
Abstract
Canine inflammatory mammary cancer (IMC) and human inflammatory breast cancer (IBC) are the most aggressive and lethal type of mammary cancer in female dogs and in women. The generation of microvascular channels by malignant tumor cells (endothelial-like cells [ELCs]) without endothelial cell participation (vasculogenic mimicry) has been reported in human breast cancer, including IBC, and is considered a new type of tumor angiogenesis. The aim of this study was to investigate the presence of ELCs in highly malignant canine mammary tumors (IMC and non-IMC) by histology, inmunohistochemistry (pancytokeratin, cytokeratin 14, vimentin, actin, desmin, vWF, CD31, and CD34), and electron microscopy. This retrospective study included 21 female dogs with diagnoses of IMC and 20 animals with metastatic grade III noninflammatory malignant mammary tumors (MMT). IMC tumors (33.33%) and MMT (5%) showed ELCs forming structures similar to small capillaries. The histological, immunohistochemical (positive to AE1/AE3 and cytokeratin 14, mostly negative to endothelial markers), and ultrastructural characteristics of these cells indicated vasculogenic mimicry. The higher frequency of this phenomenon in inflammatory versus noninflammatory canine mammary cancer is in agreement with previous studies in experimental and spontaneous human IBC, and it could be in relation with the extremely high lymphangiogenic capacity and metastatic lymphangiotropism characteristics of inflammatory breast cancer.
Keywords
Inflammatory mammary cancer (IMC) is the most aggressive and lethal type of mammary cancer in female dogs 49,69 and in women, 20-22,33,52 in spite of the new multimodality therapies used in the human patients. 21,64,74 Canine IMC and human inflammatory breast cancer (IBC) share clinical and histological characteristics; therefore, canine IMC has been proposed as a potential natural model for study of the human disease. 47 In both species, this uncommon type of tumor is a locally invasive mammary cancer that can be clinically misdiagnosed as a dermatitis or mastitis owing to its special inflammatory phenotype. 32,49,52 Although the pathogenesis of the disease remains obscure, some special clinical, genetic, biologic, and hormonal characteristics have been found to be specific for IBC 5,20,32,70 and IMC. 31,47-49,54 The term inflammatory is due to the clinical features of this type of cancer in dogs 49,69 and women, 12,20,21,33,52,70 which include sudden presentation, edema, erythema, and firmness and warmth of the mammary glands, with or without mammary nodules. Beside this, IMC in dogs is characterized by a fulminant clinical course, given that the only treatment usually applied is palliative. 49 Two clinical forms of IMC have been described in dogs 49 and women. 1,52,71 Primary IMC refers to IMC occurrence in a dog without previous history of mammary nodules, whereas secondary IMC includes IMC occurrence in a dog with previous mammary tumors. Secondary IMC is further classified into two types: postsurgical secondary (IMC after surgical excision of a previous mammary tumor) and non-postsurgical secondary (a previous mammary tumor not surgically treated that leads to IMC). Histologically, several types of highly malignant mammary carcinomas have been described in canine IMC 47,49 and human IBC. 32,52,71 The hallmark for the histological confirmation of IMC 47,49 and IBC 3,6,52 is the invasion of dermal lymphatic vessels by neoplastic emboli. Clinical and histological features of IMC should be present for a proper diagnosis of the disease. 65
