
Abstract
A progressive debilitating disease of the orbit and adjacent connective tissues of cats has historically been called feline orbital pseudotumor. The authors reviewed clinical, histopathologic, and diagnostic imaging features of this disease in 12 cases from the Comparative Ocular Pathology Laboratory of Wisconsin. The cats' ages ranged from 7 to 16 years (mean, 10.8 years). All cats had a history of severely restricted mobility of the globe and eyelids with secondary corneal disease. Eleven cats (92%) had concurrent involvement of the contralateral eye and/or the oral cavity. Diffuse scleral or episcleral thickening was seen with computed tomography in all clinically affected eyes. Histologically, an insidious infiltration of neoplastic spindle cells in the orbit, eyelids, and periorbital skin and soft tissues, with collagen deposition and a few perivascular lymphocytes, led to entrapment and restricted mobility of the eyelids and orbital tissues. The tumor failed to form a discrete mass, and it spread along fascial planes to the contralateral orbit and eyelids and/or the lips and oral cavity. In all tested cases (n = 10), neoplastic cells were immunohistochemically positive for vimentin, S100 protein, and smooth muscle actin. The authors adopted the term feline restrictive orbital myofibroblastic sarcoma to reflect the restricted mobility of the eyelids and globe and the imaging and histologic features of an invasive yet low-grade myofibroblastic sarcoma.
Proliferation of fibrous tissue in the presence of lymphocytic inflammation has been reported in the orbit, 2,20 face, 15 and limb 23 of cats as either nodular fasciitis or pseudotumor. The term pseudotumor was borrowed from the human condition known as orbital pseudotumor 9,14,21,26 and applied to this chronic, nonspecific, and fibrosing inflammation of the feline orbit.
This sclerosing orbital feline disease is progressive and poorly responsive to treatment, and it frequently leads to euthanasia. Miller et al reported a case in which disease progressed from one eye to the other despite treatment. 20 From the 7 cases that Billson et al reported, the disease progressed from unilateral to bilateral in 6 cats, despite various treatments; 2 cats had oral lesions as well as ocular involvement; and 6 were euthanized because the severity of the disease. 2 The reported aggressive behavior suggests that despite its bland cellular appearance, this is a true neoplastic process that preferentially affects the orbit and adjacent tissues. Therefore, we propose the term feline restrictive orbital myofibroblastic sarcoma (FROMS) as a more accurate reflection of the disease characteristics.
Based on histopathologic features alone, the orbital, oral, or skin lesions of this disease may be misinterpreted as nonspecific reactive fibroplasia or granulation tissue. However, its progressive course and unfavorable prognosis highlight the importance of early and accurate diagnosis. The purpose of this study is to describe the clinical, diagnostic imaging, histologic, and immunohistochemical features of FROMS.
Materials and Methods
The records from the Comparative Ocular Pathology Laboratory of Wisconsin (COPLOW) were searched for cases with a diagnosis consistent with FROMS, as either low-grade orbital sarcoma or feline orbital pseudotumor. A survey was sent to submitting veterinarians requesting medical history and follow-up information, including imaging studies. Only cases with available records were included in the study. Imaging studies were evaluated only if they contained precontrast and postcontrast computed tomography (CT) or magnetic resonance imaging (MRI) of the head of diagnostic quality. Medical records were reviewed for signalment, type and duration of clinical signs, type and outcome of treatments, clinical progression of disease to the contralateral eye and/or oral cavity, survival, and prior histologic diagnosis before submission to COPLOW.
Histologic sections stained with hematoxylin and eosin (HE) were reviewed for all cases. Only those cases with adequate tissue for diagnosis (globe, eyelid, and/or orbital tissue) were included in the study. Histologic criteria for inclusion included the presence of spindle cell proliferation within orbital tissue and/or eyelids with low cellular atypia, low mitotic rate, and a collagenous matrix. Histologic sections were evaluated for cytologic features and distribution of neoplastic cells, as well as type and extent of leukocytic infiltration.
For immunohistochemistry, formalin-fixed, paraffin-embedded 5-μm-thick sections were deparaffinized and rehydrated; antigen retrieval was performed with the Lab Vision PT Module (Lab Vision Corporation, Fremont, CA) using citrate buffer (pH 6) for 20 minutes. Endogenous peroxidase activity was blocked by incubation for 10 minutes in 3% hydrogen peroxide, followed by 5 minutes in Ultra V Block (Lab Vision Corporation)
The following primary antibodies were used: mouse anti–feline CD18 (1:15, clone FE3.9F2, Leukocyte Antigen Laboratory, Davis, CA), rabbit anti–glial fibrillary acidic protein (1:2000, Dako, Glostrup, Denmark), rabbit anti–S100 protein (1:2500, Dako), mouse anti–Melan A (1:30, clone A103, Dako), mouse anti–smooth muscle actin (1:1000, clone 1A4, Dako), and mouse anti-vimentin (1:200, clone V9, Dako). Bound antibodies were detected with horseradish peroxidase–conjugated anti-mouse or anti-rabbit secondary antibody with diaminobenzidine as a chromogen and counterstained with Harris hematoxylin. Adjacent tissues provided an internal positive control for glial fibrillary acidic protein, S100, smooth muscle actin, and vimentin. Feline lymph node was used as a positive control for CD18. A feline ocular melanoma was used as a positive control for Melan A. Test samples with omission of primary antibody were used as negative controls.
