
Abstract
Spontaneous vestibular syndrome in mice, characterized clinically by head tilt, circling or rolling, can be caused by otitis media, arteritis or central nervous system lesions. Postmortem examination of eleven non-inbred Swiss mice submitted for necropsy due to acute onset of vestibular signs revealed lesions consistent with brainstem infarction. The lesions were characterized by unilateral, well-demarcated areas of necrosis, malacia, and gliosis, with variable amounts of hemorrhage, in the lateral aspect of the medulla and caudal pons. The affected area included the medial, lateral and superior vestibular nuclei, the facial nucleus and the spinal trigeminal nucleus. While vestibular disease secondary to otitis media, periarteritis, and central nervous system neoplasia has been reported in many mouse strains, these unilateral brainstem infarctions were only seen in Swiss mice. These lesions share features with Wallenberg's Lateral Medullary Syndrome, the most common type of brainstem infarct in humans.
The vestibular system provides sensory input about body position and movement. Sensory receptors are located in the inner ear and consist of specialized hair cells that detect movement and head position. Afferent projections from the hair cells travel via the eighth cranial nerve and synapse on neurons in the vestibular nuclei of the brainstem or the uvula or nodulus of the cerebellum. Lesions in any of these components can cause vestibular syndrome, which in mice is characterized by head tilt, rolling, spinning, and inability to eat, drink, or groom normally. Otitis media, 9,11 arteritis, 12 and central nervous system lesions 5 have been reported to cause vestibular syndrome in mice.
Between 2006 and 2009, 11 noninbred female Swiss mice, 1 Hsd:ND4 and 10 Hsd:ICR(CD-1), with acute vestibular signs were presented to the necropsy service at Johns Hopkins University. Ten mice were sentinels, and the remaining mouse had not been experimentally manipulated. All mice were adults less than 1 year old. The mice were euthanized with carbon dioxide, and complete necropsies 3 were performed. Blood was collected via cardiocentesis from 4 mice and submitted for routine serology. Mouse heads were decalcified with Formical (Decal Chemical Corporation, Tallman, NY) for 24 hours before sectioning. Tissue sections from all organs were stained with hematoxylin and eosin for microscopic evaluation.
Each of the 11 Swiss mice with vestibular syndrome had a focally extensive, well-demarcated area of necrosis in the lateral brainstem. On gross examination, the affected area was characterized by malacia, variable amounts of red-brown discoloration, and, rarely, cavitation of the lateral aspect of the caudal pons and rostral medulla (Fig. 1 ). The lesions occurred on the left (n = 5) and right (n = 6) of the brainstem. Histologic examination revealed discrete areas of rarefaction, neuronal necrosis, mild gliosis, and in some cases, hemorrhage in a region of the lateral brainstem that included the medial, lateral, and superior vestibular nuclei, the facial nucleus, and the spinal trigeminal nucleus (Figs. 2, 3). In 1 mouse, a mural thrombus was identified in a small arteriole adjacent to the lesion (Fig. 4 ). Another mouse had unilateral, mild, multifocal neutrophilic myositis and skeletal muscle degeneration in the neck muscles on the affected side, attributed to trauma from rolling. Step sections through the head and neck tissues failed to identify inflammatory lesions or anatomic abnormalities of the inner ear, middle ear, eighth cranial nerve, or cervical or cerebral vasculature. Heart weights were within normal limits, and there was no histological evidence of cardiomyopathy. Standard mouse serology screens were negative.
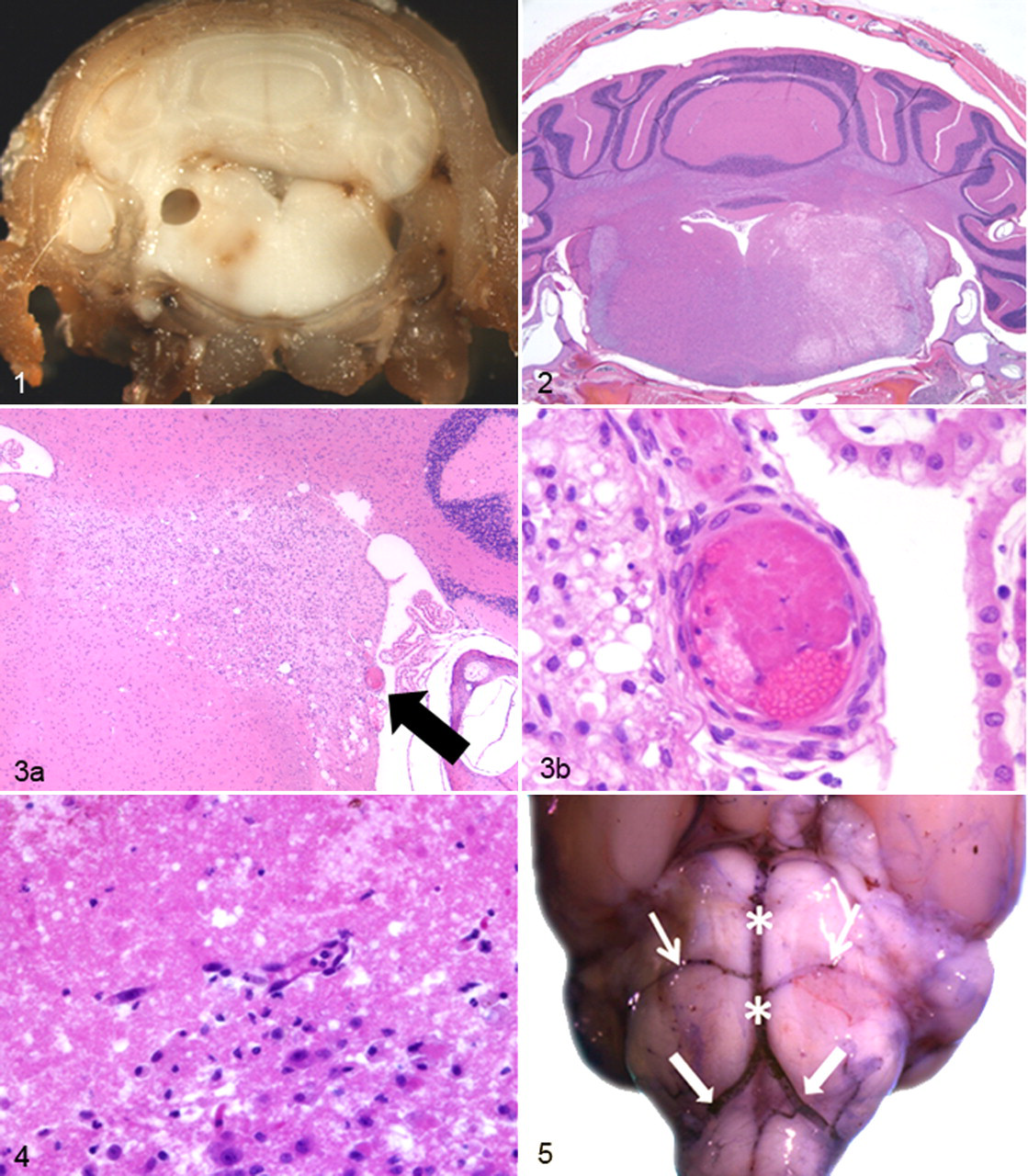
The histopathology findings in these 11 mice suggest that vestibular signs were secondary to infarction of the lateral brainstem. Examination of the mouse brainstem vasculature—via postmortem intracardiac injection with cresyl violet—confirmed that the affected area roughly corresponds to the course of the caudal cerebellar artery, a branch of the basilar artery that emerges just distal to the convergence of the vertebral arteries (Fig. 5 ).
