
Abstract
C hepatica, an important zoonotic parasite, and C fasciolaris are common parasites in rodents. In rodent livers, C hepatica causes sequential morphologic changes that are designated as early, intermediate, or late phase, and C fasciolaris forms cysts surrounded by fibroplasia and granulomatous inflammation. The present study describes the prevalence of these parasites and associated liver and lung lesions in wild rats (Rattus norvegicus) living around pig farms in South Korea. Selected parenchymal organs, including liver and lung, of 89 wild rats were examined. Of 89 rats, 28 (31.5%) were infected with either C hepatica or C fasciolaris or with both parasites. Severe medial hypertrophy of small arterioles was observed in the lungs of 11 of the 28 parasite-infected rats (P < .01). The pulmonary arteriolar hypertrophy in the rats infected with C hepatica was strongly associated with early and/or intermediate phases (88.8%) of morphologic change in the livers (P < .01). As such, this report is the first to suggest a significant association between parasite-induced hepatitis and pulmonary arteriolar hypertrophy in rodents. Further studies are warranted for the use of C hepatica–infected rats as an animal model to explore the underlying mechanisms of portopulmonary hypertension in humans.
C hepatica and C fasciolaris are common parasites causing hepatic diseases in wild rats—namely, hepatic capillariasis and cysticercosis, respectively. 11,20 C hepatica is a nematode belonging to the family Trichocephalidea and the class Tricuroidea. C hepatica is an important zoonotic parasite, 5 and its infection has been documented in more than 40 mammalian species, including rodents, 6 dogs, 18 cats, 24 nonhuman primates, 13,27 and humans. 3,4,22,31 C fasciolaris is the larval form of the cestode Taenia taeniaformis, also known as the cat tapeworm. 11,20
The pathogenesis of liver diseases caused by these two parasites is distinct and unique according to their life cycles. C hepatica infection results in multifocal granulomatous inflammation directly associated with the presence of live, dying, and dead worms and their eggs, followed by septal fibrosis. 2,12,25,30 T taeniaformis is the adult tapeworm that lives in the small intestine of carnivores such as cats, and rodents are the intermediate hosts. 20 The eggs of T taeniaformis develop into larvae, which form cysts in the liver parenchyma of rodents, inducing vigorous fibroplasia and progressive inflammation. 11,20 The fibroplastic and inflammatory lesions may often progress to fibrosarcoma. 14,36 Studies have used the rodent species infected with these parasites as potential animal models for the studies of hepatic fibrosis or cirrhosis 34,35 and parasitic carcinogenesis. 36
The liver is a primary organ involved in the maintenance of homeostasis, through metabolism, synthesis of proteins, formation of bile and clotting factors, and conjugation and detoxification of various compounds. 8 Additionally, the liver interacts with other major organs, including lung, heart, and kidney. Therefore, deleterious lesions in the liver may give rise to significant secondary adverse effects on the functions of other organs, as in the case of hepatopulmonary syndrome or portopulmonary hypertension in humans. 15,16 Hepatopulmonary syndrome is a well-defined cause of hypoxemia owing to abnormal intrapulmonary vascular dilatation in patients with liver disease, and portopulmonary hypertension is clinically defined by elevated pulmonary arterial pressure evidenced by arterial/arteriolar medial hypertrophy, secondary to the hepatic diseases. 15,16
In the present study, we report the prevalence of the hepatitis-inducing parasites C hepatica and C fasciolaris in wild rats (Rattus norvegicus) captured around pig farms in South Korea, and we describe morphologic changes that provide a possible association between parasite-induced liver disease and pulmonary lesions in these animals.
Materials and Methods
A total of 89 wild rats were captured using wire traps from areas around eight selected pig farms in Gyeonggi province and 3 farms in Gangwon province, Republic of Korea. The rats were euthanized with ethyl ether and subjected to the necropsy at the Laboratory of Histology and Molecular Pathogenesis, School of Veterinary Medicine, Kangwon National University. Following gross examination, major organs, including lung, heart, gastrointestinal tracts, liver, kidney, and urogenital organs, were fixed in 10% neutral-buffered formalin solution, processed routinely for paraffin embedding, sectioned at 5 µm, and stained with hematoxylin and eosin. Parasite infection was determined by histologic identification of eggs or worms in the liver. Liver lesions associated with C hepatica infection were further classified as early, intermediate, or late phase, based on published criteria. 2
Statistical Methods
Correlations between pulmonary lesions and parasite infection or histologic phases of C hepatica–induced hepatic changes were evaluated by chi-square test of independence. Significant relation between the comparative groups was determined at P < .05.
