, whether before or after formalin fixation. A cotton swab or wooden applicator stick should be used to place ink only on regions that are of specific interest or true surgical margins (Fig. 1b and c). In most instances, it is preferable not to submerge the whole sample in ink. Inking should occur as soon as possible, within 30 minutes of excision at most. To prevent ink from washing off or coating insignificant areas, the ink must dry completely (approximately 5–10 minutes) prior to placing the tissue in formalin. For larger specimens that require bread loafing, tissue should be inked first, allowed to dry, and then cut to prevent ink from permeating insignificant areas. Surgical ink is available in multiple colors. Black, yellow, and green are typically preferred because blue and red may be difficult to assess in the face of hematoxylin and eosin stains. Colors are visualized on histopathologic examination (Fig. 1e and 1f) and used by the pathologist for orientation when writing the final report.
Sutures can be used to demarcate surgical margins, orient tissue for trimming, or denote particular tumors when multiple samples are submitted in a single formalin jar. Identification, as presented by the clinician on the submittal form, is either by suture number (eg, 1 suture in the dermal mass from the muzzle, 2 sutures in the dermal mass from the lateral thorax) or by color (eg, blue suture is dermal mass from muzzle, purple suture is dermal mass from lateral thorax). Avoid describing suture material (eg, prolene, vicryl, silk, braided, other) since laboratory personnel may not be familiar with these terms.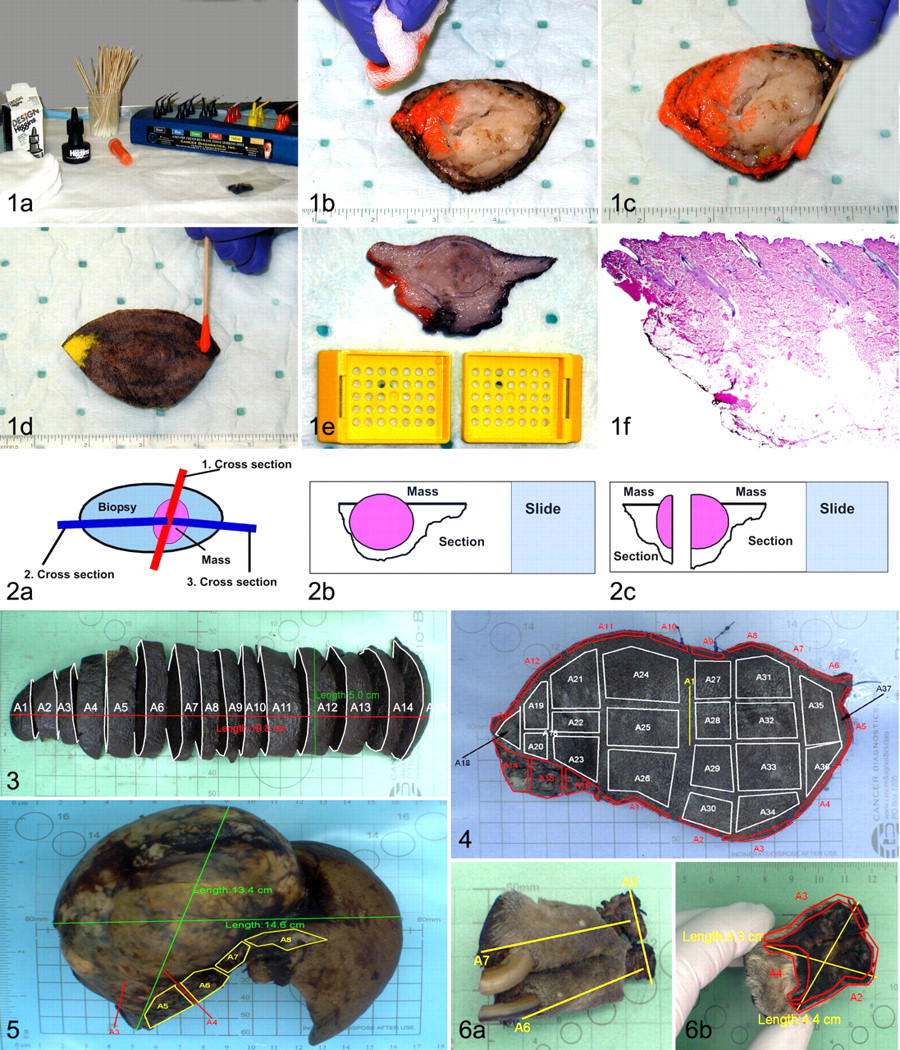
An alternative to inking or using suture to denote surgical margins is to obtain tissue from the tumor bed, the in vivo tissue that was adjacent to or contiguous with the excised specimen. Microscopic evidence of neoplastic cells in this tissue indicates the presence of residual disease in the patient. If specific regions of tumor bed are clinically relevant, each area should be submitted in a separate, appropriately labeled formalin jar. If a 1:10 tissue to formalin ratio is maintained, tumor bed specimens may be submitted in appropriately labeled red-top blood collection tubes. The collection method (eg, tumor bed) and corresponding information for each specimen should be included on the submission form.