IBC is a highly angiogenic and lymphangiogenic tumor. 77 The term angiogenesis describes the formation of new vessels from preexisting vessels in the adult. 37 According to recent advances, tumor angiogenesis can be produced through endothelial precursor cells from the bone marrow, from endothelial cells of preexisting vessels, 13,37 by sprouting angiogenesis, 13,17 by intussusceptive angiogenesis, 5,13 and by vessel co-option. 13,30 In addition, a new mechanism of tumor angiogenesis has been discovered: the vasculogenic mimicry (VM) phenomenon. 42 VM consists in de novo generation of microvascular channels by genetically deregulated, aggressive tumor cells without endothelial cell participation. 18,42 The name was coined to describe the formation of these channels by aggressive tumor cells: vasculogenic, because the channels are not formed from preexisting vessels, despite the fact that they distribute plasma and may contain red blood cells; and mimicry, because the channels are not true blood vessels but merely mimic the function of vessels. 18,42
VM was firstly recognized in aggressive human melanomas. 42 After this initial observation, other studies have reported the evidence of VM in several malignant human tumors, such as cutaneous melanoma, 72,81 ovarian carcinoma, 66 oral mucous melanoma, 38 prostatic carcinoma, 39,57 synovial sarcoma, 26 pheochromocytoma, 16 rhabdomyosarcoma, 27 mesothelial sarcoma, 68 hepatocellular carcinoma, 25 inflammatory breast carcinoma, 36,58-60,62,63 and ductal breast carcinoma. 4 VM was observed in a human IBC mouse xenograft model (WIBC-9) by electron microscopy and immunohistochemistry and in vitro cell growth of WIBC-9 cells. 62 Additionally, VM was histologically observed on stained (hematoxylin and eosin [HE]) paraffin sections from patients with IBC (15.8%) and noninflammatory breast cancer (7.4%), suggesting that the VM phenomenon is more common but not exclusive of IBC. 63
Our previous experience in the histopathology of canine IMC 31,47-49 led us to observe some neoplastic cells sharing histological characteristics with endothelial cells, possibly in relation to the VM phenomenon. Thus, based on this hypothesis, the purpose of this study was to investigate the possible presence of these endothelial-like neoplastic cells in canine mammary tumors (IMC and noninflammatory mammary cancer–comparable malignant mammary tumors [MMT]) and to characterize their immunophenotype by immunohistochemistry.
Materials and Methods
Animals
This is a retrospective study of 41 female dogs, 21 animals with clinical and pathological IMC (mean age, 10.94 ± 2.31) and 20 animals with comparable metastatic grade III noninflammatory MMT (mean age, 10.69 ± 3.14), attended at the Veterinary Teaching Hospital of the Complutense University of Madrid (VTHM) over a period of 13 years, between January 1995 and June 2008.