Basic CT and MRI acquisition data were collected. CT examinations were performed in axial acquisition mode with 1- to 3-mm slice width and interval, 80- to 160-kV peak voltage, 130- to 160-mA current settings, and a combination of medium- and high-frequency image reconstruction algorithm. The MRI study included T1 precontrast and postcontrast series in transverse and dorsal orientation, as well as T2-weighted sequences. All CT and MRI images were reviewed in DICOM (Diagnostic Imaging and Communications in Medicine) format on a computer with dedicated viewing software (eFilm Workstation 3.1.0, Merge Technologies Inc, Milwaukee, WI) or printed films by one board-certified radiologist (T.S.) who was aware of the diagnosis. Evaluation criteria included subjective thickness of sclera or episclera and eyelid (normal or thickened); clarity of retrobulbar soft tissue margins (well or poorly demarcated); gingival thickness of the hard palate (normal, thickened); soft tissue thickness of the interorbital nasofrontal cutis (normal, thickened); position of the globe in relation to the orbit (enophthalmos, normal, or exophthalmos); orbital and periorbital contrast enhancement (none, mild, marked); and evidence of bony lesions or regional lymphadenopathy.
In the course of collecting follow-up information from veterinarians, additional tissue from necropsy became available in 3 cases (case Nos. 1, 2, 5) for gross and histopathologic review. A full necropsy was performed on case Nos. 1 and 5, whereas only the formalin-fixed head was available for case No. 2. Decalcified sections of the skull were stained with HE.
Results
Clinical History
Twenty-three cats with this lesion type were identified in the collection from 1999 through 2008; of these, 12 had adequate medical records and tissue sections for inclusion in the study. One of the 12 cases was reported by Miller et al. 20 Diagnostic-quality CT imaging was available for 6 of the 12 cases. One of those 6 cases also had MRI for review.
The cats ranged in age from 7 to 16 years (mean, 10.8 years). There were 5 neutered males and 7 neutered females. Nine cats were domestic shorthair; 3 were domestic longhair.
The most frequently reported clinical signs were ulcerative keratitis, thickened eyelid, restricted mobility of the eyelids with associated lagophthalmos, and restricted mobility of the globe with reduced retropulsion of the globe (Table 1 ). In 3 of the 12 cases, the submitting veterinarian reported the presence of a mass lesion, although it is not clear whether this was based on clinical observation or on imaging suggestive of a retrobulbar mass. Duration of clinical signs at the time of biopsy ranged from 2 weeks to 6 months (mean, 2.6 months).
Clinicopathologic Features and Outcome in 12 Cases of Feline Restrictive Orbital Myofibroblastic Sarcoma
a DSH, domestic shorthair; DLH, domestic longhair; FS, female spayed; MN, male neutered; CT, computed tomography; MRI, magnetic resonance imaging.
b Progression and survival are measured from date of onset, as calculated from sample submission date and reported duration.
c Postenucleation imaging.
d Mass effect evident by ultrasound.
e Not examined.
Of 11 cats that received some type of medical intervention, all had progressive disease despite treatment. The most frequent medical therapies were topical or systemic antibiotics, topical or systemic anti-inflammatory doses of glucocorticoids, and in 1 case, antiviral therapy. Surgical treatment (enucleation or exenteration) was elected in all cases.
At the time of initial presentation to the submitting veterinarian, 10 cats had unilateral ocular involvement. Two cats also had involvement of the lips and/or oral cavity. Two cats had bilateral ocular involvement at initial presentation. In 7 cats, the clinical disease progressed to the contralateral eye. Five of these “second eyes” were evaluated histologically in our laboratory. The time between presentation for clinical disease in the first eye and presentation for clinical disease in the contralateral eye ranged from 0 to 8 months (mean, 4.3 months). Oral involvement developed in 9 of the 12 cats; oral tissue was evaluated histologically from 4 of these cases. The time from presentation for clinical disease in the first eye to identification of oral lesions ranged from 0 to 14 months (mean, 5.7 months). At the time of this writing, 10 cats died; all were euthanized because of poor quality of life directly attributable to orbital and/or oral disease. Survival time from first presentation with clinical disease ranged from 3 to 15 months (mean, 9.1 months). Only 2 cats lived: cat No. 10 had unilateral ocular and oral disease, and cat No. 4 had no apparent disease progression at 5 months postenucleation of the affected eye.