Results
Prevalence and Histologic Classification of Parasite Infection
On gross and microscopic examination, 28 of 89 wild rats (31.5%) were infected with C hepatica and/or C fasciolaris (Table 1 ). Of the 28 infected rats, 12 rats were infected with C hepatica only, 7 with C fasciolaris only, and 9 rats were infected with both parasites (Table 1). No histologic evidence of other parasitic infection was present in livers examined.
Infection of Hepatitis-Inducing Parasites and Its Association With Pulmonary Arteriolar Hypertrophy
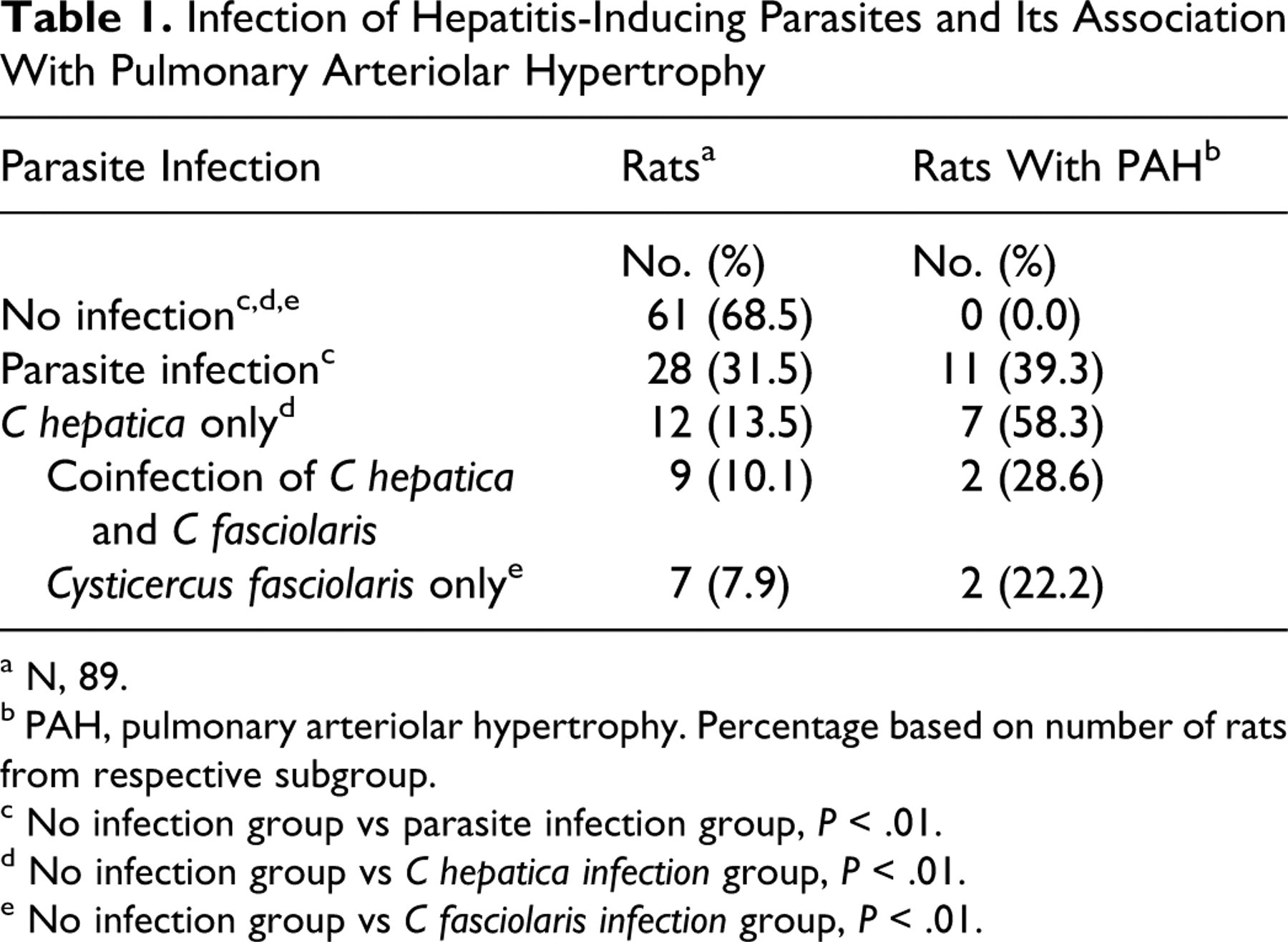
a N, 89.
b PAH, pulmonary arteriolar hypertrophy. Percentage based on number of rats from respective subgroup.
c No infection group vs parasite infection group, P < .01.
d No infection group vs C hepatica infection group, P < .01.
e No infection group vs C fasciolaris infection group, P < .01.