Trimming
Critical assessment of gross samples by laboratory personnel prior to trimming will result in a more reliable and meaningful interpretation of histologic slides by the pathologist. Trimmed areas should include tissue for tumor diagnosis and margin evaluation. There are many techniques to section a tumor sample, so it is best to develop a routine approach within a diagnostic facility. A routine approach helps to standardize surgical margin assessment and intralaboratory reporting when there are multiple individuals trimming and multiple pathologists within a laboratory. A standardized interlaboratory approach creates more consistent reporting and helps comparison across published studies. It is advised that clinicians be familiar with the approach used by their laboratory.
Trimming Methods
Reviewing all trimming methods in the literature is beyond the scope of this article. There are a few routinely used techniques that are commonly used in diagnostic laboratories, with each possessing advantages and disadvantages. Their brief review is warranted. Cross-sectioning (radial method, “halves and quarters”) is the most commonly used method for the first-time removal of small or moderately sized masses (Fig. 2a). The tumor is bisected along its shortest axis (Fig. 2b). Then, each half of the tissue is bisected through its longest axis, creating quarter sections that demonstrate the mass in a different plane (Fig. 2c). Disadvantages are (1) erroneous assumption of symmetrical expansile growth of the mass and (2) evaluation of a very limited portion of the margin tissue. Parallel slicing at regular intervals (complete bread loafing, serial sectioning) increases the percentage of marginal tissue examined (Fig. 3). Although this approach is common in human medicine, the cost of the approach may be limiting in veterinary medicine. The modified technique combines radial and parallel techniques. Parallel sections are taken through the mass at regular intervals, with the remaining ends bisected into quarter pieces per the radial technique. This allows for evaluation of tissue immediately adjacent to the bulk of the tumor and evaluation of some distant margins of the sample. Tangential sections (shaved edge sections, “orange peel”) are used to evaluate the surface area of the surgical margin. The method is most commonly used in human medicine for specific tumors (Fig. 4).
18
Multiple 2- to 3-mm sections are shaved off the edge of the sample and laid into cassettes with the cut surface down. Any tumor present in the sections is interpreted as incomplete excision. This method offers complete margin evaluation (eg, all margin areas are evaluated). The disadvantage is that the objective margin measurement (margin distance) cannot be assessed. Tumor bed technique, as discussed previously in the Identification of Surgical Margins section, is an alternative method to evaluating margins but is dependent on the clinician submitting the appropriate tissue samples. Identification of any neoplastic cells in sections is consistent with incomplete surgical excision. If devoid of neoplastic cells, an objective margin measurement cannot be determined.