Before submission to COPLOW, initial histopathologic diagnoses had been made in 6 cases: 3 from a conjunctival biopsy, 2 from enucleated globes, and 1 from orbital tissue obtained at enucleation without submission of the globe. In each case, the initial histologic diagnosis was chronic inflammation with fibrosis and/or granulation tissue.
Clinical Imaging
CT had been performed in 6 of the 12 cats; an MRI study has been performed in 1 case. Adequate contrast medium uptake was evident by contrast enhancement of the linguofacial veins. In case no. 2, an MRI was performed pre-enucleation, and CT was performed postunilateral enucleation. In 2 other cases, CT examinations were performed after unilateral enucleation (case no. 1) and bilateral enucleation (case no. 3). Thus, a total of 9 globes were evaluated by diagnostic imaging.
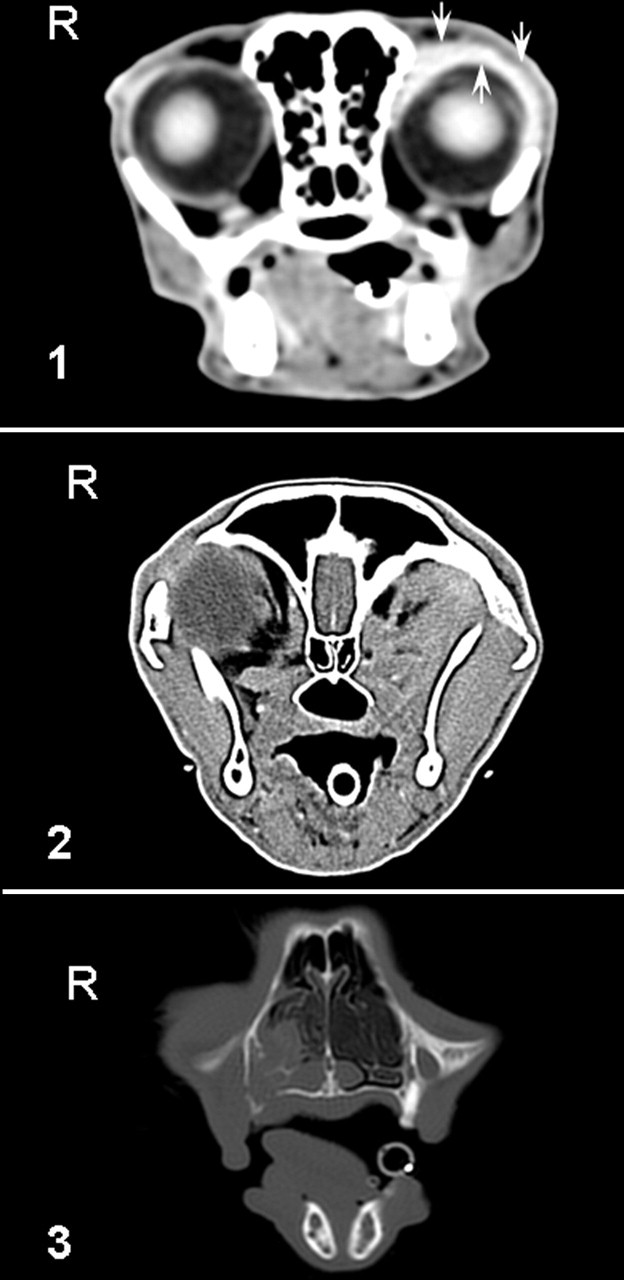
The sclera or episclera was thickened in 4 eyes and initially normal in 5 eyes; in 1 of these latter eyes, thickening was detected on a follow-up CT scan (Fig. 1 ). The eyelids were difficult to assess but appeared thickened and irregular in 3 cases. The retrobulbar soft tissues initially had poorly demarcated margins posterior to 2 eyes and well-demarcated margins posterior to 7 eyes; in 1 case, well-demarcated soft tissue margins became poorly demarcated on a follow-up CT scan (Fig. 2 ). The gingiva of the hard palate and the interorbital nasofrontal cutis were thickened in 2 cases each (Nos. 1 and 2 and Nos. 1 and 3, respectively). In 2 globes, the scleral/episcleral thickening was exclusively in the anterior part, with no invasion of the retrobulbar space. The 4 postenucleation orbital cavities were filled with material of a soft tissue density, often containing a nonenhancing core. One globe was enophthalmic; 1 was exophthalmic; and 7 were in a normal position. The sclera of all globes was enhanced postcontrast administration. However, only those scleral and episcleral tissues that were notably thickened had consistent marked contrast enhancement. Bone lesions were observed in one follow-up CT study (No. 2), with extensive osteolysis of the orbital wall nasally and invasion into the nasal cavity by a soft tissue mass (Fig. 3 ). In this case, bone resorption and remodeling with neoplastic infiltration into the nasal cavity and sinuses were confirmed by histologic examination of decalcified sections of the skull. There was mild bilateral mandibular and medial retropharyngeal lymphadenopathy in 1 cat (No. 2) and marked unilateral mandibular and retropharyngeal lymph node enlargement ipsilateral to the enucleated orbit on one postenucleation CT scan in 2 cases (Nos. 1 and 3). Tissue was not available for histologic evaluation of any lymph nodes identified as being enlarged by imaging. However, in one of the necropsy specimens (No. 5), mandibular and retropharyngeal lymph node enlargement was noted grossly ipsilateral to the previously enucleated eye, although these lymph nodes had been normal on imaging. Histologically, the enlarged lymph nodes had reactive hyperplasia but no evidence of tumor metastasis.