Grossly, in livers of C hepatica–infected rats, there were 0.1- to 0.5-mm-wide curled whitish tracts with indistinct borders under the liver capsule (Fig. 1) and, occasionally, 1- to 3-mm tan spots scattered along the serosal surface and on cut section. Livers infected with C fasciolaris comprised variable numbers of cysts, ranging from 0.6 to 2.0 cm in size, deeply embedded within the liver parenchyma. The cysts contained 15- to 28-cm-long coiled white viable larvae with a prominent scolex and a long neck (inset in Fig. 1) consistent with C fasciolaris, the larval form of Tania taeniaformis in carnivores. Gross and microscopic lesions suggestive of portosystemic shunts or portal and cardiac circulation disorders were not observed in any of the rats examined.
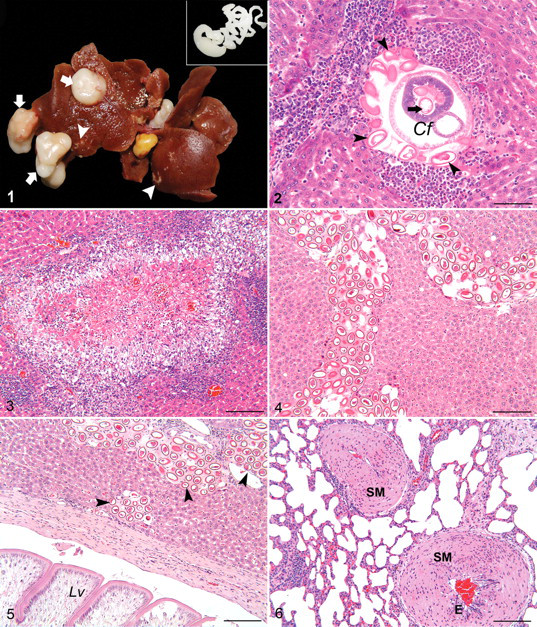
According to the aforementioned criteria, 2 C hepatica–infected livers in these rats were classified into 3 phases based on morphologic changes: early, intermediate, and late. The early phase was characterized by the presence of live juvenile or mature worms and oval-shaped eggs with bipolar plugs, associated with multifocal mild-to-moderate granulomatous hepatitis, accompanied by eosinophil, macrophage, and lymphocyte infiltration (Fig. 2). The intermediate phase was determined by the presence of degenerate or mineralized worms and egg clusters, associated with a more severe multifocal granulomatous hepatitis and fibrosis (Fig. 3). The late phase was characterized by the absence of the worms in the liver parenchyma, resolving granulomatous lesions, and residual fibroplastic and calcified lesions containing clustered eggs (Fig. 4). Septal hepatic fibrosis was also observed in the late phase. Among the 21 animals with C hepatica–associated liver lesions, 4 were classified as early phase, 5 as intermediate phase, and 12 as late phase (Table 2 ).
Prevalence of Pulmonary Arteriolar Hypertrophy in C hepatica–Infected Rats by Morphologic Phases of Liver Change a