Trimming of Specialized Tissues
Tumors can arise in sites that either require additional steps for appropriate trimming or require additional sectioning because of site-related concerns. The following guidelines offer suggestions to address these situations. Bone marrow core biopsy: A modified short decalcification step before processing without any trimming may be necessary. Eyes: Globes should be submitted whole without prior sectioning so that shape is maintained. Orbital tissue and adnexa should be removed prior to fixation unless directly involved with the tumor and representing surgical margins. Alternatively, these tissues can be submitted separately to assess surgical margins. Suspected location of a mass within the globe can be drawn, described, or marked with surgical ink or sutures on its exterior, taking care not to penetrate the globe. At trimming, the initial cut should be made immediately adjacent to the optic nerve in a caudal to dorsal direction. If the location of a mass or area of interest is known, the globe is bisected using anatomic landmarks placed by the clinician so that the incision will traverse through the area of interest. If a specific site of interest is unknown, the eye should be bisected on a central dorsoventral plane that allows for evaluation of dependent and nondependent areas of the globe. If specific sites, including masses, are not approximated by this first incision, additional sectioning of the remaining globe is performed. Note that tumor invasion is most common at the limbus and optic nerve. Skeletal tumors (eg, limb or tail amputation, mandibulectomy): Evaluate both soft tissue and bone at the proximal margin. Trim soft tissue from bone sections after inking (if necessary) while keeping track of orientation. Bone can also be inked prior to decalcification. If surgical margins are wide, a cross-section can be cut through the proximal bone and distal bone as appropriate as well as a cross-section through the area of concern (eg, tumor) to show both bone and any surrounding tissue. If margins are close (as in many mandibulectomy/maxillectomy cases), multiple sections oriented perpendicular to the surgical plane can be used to evaluate a larger percentage of the surgical margin and allow the pathologist to report margin distance. Other areas of the sample should still be surveyed for margins, but in less detail. Parenchymal tumors (spleen, kidney, liver, thyroid gland, lung, brain): Tangential sections along the surgical margin are adequate if wide margins are present, whereas multiple perpendicular sections offer better detail when margins appear close (Fig. 5). Surgical margins are often difficult to identify after fixation, so tissue inking by the submitting clinician is most valuable. For splenic tissue, multiple sections may be required for tumor identification, including sections of normal appearing tissue adjacent to nodular lesions. Digital masses: Routine sections should include the most proximal soft tissue and bone sections in a cross-sectional plane at the amputation site (Fig. 6). A complete longitudinal or sagittal section, including bone, nail, and nail bed, is necessary to evaluate the site of tumor origin (eg, nail bed vs haired skin) since this can be predictive of biological behavior for melanomas and squamous cell carcinomas of the digit. Luminal tissues (intestine, uterus, etc): Cross-sections (or multiple perpendicular sections) at the resection sites for margin evaluation and an additional section through the gross tumor for tumor diagnosis.
Consensus Recommendations
Putting forth a blanket recommendation on how every tumor biopsy specimen should be trimmed is impossible because each specimen is unique. Specimen size, overall margin area, tumor type, and potential financial restrictions should be considered. Therefore, it is recommended that both pathologists and clinicians understand the various trimming methods and associated advantages and disadvantages. Additionally, scientific evidence does not currently exist in the veterinary literature to support the superiority of one technique over another.
We do agree that the greater the percentage of marginal tissue evaluated, the greater the confidence that this evaluation reflects the surgical margin overall. Thus, radial sectioning alone, which evaluates minimal margin tissue, is least favored for margin evaluation. A combination of either radial and parallel sectioning or radial and tangential sectioning is recommended. A consensus regarding an optimal technique for margin evaluation could not be reached, despite much debate, given the absence of scientific support in this field. However, there was a consensus that studies are needed to determine the most suitable techniques to evaluate margins for specific tumor entities.
A combination of cross-sectioning (radial method) and tangential sectioning for tumor margin assessment of cutaneous and subcutaneous neoplasms will allow the pathologist to evaluate the tumor, to provide complete surgical margin assessment (circumferential and deep), and to provide numeric measurements of margins for the radial sections (Figs. 2 and 4). However, tangential sections, when free of neoplastic cells, can at best only indicate that the margin is at least 2 to 3 mm. In contrast, bread loafing of tumors using at least 0.5- to 2.0-cm intervals (based on the longest dimension of the gross tumor) will provide more detailed information regarding the numeric margin distance of a tumor. This parallel sectioning will not achieve complete margin evaluation. Ideally, the client should be provided with an image showing the assessed margin fields to easily communicate which areas of the tumor were incompletely resected (Figs. 4–6).