Gross Findings
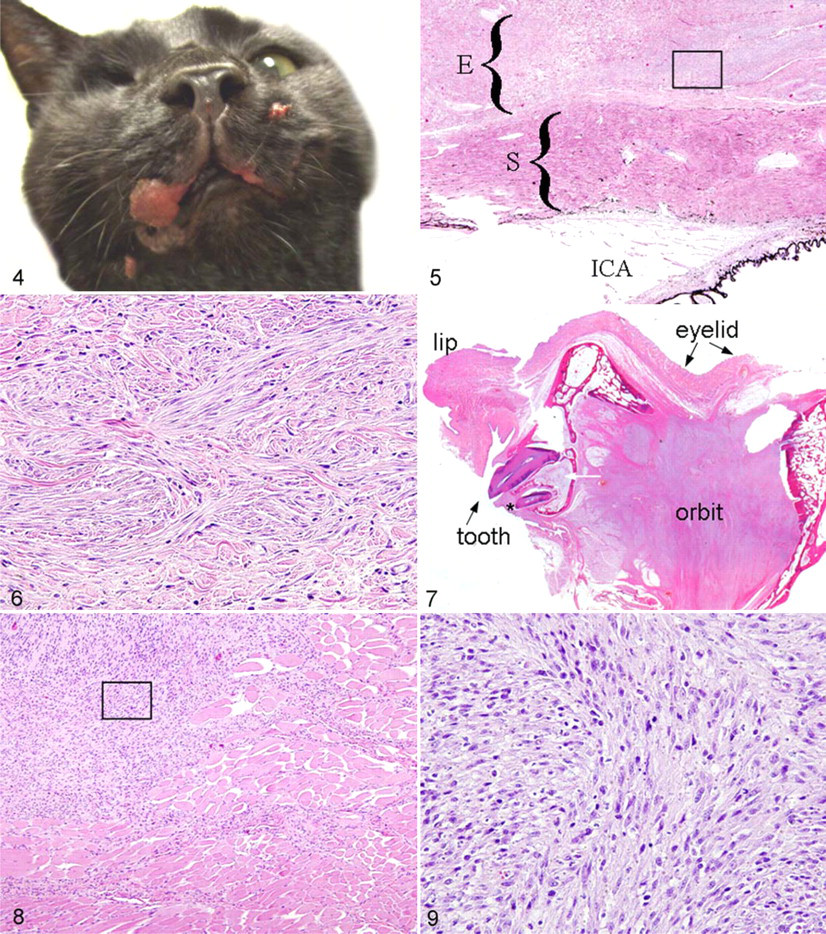
Of the cats that were examined by necropsy, cat No. 2 had bilateral ocular involvement, whereas Nos. 1 and 5 had unilateral ocular involvement with progression to the ipsilateral oral cavity and lip. Each cat had had a unilateral enucleation/exenteration. At necropsy, dense white fibrous tissue filled each orbit. In cat No. 1, the neoplastic tissue extended beyond the orbit and markedly thickened the dermis over an extensive area of the ipsilateral side of the face and upper lip. In cat No. 2, there was gross thickening of the palate and proliferation of the maxillary gingiva. Cat No. 5 had thickening and multifocal ulceration of the skin overlying the muzzle bilaterally as well as a discrete, broadly pedunculated and ulcerated mass on the margin of the upper lip ipsilateral to the affected eye (Fig. 4 ). In one cat (No. 5), there was asymmetric enlargement of the ipsilateral mandibular and retropharyngeal lymph nodes.
Histologic Findings
Tissue was available for histologic evaluation from a total of 17 clinically affected eyes. Of these, the globe was available for 16 cases; orbital tissue, for 11 cases; and eyelid tissue, for 10 cases. Consistent histologic findings in all cases included poorly delineated and infiltrative spindle cells within a collagenous matrix, infiltration and invasion along fascial planes with entrapment and atrophy of normal orbital tissues, moderate to severe keratitis, and minimal to moderate multifocal lymphoplasmacytic inflammation of orbital tissues. Spatially, the densest infiltration of neoplastic cells was in the substantia propria of the bulbar conjunctiva, either at the limbus or in the palpebral conjunctiva near the fornix (Fig. 5 ). In haired skin, neoplastic infiltration was denser within the hypodermis and deep dermis than in the superficial dermis. Consistent cytological features of neoplastic cells included mild to moderate anisocytosis and anisokaryosis, a diffuse to stippled chromatin pattern, an occasional single nucleolus, and low mitotic activity (Fig. 6 ). Mitotic figures per 10 fields (400×) were 0 (n = 11), 1 (n = 4), and 2 (n = 2). Evidence of metastasis and tumor necrosis was not observed.