A complete medical record and history of reproductive status was obtained. Information about the tumor was also recorded in all cases, both IMC and MMT (growth rate, size, location, pain, previous surgery or not, type of IMC). In addition, a complete physical exam and radiological evaluation of the thorax (2 lateral projections) were performed (and, in some cases, abdominal ultrasonography) to investigate the presence of metastases. Surgical resection of the mammary nodules and subsequent histological diagnosis of surgical specimens were performed in all dogs from the MMT group.
After the diagnosis, the dogs in both groups were followed up until euthanasia. Necropsies were performed under consent of the owners.
Diagnostic Procedures: Samples
IMC
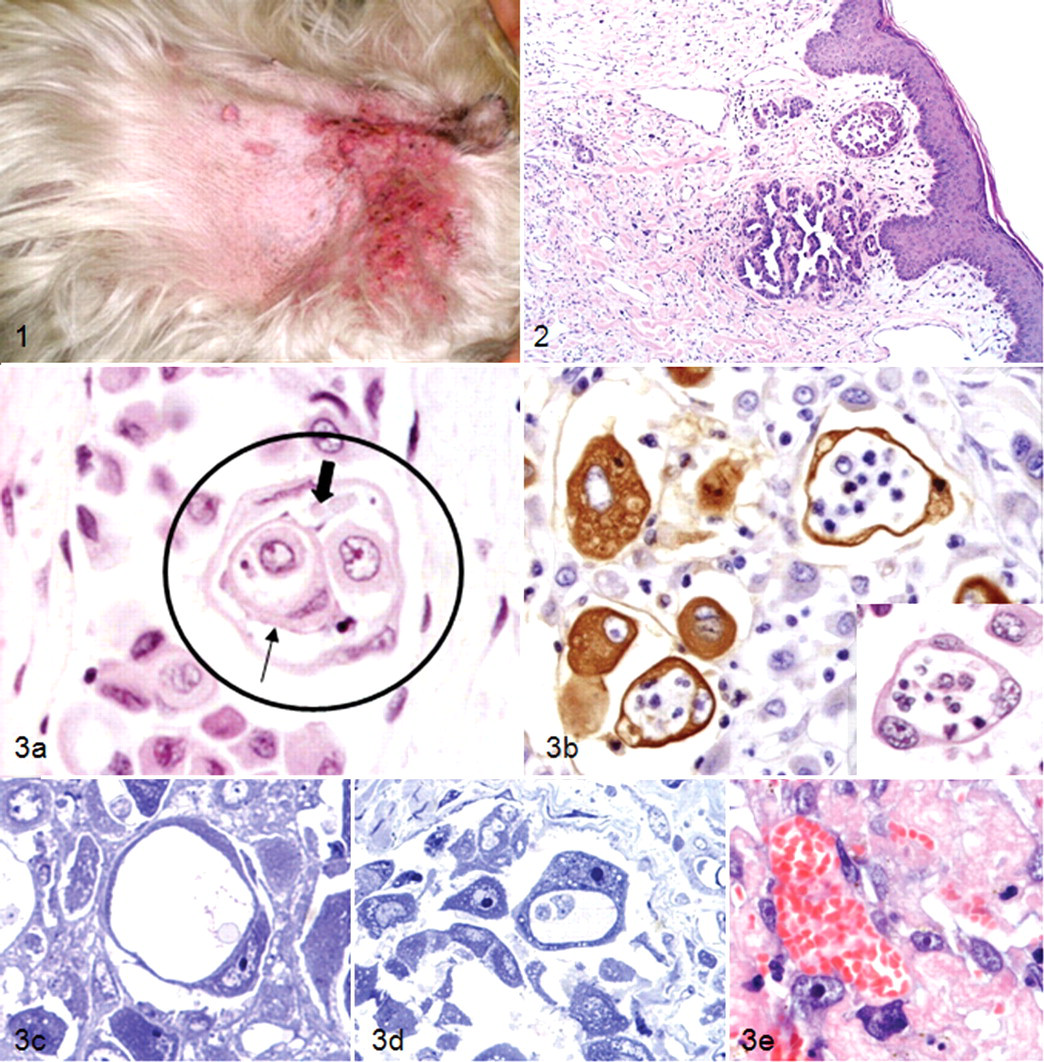
Only cases with clinical and histopathological diagnoses were included. Clinical diagnosis of IMC was based on features previously described in dogs. 49,69 IMC was suspected in dogs with rapidly growing disease of the mammary glands and overlaying skin, characterized by diffuse involvement of multiple glands (with or without mammary nodules), firmness, warmth, edema, erythema, thickening, and signs of pain (Fig. 1 ). IMC cases (n = 21) were histologically diagnosed either by Tru-cut biopsies or by necropsy specimens submitted to the Veterinary Pathology Service of the VTHM. In each case, fragments of the tissues were fixed in neutral formalin and paraffin embedded. The samples were histologically diagnosed on HE-stained sections following the World Health Organization’s classification of canine mammary tumors. 44 Clinical IMC was histologically confirmed when numerous neoplastic emboli in superficial dermal lymphatic vessels were observed 47,49 (Fig. 2 ).
Noninflammatory MMT
Noninflammatory MMT (n = 20) were either surgical or necropsy specimens submitted for diagnosis to the Veterinary Pathology Service of the VTHM. In each case, fragments of tissue were fixed in neutral formalin and paraffin embedded. The histopathologic exam was done following the World Health Organization’s classification of canine mammary tumors. 44 To select MMT that were comparable to IMC cases (in terms of clinical and histological malignancy), only malignant mammary tumors of histological malignant grade (HMG) III with distant metastases were included.
The HMG was established in IMC and MMT groups following a modification of the commonly used numeric method of Elston and Ellis
15
for grading human breast tumors, adapted to canine mammary tumors. The system was as follows:
Tubular formation (1 to 3 points): 1 = formation of tubules in > 75% of the specimen; 2 = moderate formation of tubular arrangements (10 to 75%) admixed with areas of solid tumor growth; 3 = minimal or no tubule formation (< 10%).
Nuclear pleomorphism (1 to 3 points): 1 = uniform or regular small nucleus and occasional nucleoli; 2 = moderate degree of variation in nuclear size and shape, hipercromatic nucleus, and presence of nucleoli (some of which can be prominent); 3 = marked variation in nuclear size and hipercromatic nucleus, often with one or more prominent nucleoli.