For neoplasms of lobated internal organs (lung or liver) and all pendulous neoplasms, tangential sectioning through the point of origin or the point of surgical excision should be performed for margin evaluation (Fig. 5) in addition to radial sectioning of the mass. For digits, cross-sectioning through the proximal bone for margin evaluation and longitudinal sectioning through the length of bone to investigate bony involvement should be performed (Fig. 6) in addition to radial sectioning of the mass. For jaw neoplasms, tangential sectioning through the cranial and caudal bone for margin evaluation should be performed in addition to radial sectioning of the mass. For luminal tissues (intestine, uterus, etc), cross-sectioning at the organ ends should be performed for margin evaluation in addition to perpendicular sectioning of the mass.
The vast differences in circumstance that accompany each sample do not allow for rigid standardization of technique across all laboratories or for all tumor types. Awareness of the different techniques with their associated benefits and limitations is recommended. Documentation of the trimming method used should be provided in the pathology report, either verbally or, ideally, by an associated annotated image. When conducting prospective studies, within or across institutions, a standardized trimming method should be used to maintain consistency of results.
Microscopic Evaluation and Reporting
The finalized pathology report is the essential document from the pathologist to the clinician which impacts the patient’s prognosis and ultimately directs the therapeutic plan. This section provides recommended guidelines for the microscopic evaluation and reporting of tumor biopsy specimens with the ultimate goal of improving communication with, and information provided to, the veterinary oncologist/clinician. Report components should include the diagnosis (with grade when applicable), microscopic description, comments/remarks, and references where applicable. Ideally, an indication of the samples received and a gross specimen description, or digital image, should also be provided. Report format/organization should be consistent within a given laboratory and easily interpretable.
Microscopic Diagnosis and Grade
A microscopic diagnosis should be clearly visible and provided on all final pathology reports. The diagnosis may be an initial diagnosis (eg, incisional biopsy) or confirmation of a previous diagnosis (eg, wider surgical margins from previous incomplete excision). If a definitive diagnosis is pending, the “Comments” section of the preliminary report should indicate which tests are still pending (eg, additional sections, decalcification, special stains). The report status (eg, preliminary, final, addendum) should always be indicated on the report.
When a definitive diagnosis cannot unequivocally be determined on routine hematoxylin and eosin (HE) evaluation, a presumptive diagnosis or differential diagnoses should be provided and additional diagnostic tests recommended, such as histochemistry, immunohistochemistry (IHC), or polymerase chain reaction (PCR). If a diagnosis cannot be rendered (eg, nondiagnostic sample), the reason should be provided in the comments (eg, tumor tissue not observed in examined sections, inadequate sample size, tissue artifact precludes diagnosis). For multiple samples, a list of diagnoses should be reported based either on anatomical site or on the sample list submitted by the clinician.
When applicable, tumor grade should follow the diagnosis (eg, mast cell tumor, grade III). Tumor grade predicts biological behavior and is based upon published grading criteria. The respective references should be provided in the reference area of the “Comments” section. The references may serve as a resource to assist the clinician with case management. If a clinician/oncologist requests a “grade” on a lesion for which no published veterinary data exist, the pathologist may honor the request based on clinician-provided criteria but should also include a comment appropriate to the case, such as, “grading of this tumor is not supported by data,” “grading is extrapolated from the literature of similar tumors in humans,” or “grading is anecdotal.” For cases where there is inadequate tissue to accurately evaluate grading criteria (ie, needle biopsy), tumor grade may be precluded.
Microscopic Description
Components of the microscopic description may vary relative to the particular lesion but should include the salient features supportive of the diagnosis. If this description is read by another pathologist, the diagnosis should be attainable from the description alone (eg, junctional change for melanoma, osteoid for osteosarcoma, sheets of well-differentiated adipocytes for lipoma). Similarly, when grading malignancies, the criteria evaluated when determining that grade per published data should also be described (eg, mitotic index, cellular differentiation, invasion). The description should be written in a clear and concise manner.
Descriptions of benign lesions may not have as many reported parameters as malignancies, but features that support the lesion diagnosis should still be reported (eg, well demarcated or encapsulated). This may be the only means of relaying to the clinician, or perhaps a second-opinion pathologist, what features were observed to support the diagnosis. Surgical margins should also be reported but may not require the same amount of detail as for malignancies (addressed below in the section titled Margins).