Mild to moderate multifocal and perivascular lymphoplasmacytic inflammation was observed in orbital tissues in most cases. Frequently, inflammatory foci occurred at the margin between neoplastic and preexisting tissues, corresponding to a fascial plane. Occasional areas of tumor with a more diffuse lymphoplasmacytic infiltration were within the eyelid or nictitans, adjacent to regions of marked lymphoplasmacytic conjunctivitis.
The cornea was severely inflamed and ulcerated in all affected globes; lesions ranged from acute suppurative keratitis to chronic neovascular and fibrosing keratitis. Corneal perforation was seen in one globe; 3 globes had a corneal sequestrum. With the exception of corneal disease, the globe proper was minimally affected in all cases.
Histologic features of tissues from the 3 necropsy cases (Nos. 1, 2, and 5) included lysis of orbital bone, filling of the enucleated orbit with a solid spindle cell population and collagenous matrix, and neoplastic infiltration of the adjacent tissues along fascial planes (Fig. 7 ). Neoplastic cells infiltrated the oral lamina propria in all 3 cases and the nasal submucosa in both cases for which tissue was examined. In all 3 cases, cellular and nuclear atypia and mitotic activity were greater in the neoplastic cells of oral than orbital tissue (Figs. 8, 9 ). Neoplastic cells from the primary orbital tumors had 0 to 1 mitotic figures per 10 fields in all cases. However, neoplastic cells in oral tissue had 2, 14, and 5 mitotic figures per ten fields in Nos. 1, 2, and 5, respectively. There was no gross or histological evidence of regional metastasis in any case. Histologic findings in the necropsy specimens correlated with the clinical imaging, with neoplastic tissue thickening the interorbital dermis and subcutis (No. 1) and expanding the oral lamina propria of the hard palate (Nos. 1 and 2).
Immunohistochemistry
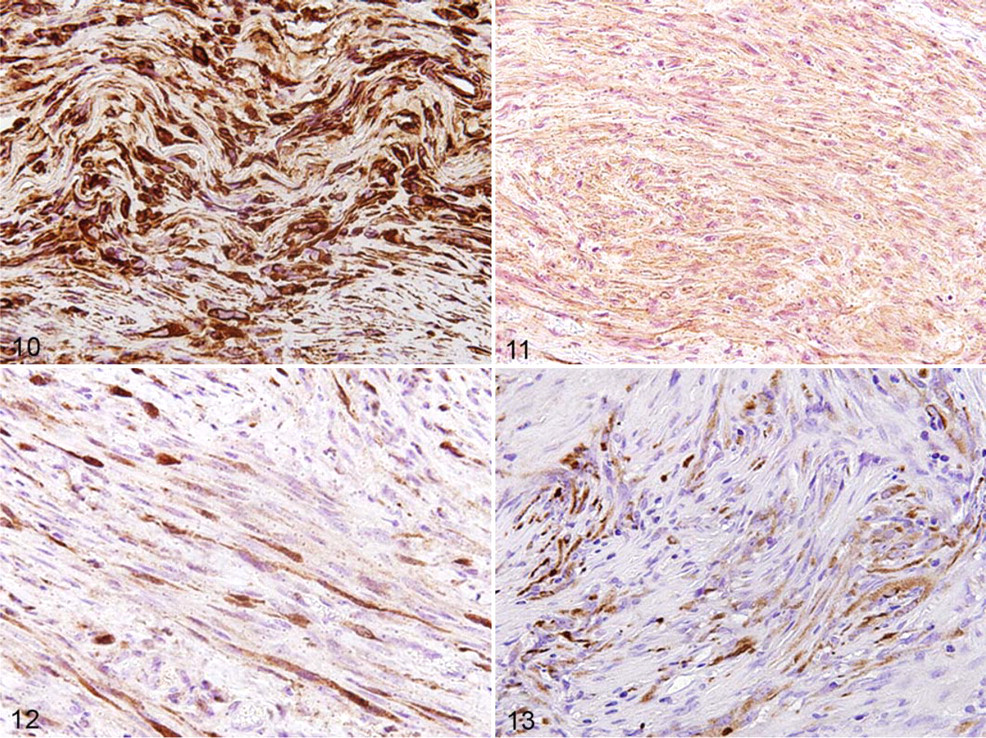
Table 2 summarizes the results of immunohistochemistry. There was strong cytoplasmic labeling with vimentin, > 75% of the neoplastic cells (Fig. 10 ) in all cases tested (n = 10). Smooth muscle actin was strongly expressed in the cytoplasm, > 75% of the neoplastic cells in 8 of the 10 cases tested (Fig. 11 ), whereas partial labeling was observed in 2 cases. Labeling for S100 protein was moderate to weak within the cytoplasm and erratic within the nucleus, > 75% of the neoplastic cells in 7 cases and 25–50% in 3 cases (Fig. 12 ). Seven of the 10 cases had no labeling for glial fibrillary acidic protein; 3 had moderate to weak cytoplasmic labeling, < 25% of neoplastic cells (Fig. 13 ). Immunolabeling for Melan A and CD18 was evaluated in only 2 cases (Nos. 2 and 9), with no positive labeling for either marker.