Mitotic rate (1 to 3 points): The tumor is scored 1 to 3, depending on the number of mitotic figures per 10 selected high-power fields (HPF; 40×; Olympus microscope: 22 mm; Olympus America Inc., Center Valley, PA). The fields are selected at the periphery or the most mitotically active parts of the sample: 1 = 0 to 9 mitotic figures per 10 HPF; 2 = 10 to 19 mitotic figures per 10 HPF; 3 = 20 or more mitotic figures per 10 HPF.
The HMG of the tumor is the sum of the points of the three features evaluated (tubular formation + nuclear pleomorphism + mitotic rate): HMG I = 2 to 5 points, well differentiated; HMG II = 6 or 7 points, moderately differentiated; HMG III = 8 or 9 points, poorly differentiated. Tumors with neoplastic emboli are also considered HMG III.
In both groups of tumors (IMC and MMT), Sudan III–stained cryostat sections were evaluated to confirm or rule out the lipid nature of the tumors.
Histopathological evaluation of endothelial-like cells
HE slides from all the tumors included (21 IMC and 20 noninflammatory mammary cancer [metastatic MMT, grade III]) were evaluated for 2 observers to detect the presence or absence of highly malignant neoplastic cells resembling endothelial cells— denominated endothelial-like cells (ELCs). A systematic evaluation of the entire tumor sample was performed in each case, using optical microscopy (40×). The presence of ELCs (VM) was established when, according to the morphology, highly malignant tumor cells sharing features with endothelial cells were observed: either groups of cells arranged forming a channel or individual neoplastic cells showing a large cytoplasmatic central space suggestive of a channel lumen resembling a single-cell capillary. For the purposes of being strict, only those structures containing other neoplastic or blood cells were considered to be ELCs. The last requirement, with the negative staining to Sudan III, was used to distinguish them from lipid-rich cells.
Immunohistochemical study
Immunohistochemistry of lineage and endothelial markers was performed on deparaffined sections using the streptavidin–biotin–complex peroxidase method. Table 1 shows the antigen unmasking technique and the primary antibodies used. After the incubation with the mouse monoclonal primary antibodies—pan-cytokeratin (CK), cytokeratin 14 (CK 14), vimentin, smooth muscle actin, desmin, and CD34—the slides were washed and incubated with anti-mouse biotinylated secondary antibody (1:400, 30 minutes at room temperature; BA-2000, Vector Laboratories, Burlingame, CA). After the incubation with the polyclonal rabbit antibody (von Willebrand factor), the slides were washed and subsequently incubated with anti-rabbit biotinylated secondary antibody (1:200, 30 minutes at room temperature; E 0353, DakoCytomation, Glostrup, Denmark). Next, all the slides were incubated with streptavidin conjugated with peroxidase (1:400, 30 minutes at room temperature; empleated peroxidase, No. 43-4323, Zymed, San Francisco, CA). For CD31 immunostaining, the slides were preincubated with ultrablock (prediluted, 10 minutes at room temperature; ultrasensitive kit, streptavidin–biotin–complex peroxidase, MLINK: MAD-001828QK, Master Diagnostica, Spain) and incubated with the primary monoclonal antibody anti-CD31; after washing, the slides were incubated with a secondary multilink antibody (prediluted, 10 minutes at room temperature; ultrasensitive kit, streptavidin–biotin–complex peroxidase, MLINK: MAD-001828QK, Master Diagnostica, Spain). All washes and dilutions were made in Tris-buffered saline (pH 7.4). All the slides were developed with a chromogen solution containing 25 g of 3-3′diaminobenzidine tetrachloride (No. D5059, Sigma, St. Louis, MO) and 100 μl of hydrogen peroxide in 100 ml of distilled water and counterstained in hematoxylin (No. GH5-2-16, Sigma). Technical data on specific antibodies are given in Table 1.