As mentioned, when tumor grade is applied to a malignancy, the features evaluated to arrive at that grade should be described. However, meaningful tumor grades have not been established for all tumors. In these cases, the microscopic features affecting biological behavior are unknown. At best, pathologists and oncologists can only speculate on behavior based on knowledge of how similar features affect the biological behavior of other tumor types. Parameters that may be reported in either malignancies lacking established grading criteria or malignancies with a degree of atypia precluding definitive diagnosis include tissue invasion, cellular and nuclear pleomorphism, degree of anisocytosis and anisokaryosis, nucleolar features, mitotic index, necrosis, and vascular invasion.
Mitotic index
Mitotic index is the number of cells observed in mitosis in an indicated number of microscopic high-power (400×) fields (hpf). The mitotic index should be reported as the absolute number of mitotic figures (MFs) per number of evaluated 400× fields; ideally, a minimum of 10 hpf should be examined. When dealing with small tissue samples (eg, needle biopsies), MFs should be reported as the absolute number of MFs per total hpf evaluated (eg, x MFs per 6 hpf), and the report should include a comment describing the limited tissue sample. Evaluated fields should consist of densely cellular neoplastic tissue. Avoid areas with extensive hemorrhage, necrosis, or cellular paucity. Evaluation should focus on fields with the highest mitotic activity as determined by a low-power scan. When publications demonstrating a direct correlation between mitotic index and biological behavior exist, the mitotic index should be reported as in the study (eg, MF/10 hpf for canine cutaneous mast cell tumors). 15 Variations in the size of the microscopic field of vision between different brands of microscopes, the variation of mitotic activity within tumor samples, and the potential variation of cell density throughout a tumor are all factors that limit a standardized and objective evaluation and commonly result in interobserver variation.
Necrosis
The degree of necrosis observed may be dependent upon the region of tumor selected at trimming (eg, central vs peripheral). However, if trimming methods previously described are adopted, broader microscopic evaluation of the tumor will be obtained and regional bias will be diminished.
Vascular invasion
Vascular invasion suggests an increased probability of metastatic disease and more aggressive biological behavior. Descriptions should include the presence or absence of neoplastic cells within vessels, the type of vessel affected (if distinguishable), characteristics of vascular invasion (transmural infiltration of the vessel wall by nests of neoplastic cells or the presence of intraluminal tumor emboli), and vascular location (intratumoral vs peritumoral). 9,14,16 If vascular structures are not identified or are indiscernible within the examined specimen, this should be reported.
Margins
Surgical margins may, at times, be the most important parameter for the clinician. 7 Accurate margin evaluation can only be provided on samples that have been submitted and trimmed accordingly. The method by which sections are trimmed for margin evaluation should be provided (see the section titled Trimming). This can be achieved verbally or with an annotated image of the gross specimen (Figs. 3–6). An image allows the pathologist to easily identify and describe areas of incomplete resection to the client. Microscopic evaluation of margins should include (1) a description of the neoplastic cells closest to the margin (eg, peripheral cells of an overt mass, infiltrative nests beyond the mass), (2) an accurate and objective measurement (via stage or ocular micrometer) of the distance from the tissue edge to the closest neoplastic cell (this parameter is limited to nontangential sections), and (3) the tissue constituents (eg, adipose tissue, dense connective tissue) and tissue quality (eg, viable, necrotic, inflamed) composing the margin, since different tissue types provide variable barriers against invasion or infiltration of neoplastic cells.
Assuming appropriate sample submission and trimming, as discussed previously, a pathologist should be able to clearly determine which slides and/or colors of surgical ink represent which respective margins so they can reliably provide the above parameters. Measurements can be reported in micrometers, millimeters, or centimeters but should remain consistent for all margins reported for that specimen. Reports of this information should be concise yet detailed and accurate, such as “random, rare, nests of neoplastic cells are within 3 mm of the deep margin which consists of normal adipose tissue (2.5 mm) and panniculus muscle (0.5 mm)” followed by “in the plane of section of the tissue examined.” Vague or ambiguous terms, such as clean, dirty, close, and narrow, should be avoided because they are subjective and introduce interpathologist variability.