Immunohistochemistry in 12 Cases of Feline Restrictive Orbital Myofibroblastic Sarcomas a
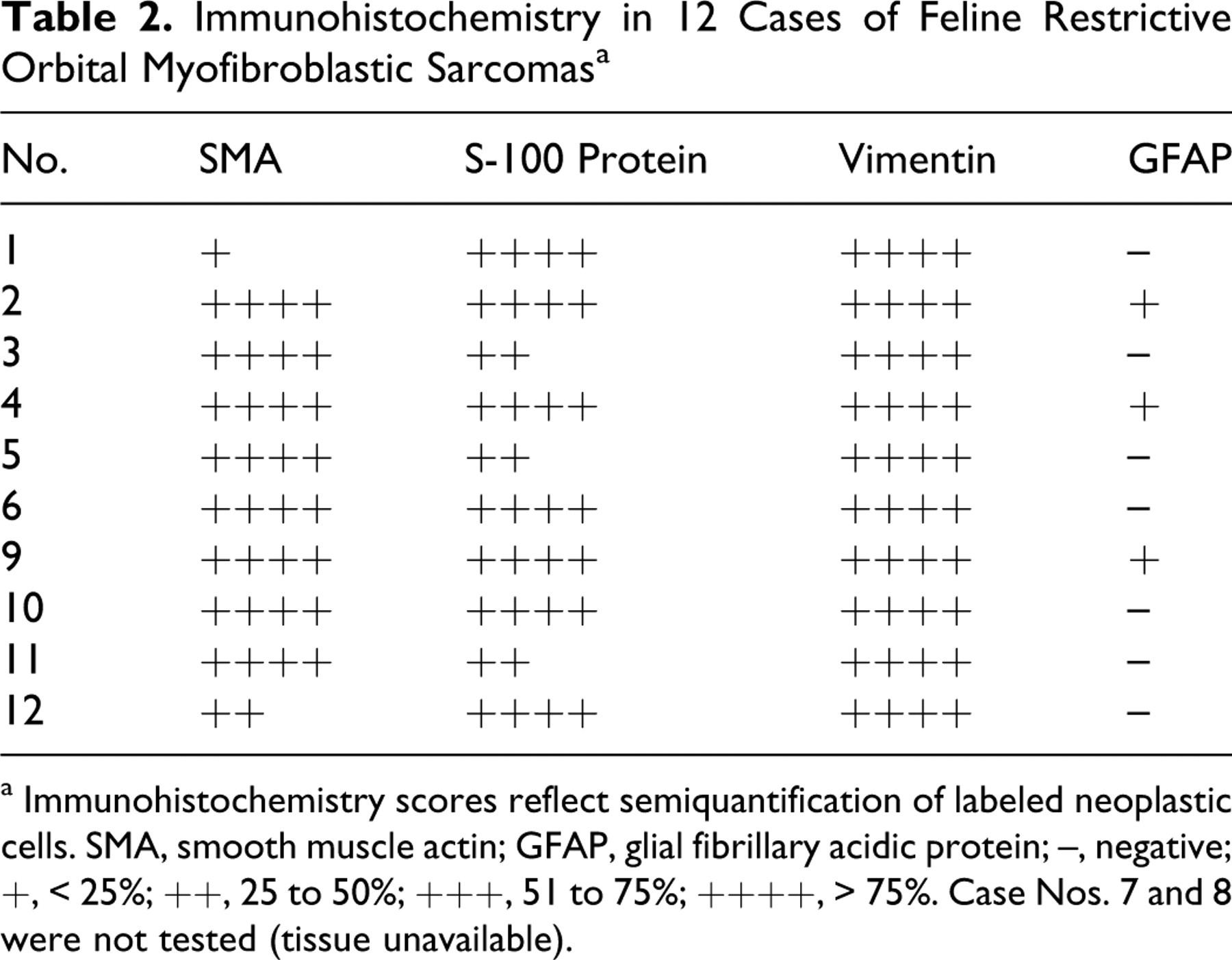
a Immunohistochemistry scores reflect semiquantification of labeled neoplastic cells. SMA, smooth muscle actin; GFAP, glial fibrillary acidic protein; –, negative; +, < 25%; ++, 25 to 50%; +++, 51 to 75%; ++++, > 75%. Case Nos. 7 and 8 were not tested (tissue unavailable).