The majority of cerebrovascular accidents, or strokes, in humans involve the anterior cerebral circulation, supplying the cerebrum. 4 Strokes involving the posterior circulation (vertebral and basilar arteries and branches) are less common but tend to have higher mortality and more adverse neurological sequelae in survivors. 4 The most common type of brainstem infarct in humans is Wallenberg lateral medullary syndrome (LMS), which involves occlusion or rupture of the vertebral artery, basilar artery, posterior inferior cerebellar artery, or medullary artery, with resulting ischemia of the lateral brainstem. 8 Clinical signs and symptoms associated with lateral medullary syndrome include vertigo, ataxia, sensory deficits, Horner syndrome, and nystagmus. Risk factors for posterior circulation strokes are similar to those for anterior circulation strokes and include hypertension, atherosclerosis, and diabetes mellitus. In young patients, posterior circulation strokes are often associated with vertebrobasilar artery abnormalities such as dissections and are occasionally associated with cervical spine subluxation. 6 None of these risk factors have been reported in young Swiss mice.
Several animal models of posterior circulation infarcts have been developed. Vertebrobasilar strokes have been modeled in rabbits via endovascular occlusion of the basilar artery. 1 These animals develop bilateral ischemic lesions in the pons, with variable involvement of the cerebellum, medulla, and midbrain. In rats, posterior circulation infarcts have been modeled by injection of thrombi into the vertebral artery near its origin in the thorax. 7 The majority of these rats developed neurologic signs, such as rolling, nystagmus, and ataxia, and ischemic lesions were documented in the medulla, pons, or cerebellum. Models of posterior circulation ischemic stroke have also been developed in dogs, cats, and gerbils 10 but not in mice. Spontaneous brainstem infarcts are rarely reported in any veterinary species.
The lack of male mice affected during the reporting period likely reflects the institutional use of female mice as sentinels and the resulting predominance of female Swiss mice at this institution. During the 3-year period in which these mice presented for necropsy, more than 17,000 female ICR Swiss mice from a single vendor were used as surveillance sentinels. However, we cannot rule out a sex predilection. In humans, all strokes are more common in males than in females, but the gender difference is less pronounced in posterior circulation strokes. 14 Unilateral brainstem malacia was not seen in any other mouse strain during the 3-year period. Non-Swiss mice presenting with vestibular disease during that time frame (n = 6) were diagnosed with well-recognized causes of vestibular dysfunction in mice, such as otitis interna (n = 2), arteritis (n = 3), and central nervous system neoplasia (n = 1). Also, ischemic lesions were not seen outside the brainstem in the affected Swiss mice or any other Swiss mice examined. These findings warrant further studies of the anatomy and hemodynamics of the brainstem vasculature in Swiss mice compared with other mouse stocks and strains. Strain-associated anatomical differences in cerebral vasculature have been reported to affect susceptibility to cerebral ischemia. 2,15 Compared with inbred mouse strains, the noninbred Swiss mouse stocks, such as Hsd:ICR(CD-1) and Hsd:ND4, are expected to have greater genetic diversity. 13 Their heterogeneity may contribute to the low incidence of presumptive brainstem infarcts in Swiss mice at our institution.
In conclusion, unilateral brainstem malacia, suggestive of infarction, represents a previously undescribed cause of vestibular signs in Swiss mice. This lesion has been identified in only relatively young Swiss mice with no other significant gross or microscopic lesions, and it shares features with Wallenberg lateral medullary syndrome, the most common type of brainstem infarct in humans.
Footnotes
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
The authors declared that they received no financial support for their research and/or authorship of this article.