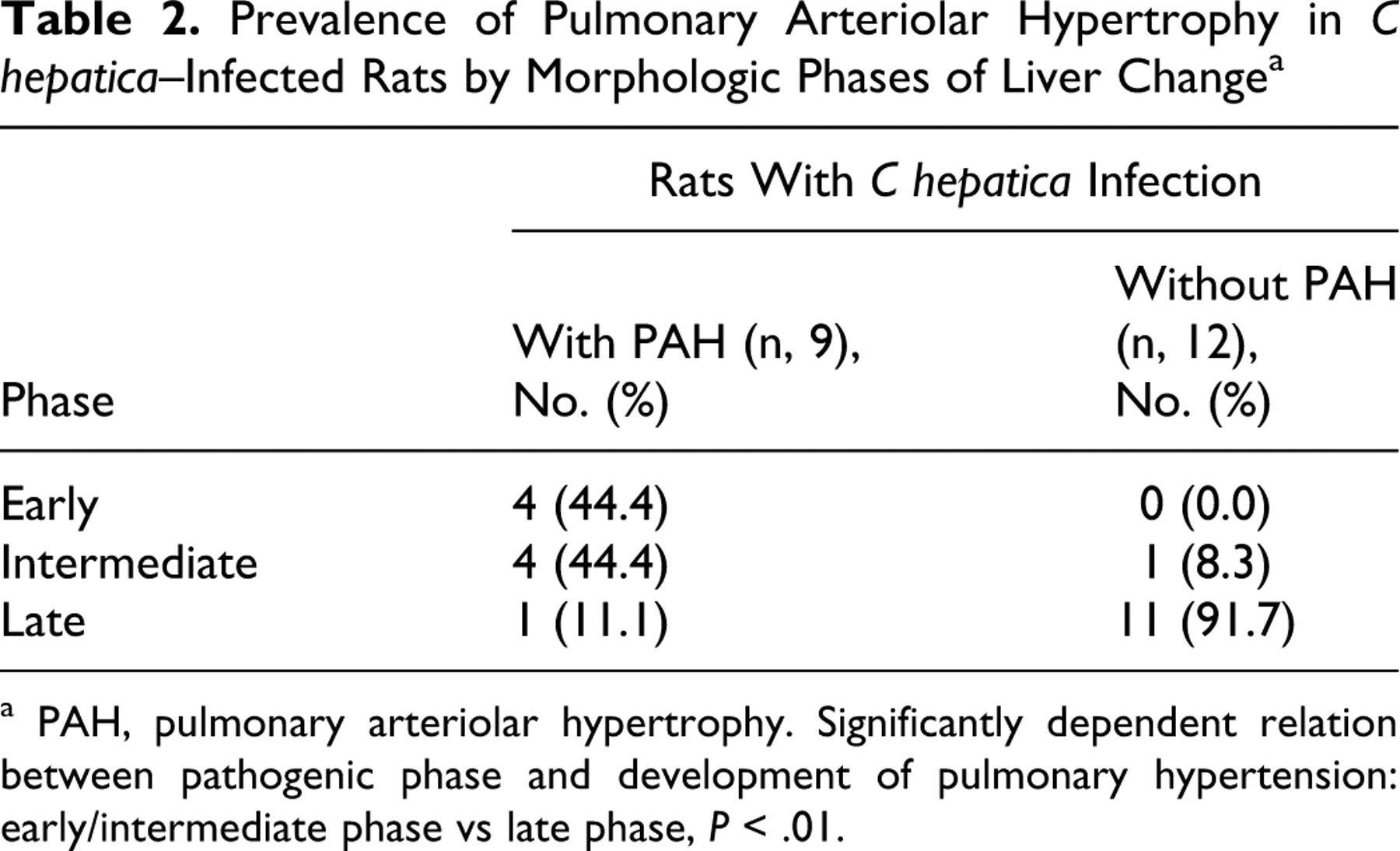
a PAH, pulmonary arteriolar hypertrophy. Significantly dependent relation between pathogenic phase and development of pulmonary hypertension: early/intermediate phase vs late phase, P < .01.
In rats infected with C fasciolaris, the presence of larvae-containing hepatic cysts and progressive inflammatory and fibrotic lesions was observed (Fig. 5). Histologically, the larvae were characterized by the sucker at the anterior end and 2 zones of muscle fibers in the body parenchyma. The parasitic cysts were surrounded by connective tissue associated with mild infiltrates of lymphocytes or severe inflammatory infiltrates predominantly composed of lymphocytes and macrophages as well as moderate numbers of eosinophils. Rupture of the cyst wall was associated with the formation of granulomas characterized by epitheloid macrophages, lymphocytes, and eosinophils.
Association of Parasite-Induced Hepatic Lesions With Pulmonary Arteriolar Hypertrophy
Out of 89 rats examined, 11 had medial hypertrophy of the pulmonary arterioles, which was characterized by proliferation of smooth muscle cells, resulting in a marked thickening of the tunica media and narrowing of the arteriolar lumen (Fig. 6). Interestingly, all rats with medial hypertrophy of the pulmonary arterioles were infected with hepatic parasites: 7 rats with C hepatica only, 2 rats with C fasciolaris only, and 2 rats with both parasites (Table 1). Of the 9 rats with C hepatica infection and pulmonary arteriolar hypertrophy, 4 were in the early phase of liver change, 4 were in the intermediate phase, and 1 was in late phase (Table 2). All animals that were infected with C hepatica but did not have pulmonary arteriolar medial hypertrophy were in the late phase (Table 2). These findings suggest a strong linkage between hepatitis induced by C hepatica infection and pulmonary arteriolar hypertrophy (P < .01) (Table 2).