Discussion
FROMS is a progressive and fibrosing condition with characteristic clinical, pathological, diagnostic imaging, and immunohistochemical features. Recognition of these features is critical for the diagnosis of this condition, which generally responds poorly to treatment and bears a poor prognosis.
Clinically, most cats were presented with unilateral ocular involvement and subsequent progression of the tumor to the contralateral eye and/or oral tissues. The condition affected middle-aged to old cats without an apparent sex or breed predisposition. The most common clinical signs at initial presentation were exposure keratitis, severely restricted mobility of eyelids, and decreased retropulsion of the globe. Thickening of the eyelids, seen grossly and histologically, correlated with a diffuse dermal neoplastic infiltration and probably accounted for the clinical lagophthalmos. Cats with FROMS generally had a history of poor response to therapy, and in several cases, a previous biopsy specimen had been interpreted as being reactive. The clinical differential diagnosis for this presentation should include other orbital or eyelid neoplasms, orbital abscess or cellulitis, and chronic reactive fibrosing conditions.
Because all cases were obtained as postenucleation or postexenteration submissions, this study includes only those cases that were treated surgically; thus, it may be biased toward a more aggressive form of the disease. However, we are unaware of any cases, whether described in the literature or anecdotally, in which medical management of this disease has been successful in the long term. Based on the current study, the neoplasm typically spreads to adjacent tissues despite enucleation or exenteration. Clinical involvement of the contralateral orbit and/or lips and oral cavity generally occurs within 6 months of initial presentation. Most cats are euthanized owing to progressive disease within 9 to 12 months of initial presentation. A minority of cats have oral involvement at initial presentation, necessitating consideration of additional entities in the differential diagnosis, such as eosinophilic stomatitis, proliferative gingivitis, and primary oral neoplasms.
The regionally invasive nature of this tumor was readily evident with CT and MRI, with all 4 clinically affected eyes having distinct scleral/episcleral thickening. Furthermore, in 1 eye that was clinically unaffected at the time of MRI but affected at follow-up CT, the increase in the scleral/episcleral thickness was detected by imaging, consistent with the clinical progression. The loss of margination on CT of the retro-orbital soft tissues was a direct result of the obliteration of the surrounding contrast-providing adipose tissue by neoplastic infiltration and fibrosis.
Histologically, FROMS is characterized by bland spindle cells with moderate collagen deposition and low mitotic index. It is an infiltrative neoplasm that spreads along fascial planes and encircles preexisting tissues, causing atrophy of entrapped skeletal muscle and peripheral nerves, and it contributes to the mechanical restriction of the eyelids and globe. This restrictive effect may have a neurologic component, given that entrapped peripheral nerves with axonal degeneration were seen histologically.
Routine histologic examination of biopsy specimens with little or no clinical history may lead to misdiagnosis of FROMS as reactive fibrosis. However, the severity of the inflammatory component tends to be minor compared to the degree of spindle cell proliferation. Consideration of the distribution of neoplastic tissue should prove helpful to the surgeon in obtaining a biopsy specimen of diagnostic quality. Within the orbit, relatively more neoplastic tissue is in the anterior and superior aspect of the episclera. In the eyelids, the densest neoplastic infiltration is in the conjunctival substantia propria near the fornix. Based on our experience, the best tissues to submit for diagnosis are thickened eyelid, thickened haired skin with subcutis, or grossly abnormal orbital tissues that retain their orientation to the globe and/or eyelids. In the absence of a mass lesion, episcleral tissues may not be grossly interpreted as being neoplastic; consequently, they may be trimmed away from the globe. If there is a clinical suspicion of FROMS, the globe should be submitted for histologic evaluation with the eyelids and orbital tissues in place, contrary to the routine recommendation for dissection and fixation of enucleation specimens. Formation of a discrete mass or malignant cytological features are more likely to develop late in the course of the disease (eg, when the tumor has extended to oral tissue or filled the orbit postenucleation).
Even when grossly and clinically inapparent, there is local tumor infiltration into the substantia propria of the contralateral conjunctiva, the deep dermis and hypodermis of eyelids and skin of the face, and the nasal and oral lamina propria, as seen in the necropsy specimens. In all necropsy cases, destruction of bone was seen histologically, although it was not always apparent in CT images.
The immunohistochemistry profile suggests that FROMS is a myofibroblastic sarcoma. Positivity for S100 protein is not expected for a myofibroblastic neoplasm; however, in our experience, many tissues of the head—whether native or neoplastic—are positive for S100. This is presumably due to the neural crest origin of much of the facial mesenchyme. We attribute the inconsistent scattered expression of glial fibrillary acidic protein to fragments of peripheral nerves containing nonmyelinating Schwann cells.