Technical data and specific cellular lineage and vascular markers. a
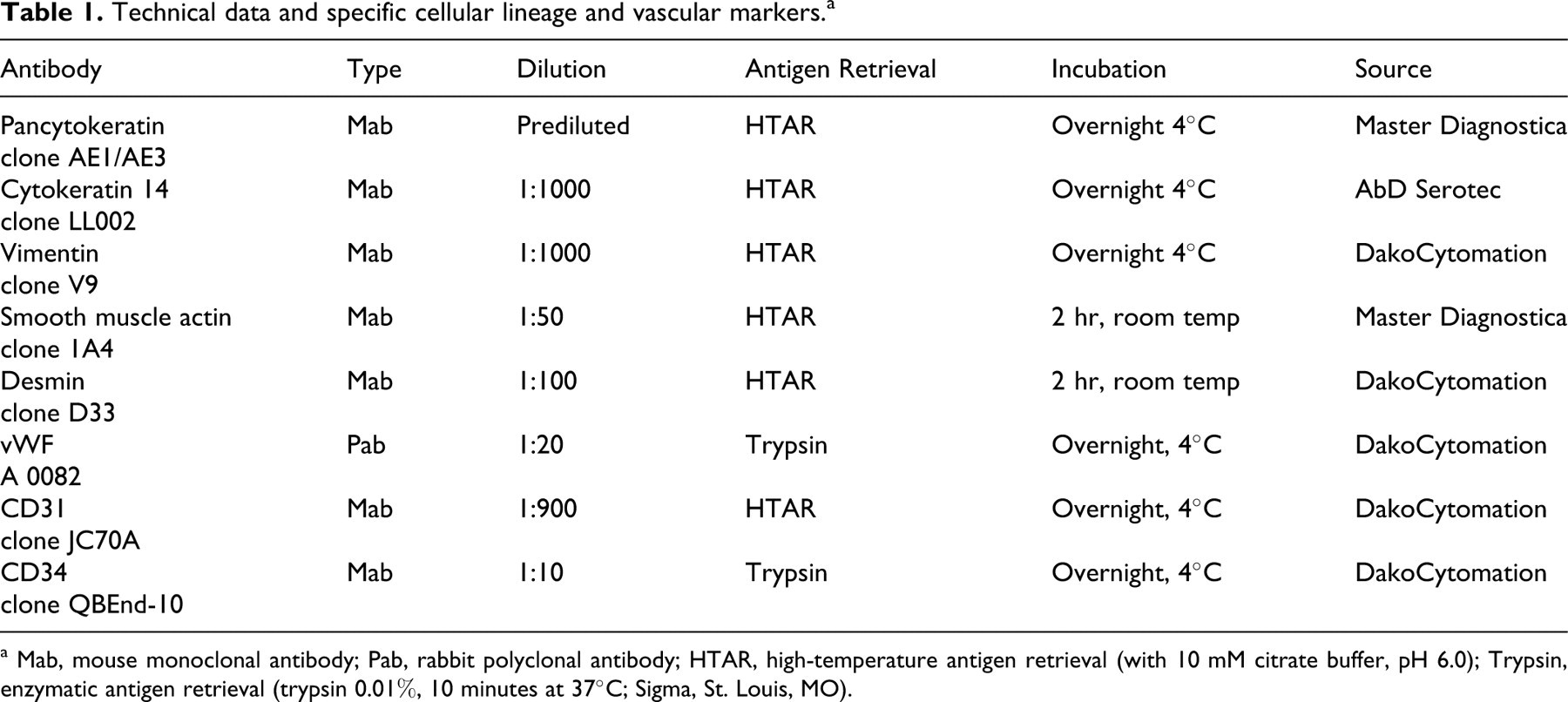
a Mab, mouse monoclonal antibody; Pab, rabbit polyclonal antibody; HTAR, high-temperature antigen retrieval (with 10 mM citrate buffer, pH 6.0); Trypsin, enzymatic antigen retrieval (trypsin 0.01%, 10 minutes at 37°C; Sigma, St. Louis, MO).
Corresponding negative control slides were done by replacing the primary antibody with Tris-buffered saline. In some cases, internal positive controls were used. The positive controls were as follows: canine normal mammary gland (CK and CK 14), smooth muscle cells of blood vessels (internal positive control for smooth muscle actin and desmin), and canine hemangiosarcoma (vWF, CD31, and CD34).