When surgical excision is extensive and no neoplastic cells are present in the nontangential margin sections, the margin measurement can be reported as “at least x,” where x constitutes the entire length/distance of the examined tissue.
Comments/Remarks
This section allows the pathologist to directly communicate with the clinician, relaying additional information and thoughts about the case. This additional communication should address the following: If further evaluation requiring a final report is pending, this should be clearly stated and the pending parameters indicated (eg, additional sections, decalcification, special stain). Recommendations for additional diagnostic tests (special stains, IHC, PCR) should be provided when applicable. IHC, although most often used to assist in determining histogenesis, is more frequently being used for prognostic and therapeutic indications.
21,22
Comments regarding biological behavior, prognosis, and general adjuvant therapies from which the patient may benefit (eg, chemotherapy for canine hemangiosarcoma
19
or osteosarcoma
2
) can be included at the pathologist’s discretion. However, these comments should be reserved for the general practitioner and should include supporting references (discussed in further detail below). Any anecdotal information must be noted as such. Recommendation for veterinary oncologist consultation may be beneficial depending on the case but should always be included if comments regarding general therapeutics are made. References (eg, Patnaik AK, et al. Vet Pathol If a comment is deemed unnecessary (eg, “Sebaceous adenoma. Excision complete.”), the use of “N/A” or “no comment” is recommended to convey to the clinician that a comment was not omitted in error.
The scope of comments, particularly in relation to biological behavior and general therapeutics, is often of great assistance to the general practitioner and may facilitate practitioner–client interactions, ultimately resulting in referral to a veterinary oncologist.
When a specimen is received from, and hence the report generated for, a board-certified veterinary oncologist, general comments regarding biological behavior, prognosis, and especially therapeutic recommendations should be reserved. The pathologist must be cognizant of the clinician submitting the sample and tailor the report appropriately. However, information that may not be common knowledge throughout the veterinary oncology community (eg, recent publications, conference presentations, or comparative medicine correlations) may be provided at the pathologist’s discretion. Such data should be appropriately referenced or noted as anecdotal or experiential. Clinicians will draw their own conclusions as to the degree of relevance they believe a particular study’s findings may have on the case in question.
If a report initially submitted to a general practitioner is transferred to an oncologist at referral, and the information in the report differs from recommendations suggested by the oncologist, the reporting pathologist can be contacted, with the consent and knowledge of the original clinician, to discuss the information. If necessary, an amended report/addendum can be created. An open discussion and acceptance of new information may improve patient treatment and foster an essential and critical relationship between the pathologist and the oncologist.
Additional Report Components
Documentation of the samples received can be included in the report or, at minimum, should be recorded in laboratory records. Ideally, a gross description of the specimen should be included but may be unnecessary if digital images are provided for trimming purposes. The report should include a brief clinical history/lesion description, as provided by the clinician on the submission form, as well as administrative information (eg, clinic name, address, telephone number).
Postreport Options
Receipt of the final pathology report does not necessarily correlate with case completion. If any conflict exists between the reported information and clinical impression, the clinician should contact the reporting pathologist without hesitation. Discussion may result in any number of outcomes, such as clarification of information, correction of a clerical error, or initiation of steps for further evaluation. Familiarity with the pathologist is recommended to facilitate clinician–pathologist interactions. Familiarity with the laboratory’s internal regulations and requirements, typically provided in the laboratory’s quality manual, is also strongly encouraged. These include, but are not limited to, methods of quality assurance and quality control (QA/QC) for sample receiving, trimming, reporting, case evaluation, and histochemical and immunohistochemical staining techniques, protocols, and evaluation. Institutional laboratories are often accredited by the American Association of Veterinary Laboratory Diagnosticians (AAVLD), which indicates they adhere to the guidelines set forth by the AAVLD (available at www.aavld.org). Private laboratories often adhere to internal QA/QC guidelines, which may be provided upon request.
Consultation With the Pathologist
To facilitate clinician–pathologist interaction, familiarity with the pathologist is strongly encouraged. Information about the pathologist the clinician should be aware of, and which should be provided in the report, includes the following: Pathologist signature; handwritten or electronic (signature denotes final approval and release of report by the pathologist). Laboratory telephone number (ideally including pathologist extension). Veterinary board certification (eg, DVM, VMD, or equivalent); MD pathologists are not trained in veterinary tumor pathology or terminology, which may lead to misdiagnoses. Advanced pathology degrees (eg, Diplomate of the ACVP or ECVP, PhD) and pathology specialty (anatomic, clinical).