Ocular trauma is common in cats and a potential confounding factor in the diagnosis of FROMS. In cases of trauma, the globe may have scleral rupture, retinal detachment, lens luxation, doubling of Descemet membrane, or iridal cysts. However, blunt trauma may present histologically as marked episcleral fibrosis in the presence of a relatively unreactive globe. Clinical history and follow-up are critical in such cases. In the present series of cases, there was no evidence of ocular trauma—from neither clinical history nor histopathology. We emphasize that FROMS is not a variant of feline posttraumatic sarcoma, given that the latter is characterized by severe distortion of the globe and unmistakable cellular features of malignancy. 7
The histologic features of FROMS are distinct from high-grade fibrosarcomas and peripheral nerve sheath tumors, both of which are reported in the orbit and/or eyelids of cats. 12,13 Within the COPLOW collection, peripheral nerve sheath tumor is the most common primary tumor of the feline eyelid. However, unlike FROMS, peripheral nerve sheath tumors tend to form a mass confined to an anatomic region; they display characteristic histologic patterns with malignant cytological features; they do not express smooth muscle actin; they are not associated with restricted mobility of the eyelids and globe; and they lack an accompanying inflammation.
In some regard, FROMS resembles the canine maxillofacial fibrosarcoma (CMF). Both tumors are locally invasive with low metastatic potential, and both share a misleading bland cytological profile. Unlike FROMS, canine maxillofacial fibrosarcoma tends to form a mass lesion, facilitating diagnosis as a discrete neoplastic process. Canine maxillofacial fibrosarcoma in dogs has been shown to metastasize, albeit infrequently. 5 There is currently no evidence of metastasis in cases of FROMS, and spread of the tumor is limited to local invasion.
The nomenclature and classification of infiltrative fibrosing disorders of the human orbit and other anatomic sites are inconsistent, with ill-defined and overlapping categories of neoplastic and inflammatory conditions in the literature. 1,8,9,14,18,21,26 These include, but are not limited to, aggressive fibromatosis, idiopathic sclerosing inflammation, inflammatory pseudotumor, nodular fasciitis, and desmoid tumors. More recently, several of these conditions have been incorporated under the umbrella of myofibroblastic lesions/tumors, with low-grade myofibroblastic sarcoma and inflammatory myofibroblastic tumor as the most common in humans. 8 A recent report described a retrobulbar inflammatory myofibroblastic tumor in a dog. 16 Isolated reports of similar proliferative and fibrosing lesions in anatomic sites remote from the orbit have been reported in the horse, 4,24,28 goat, 27 cat, 15,23 macaques, 11 and dogs. 3,6,10,16,29
A study by Qiu et al 25 compared inflammatory myofibroblastic tumors and low-grade myofibroblastic sarcoma in humans, concluding that the two are distinct clinicopathologic entities with key genetic and histologic differences. Inflammatory myofibroblastic tumors typically form a distinct mass lesion; they lack anatomic predilection sites; they have a heterogeneous histologic composition with a plasmacytic inflammatory component; and they are frequently associated with specific genetic rearrangement. In contrast, low-grade myofibroblastic sarcomas are grossly ill-defined and infiltrative; they have a predilection for the head and neck; they consist of a uniform population of bland myofibroblasts without significant inflammatory component; and they have no known specific genetic alterations. In an earlier review, Fisher 8 reported similar findings and further characterized low-grade myofibroblastic sarcomas as neoplasms that are unlikely to metastasize, that are rarely associated with necrosis, and that have increased cellular pleomorphism when the tumor recurs. These characteristics are strikingly similar to the more consistent features of the cases in the present series.
Immunohistochemistry using myoid markers may have limited usefulness in differentiating low-grade myofibrosarcomas from other myofibroblastic conditions, whether neoplastic or reactive. Although specific molecular markers have been proposed, including β-catenin 17,22 and fibronectin, 19 there are currently no immunologic markers with diagnostic specificity for myofibroblastic sarcomas. Ultrastructural analysis was not performed on any of the tissues from this study. Historically, myofibroblasts have been defined by their ultrastructural characteristics, although these criteria have been shown to lack specificity. 25
FROMS is a relatively uncommon tumor that occurs in middle-aged to older cats without apparent breed or gender predilection. Historically, reports of this entity in the veterinary literature used the name feline orbital pseudotumor. However, our results indicate that this condition represents a true neoplastic process based on proliferation of a monotonous cellular infiltrate with minimal inflammation and invasive behavior. Despite a bland cellular profile, FROMS has the malignant characteristics of infiltrative local spread, loss of function of associated tissues, and unfavorable clinical outcome. The name FROMS implies a malignant spindle cell neoplasm of cats and reflects the prominent clinical feature of restricted mobility of the eyelids and globe. Differentiating FROMS from traumatic and other neoplastic processes depends on recognizing characteristic features of the clinical presentation, imaging, pathology, and immunohistochemistry.
Footnotes
Acknowledgements
Special thanks to Sandy Cheasty, Barb Reese, and Mingyu Wang for assistance with histopathology and immunohistochemistry. We would like to thank Kate Lieber, Doris Dubielzig, and Gillian McLellan for their logistical support and helpful advice.