The evaluation of the immunostaining was performed by 2 observers simultaneously. The tumors were considered positive to the markers CK, CK 14, vimentin, actin, and desmin when more than 80% of the neoplastic cells were positive. The immunostaining of ELCs was separately evaluated for all the markers studied (CK, CK 14, vimentin, actin, desmin, vWF, CD31, and CD34); the intensity of immunoexpression was classified as low (+), moderate (++), or intense (+++).
Electron microscopy
Selected formalin-fixed mammary tissue samples (n = 5) of IMC tumors that exhibited ELCs by histology were processed for electron microscopy. The samples were washed in a phosphate buffer (pH 7.2; 24 hours at 4°C) to eliminate the formalin and immersed in 1% osmium (diluted in phosphate buffer) for 1 hour at room temperature. Then, they were washed in distilled water, dehydrated in acetone of increasing concentrations (30, 50, 70, 80, and 100%), gradually infiltrated in a Müllenhauer mixture resin, and solidified at 60°C for 24 hours. The resin blocks were then processed and studied in the Electron Microscopy Centre of the Complutense University of Madrid, Spain.
Results
Diagnosis of IMC and MMT
Different histological types of MMT were diagnosed in both groups (IMC and MMT) on stained sections (HE and Sudan III) and by means of the evaluation of the lineage cellular markers immunostaining. The 21 IMC neoplasms were classified as follows: simple tubular/papillary carcinoma (n = 9), lipid-rich carcinoma (n = 5), anaplastic carcinoma (n = 4), simple solid carcinoma (n = 2), and squamous cell carcinoma (n = 1). The observation of comedo-type formations was very frequent in the IMC group (8 of 22, 38.09%). Histological classification of the 20 noninflammatory mammary cancer neoplasms (MMT) was as follows: simple/complex solid carcinoma (n = 7), carcinosarcoma (n = 5), anaplastic carcinoma (n = 2), malignant myoepithelioma (n = 2), simple tubular carcinoma (n = 1), complex tubulopapillary carcinoma (n = 1), sarcoma (n = 1) and osteosarcoma (n = 1).
Endothelial-Like Cells
Histopathology
Of the 41 canine mammary cancers included, 7 of the 21 IMC cases and 1 of 20 MMT cases showed highly malignant neoplastic cells resembling endothelial cells (ELCs). This type of cell was not observed in the rest of the tumor samples.
ELCs were observed in two locations: inside neoplastic emboli and infiltrating the stroma. The ELCs were found in groups, forming structures similar to small capillaries or as individual neoplastic cells with similar morphology to a capillary formed by one cell (VM; Fig. 3). The same tumor could have groups and/or individual ELCs in the two locations. All ELCs were negative to Sudan III.
Isolated ELCs were round giant cells (140 to 200 μm), with distinct cell borders and scant cytoplasm surrounding a big central space like a rim. The nuclei were large (karyomegaly), oval, and eccentric, with finely stippled chromatin. Hyperchromatic nuclei were also frequent. Numerous and prominent nucleoli were characteristic. The cells presented marked cytological features of malignancy, such as anisokaryosis, anisocytosis, and multinucleation. The main characteristic of these cells was the presence of the central space (channel; VM) containing a variable number (n = 1 to 14) of tumor and/or blood cells (lymphocytes and neutrophils and, less frequently, erythrocytes). Some ELCs could appear in groups forming larger channels. These channels were covered by large and flattened ELCs (n = 2 to 14), with evident nuclear and cytoplasmic characteristics of malignancy, and they contained other tumor cells and/or blood cells (leukocytes more common than erythrocytes; Fig. 3).
The IMC neoplasms that presented ELCs were as follows: anaplastic carcinoma (n = 2), simple tubular carcinoma (n = 2), simple papillary carcinoma (n = 1), squamous cell carcinoma (n = 1), and lipid-rich carcinoma (n = 1). In the MMT group, the ELCs were found only in an anaplastic carcinoma.
The number of ELCs was different among the tumors: ELCs were abundant in 5 of 7 IMC cases and in the unique MMT case that showed the VM phenomenon.
Immunohistochemistry
Table 2 summarizes the immunostaining of ELCs. In each case, the immunostaining of ELCs was consistent with that of the majority of the tumor cells. For each antibody, the positive controls showed intense (+++) immunostaining (normal epithelial mammary gland cells for CK and CK14, smooth muscle cells for smooth muscle actin and desmin, and normal endothelial cells for vWF, CD31). CD34 stained only some endothelial cells in the control samples.