Discussion
C hepatica is a common hepatic parasite in rodents that is also an important zoonotic parasite. C hepatica has a range of mammalian hosts, many of which are closely associated with humans, increasing the likelihood of human infection. 6,13,18,24,27 Although human infection is rare, it is reported to be relatively more frequent in children. 3,4,7,22,31 The prevalence of C hepatica infection in rodents is reported worldwide with variable infection prevalence ranging from 7.9% to 88.0%. 6,21,23,32,33,37 In the present study, 23.6% of captured wild rats from the selected areas of Korea were infected with C hepatica. Hepatic lesions associated with C hepatica infection can be classified into early, intermediate, and late phases. 2 This classification scheme represents the sequential histopathologic changes associated with disease progression, including development and death of the parasites and their eggs, the resolution of inflammation and removal of parasites, and progression of septal fibrosis. 2,12 In the present study, hepatic lesions in rats with C hepatica infection were similar to those described in previous studies 2,12 and could be classified as early, intermediate, and late phases according to the published criteria. 2
An interesting finding in the present study was a strong correlation between parasite infection and pulmonary arteriolar medial hypertrophy (P < .01), as characterized by thickening of the tunica media and recognized as a response to pulmonary hypertension. 17 All rats that had pulmonary arteriolar medial hypertrophy were infected with either C hepatica or C fasciolaris, suggesting a strong association between parasitic infection and development of the pulmonary lesion. Furthermore, 9 of the 11 rats with pulmonary arteriolar medial hypertrophy were infected with C hepatica, suggesting that development of pulmonary arteriolar hypertrophy was more likely associated with C hepatica infection than with C fasciolaris. The pulmonary arteriolar hypertrophy was strongly correlated with the inflammatory phase of liver disease associated with C hepatica infection (P < .01). Of 9 C hepatica–infected rats with pulmonary arteriolar hypertrophy, 8 were in the early to intermediate phases whereas only 1 was in the late phase. Most rats with late-phase hepatic lesions had no pulmonary lesions. Hepatic lesions in early and intermediate phases were characterized by multifocal granulomas encompassed by fibrosis that resulted in distortion of the normal hepatic architecture as well as disruption of normal intrahepatic and portal circulation. However, the late-phase lesions were characterized by diffuse and mild bridging septal fibrosis with no disruption of intra- or extrahepatic circulation. These findings indicate that pulmonary hypertension presumably develops during the early to intermediate phases and resolves at the late phase. Further studies are necessary to determine the exact mechanism underlying the development of the pulmonary lesion.
In support of our speculation, pulmonary hypertension is frequently found in human patients with chronic liver disease. 15,16,19 Pulmonary hypertension is considered a significantly deleterious condition that has a substantial impact on survival of human patients with liver disease. 15 Therefore, it is important to understand the mechanism by which liver disease contributes to pulmonary hypertension. To date, the incidence of liver disease–associated pulmonary hypertension in humans has been shown to vary greatly, ranging from 0.73% to 16.0% depending on the severity of liver disease. 28 Furthermore, its pathogenesis is poorly understood and still speculative, despite the implication of various vasoactive mediators (serotonin, interleukin 1, endothelin 1, glucagon, secretin, thromboxane B2), venous thromboembolism, and increased vascular shear stress in its pathogenesis. 9,10,26 Individual variation is a critical limitation in illustrating a reliable relationship between hepatic impairment and pulmonary hypertension, as well as determining its underlying mechanism. In particular, the molecular mechanisms have been hypothesized on the basis of general studies on primary pulmonary hypertension 1,10,29 rather than a cause–effect relationship between liver and lung. In the present study, the incidence of the pulmonary lesion was in 42.8% of C hepatica–infected rats. It is interesting that 88.8% of the C hepatica–infected rats with severe hepatic lesions at early/intermediate phases suffered from pulmonary hypertension. Based on the findings, we speculate that C hepatica–infected rats may be useful as an animal model for the studies of portopulmonary hypertension.
In conclusion, C hepatica and/or C fasciolaris infection was found in the livers of wild rats captured in South Korea (31.5%), and hepatic lesions caused by C hepatica were closely associated with pulmonary arteriolar hypertrophy, which may represent the effects of pulmonary hypertension. Our results provide a clue of a cause–effect relationship between parasite-induced hepatic disease and pulmonary hypertension, which warrants further physiologic and pathologic studies in terms of the use of C hepatica–infected rats as an animal model for portopulmonary hypertension in humans.
Footnotes
Acknowledgements
We thank Dr Mark J. Hoenerhoff at NIEHS for his constructive review of this article. B.-I. Yoon also gives thanks for the financial support of Kangwon National University and LG Yonam Foundation during a sabbatical year (2009) at College of Veterinary Medicine, North Carolina State University, Raleigh.
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by a grant (Project Code No. Z-AD12-2007-07-02) from National Veterinary Research and Quarantine Service, Ministry of Agriculture, in 2007.