Oral communication (telephone, VoIP, video conferencing, other) is encouraged over written communication (eg, e-mail), since the latter presents greater potential for error in interpretation. If not immediately available, every effort should be made by the pathologist to respond within 24 hours of an inquiry. Laboratory staff may be able to assist the clinician in resolving the problem. An official amended report or addendum may need to be generated. At minimum, the conversation and outcome should be documented for laboratory records, which is typically a requirement of laboratory-dependent QA/QC guidelines.
Clinician Requests
Clinicians may request further evaluation if the clinical impression does not correlate with reported findings. Such requests can include reevaluation of the original slide(s), evaluation of additional wet tissue, special stains, deeper levels/step-sections of the original block, or, when necessary, a second opinion by an additional pathologist. On occasion, repeated biopsy may ultimately be the best option. Reevaluation of original slides may be the most efficient way to resolve an issue. This may be requested for evaluation of an unreported feature (ie, vascular invasion) or when the clinician expected a different diagnosis and would like the specimen reevaluated with that diagnosis in mind. Evaluation of additional wet tissue is typically requested when there is concern that the mass lesion may have been missed during trimming or when trimming failed to capture viable tumor tissue (eg, necrotic or hemorrhagic areas in hemangiosarcoma), rendering the results nondiagnostic. Depending on the laboratory, wet tissues may be stored from 2 weeks to 3 months. Additional charges may apply depending on the laboratory’s pricing schedule. Histochemical stains and/or immunohistochemical panels may be beneficial in the face of a questionable or undetermined diagnosis. Additional tests may have been recommended in the original report and often involve additional costs. Technical aspects of generating stains, and methods of evaluating stains, may be critical to the success of the test.
10
Recommended guidelines for IHC have been established by the AAVLD. Ideally, the laboratory performing these tests, which may be a second party laboratory, adheres to these guidelines.
11
Deeper levels (step sections) involve collection of additional 4- to 5-μm sections from the tissue embedded in the block. This is usually requested when no wet tissue is left (eg, core bone biopsies, needle biopsies, or pinch biopsies), and insufficient tissue or absence of neoplastic cells prevents a definitive diagnosis on the original slide. Sections are made in the block at 20- to 50-μm intervals (dependent on the amount of embedded tissue), resulting in additional sections for microscopic evaluation that may reveal larger portions of the tissue specimen or the neoplastic cell population. Second opinion by an additional pathologist is usually requested if case discussion with the reporting pathologist and other steps do not address the clinical concern. The request can be initiated by the pathologist or submitted to the laboratory by the clinician.
Second Opinions
Most commonly, second opinions are carried out internally; review is by a pathologist working at the same laboratory as the reporting pathologist. There may or may not be an additional charge depending on individual laboratory policy. This may be an informal or formal review, depending on the specifications of the clinician or based upon agreement between the clinician and pathologist. Informal review involves collegial requests from one pathologist to another, such as soliciting opinions and thoughts on a case/slide, and may not involve additional costs. Second-party information is relayed by the reporting pathologists in an addendum indicating the case was additionally reviewed by Dr. X, who supports a diagnosis of Y, along with any additional relevant comments.
A formal second opinion is conducted differently in that the second-opinion pathologist will independently generate and sign off on a second-opinion report. This report will consist of the second-opinion diagnosis and comments/remarks and may or may not include a description at the pathologist’s discretion. The second-opinion pathologist should be privy to the initial report but may choose not to review it until after the slides have been evaluated to reduce bias. Second opinions should be performed on the same slide(s) evaluated by the original pathologist. When additional sections (eg, recuts) are acquired, the examined tissue is obtained from a different level of the embedded specimen, which may reveal different tissue characteristics and result in the reporting of different features. If recuts are necessary for the second opinion to transpire (eg, original slides cannot be readily retrieved), sections should be acquired as superficially in the block as possible in an attempt to maintain consistency with tissue components present in the original slide. The original reporting pathologist may also wish to review these recuts to assess consistency of features.
When a second opinion is carried out externally at a different laboratory, the original slides may not be available for submission. Individual laboratories may have proprietary regulations that do not allow release of original slides or blocks but instead will send recuts as requested. This is not ideal but is a practice that currently exists. All external second opinions are formal reviews in which the reviewing pathologist will create an independent second-opinion report as described above. Reports generated by formal second opinions are sent directly to the requesting clinician and should be copied to the original pathologist. Additional charges associated with external second opinions may include the recuts, HE stain, and shipping by the primary laboratory as well as a charge by the external laboratory providing the second opinion.
Interpreting a second opinion
The goal of a second opinion request is to attain the most accurate diagnosis possible. Diagnostic discrepancies between the first and second opinions may arise. Those that affect clinical outcome include overt discrepancy of the diagnosis with regard to degree of malignancy (malignant vs benign) or histogenesis (cell type) or involve discrepancies in tumor grade or vascular invasion. 12 Differences in features such as vascular invasion can vary throughout the specimen and may be a result of slide recuts.
If discrepancies exist between the initial diagnosis and second opinion, the second opinion is not unequivocally the most accurate diagnosis. 21 Instead, it may demonstrate the complexity of the case, and a third opinion or pursuit of additional testing (ie, IHC) to further evaluate the sample may be necessary. Once the case has been submitted to the second-opinion pathologist, he or she should manage any additional tests and reporting of respective results. It is important, however, for all parties to remain informed of all tests and results for continued discussion and an eventual consensus on diagnosis.
Ideally, cases that present enigmatic diagnostic challenges should be monitored closely with persistent clinical follow-up until recuperation or demise of the patient. Information such as clinical progression, outcome, and postmortem examination may be invaluable in confirming or dismissing the suspected diagnosis. Intensive and focused follow-up may identify vital information that can benefit similar cases in the future.
The Future of Second Opinions
There are no guidelines or recommendations on how to approach a second opinion in veterinary medicine. In human medicine, the Association of Directors of Anatomic Surgical Pathology recommends that pathology consultation by the referral institution be standard practice prior to the initiation of treatment. 1,3,6,17,20 For particular cases or under certain circumstances, many human surgical pathology services mandate review of the case by a second pathologist before the report is signed and released. 8 Second-opinion policies that exist in human medicine deserve serious consideration in veterinary medicine.
As digital pathology becomes more common in veterinary medicine, shipment of slides for second opinions may become unnecessary, thereby eliminating shipping costs. This also significantly reduces turnaround time, sample processing costs, and personnel time because recuts and staining may not be necessary. Most important, the original slide can be evaluated without the need to release proprietary materials. Using this technology would also facilitate group discussions as multiple pathologists could gain access to the scanned slide simultaneously.
Conclusions
Optimal management of the veterinary cancer patient requires a unified, interdisciplinary, and highly communicative approach between clinicians, oncologists, and pathologists. Patient care is directed by the diagnosis and information provided in the pathology report. Accurate, thorough, and reliable pathology reports depend on reception of excellent specimens, complete information, and appropriate trimming. This document provides recommended interdisciplinary guidelines for the various stages of tumor biopsy handling, including submission, trimming, margin evaluation, reporting, and postreport activities. These guidelines have been established to assist clinicians and veterinary pathologists in achieving optimal diagnostic accuracy. Moreover, composition of these guidelines has highlighted areas in veterinary oncology/pathology that require attention. Of note, a consensus on diagnostic and grading landmarks relative to specific tumor type, as well as studies critically evaluating various trimming techniques for surgical margin assessment, could be of significant value. These guidelines should be viewed as an evolving document requiring continuous revision as new data are generated, which will be best achieved via a collaborative and longstanding effort between oncologists and veterinary pathologists.
Footnotes
Acknowledgements
We thank Ann Wismer and Thomas Wood of the Diagnostic Center for Population and Animal Health, Michigan State University, for their help with photographing and annotating surgical biopsy samples. This study represents an initiative of the American College of Veterinary Pathologists' Oncology Committee. The manuscript was reviewed and endorsed by the World Small Animal Veterinary Association. We thank both organizations for their support and guidance.
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.