Immunohistochemistry of endothelial-like cells. a
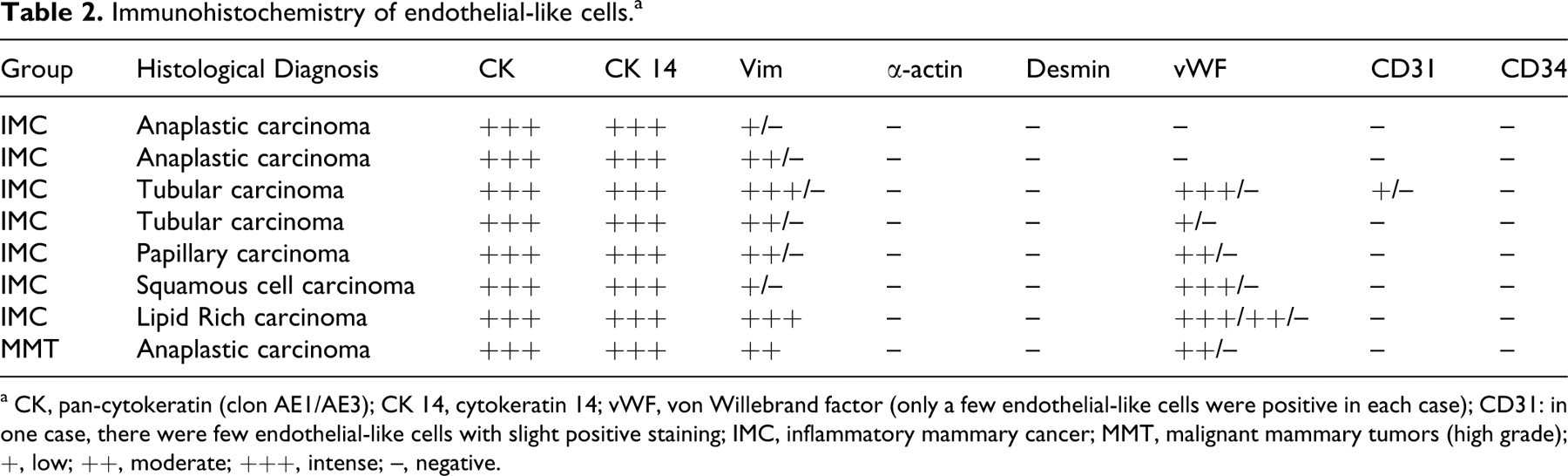
a CK, pan-cytokeratin (clon AE1/AE3); CK 14, cytokeratin 14; vWF, von Willebrand factor (only a few endothelial-like cells were positive in each case); CD31: in one case, there were few endothelial-like cells with slight positive staining; IMC, inflammatory mammary cancer; MMT, malignant mammary tumors (high grade); +, low; ++, moderate; +++, intense; –, negative.
Electron microscopy
Ultrastructurally (Fig. 4 ), the central spaces formed by the ELCs (individual or in groups) were empty spaces without any secretion; furthermore, they were limited by a cytoplasmic membrane and occupied by blood or tumor cells (degenerated or not) that were not inside vacuoles. The junction between ELCs was through desmosomes. The cytoplasm of ELCs was thin and scant with abundant rough endoplasmic reticulum, ribosomes, lysosomes, and mitochondria in scant number. The Weibel-Palade bodies, characteristic of endothelial cells, were absent. The nuclei were large, with granular chromatin and one or more prominent nucleoli.

Discussion
The present study describes the presence of highly malignant neoplastic cells resembling endothelial cells (ELCs) in canine mammary cancer, including IMC. The histological, immunohistochemical, and ultrastructural characteristics of these cells indicated VM. According to some authors, 18,36,42,62,66 tumors might have the potential to feed themselves via alternative pathways by vascular channels covered by deregulated neoplastic cells. Until the discovery of VM in human melanomas, the assumption was that all intratumoral vascular channels were formed and lined by endothelial cells. However, after demonstration of the VM phenomenon, researchers have accepted that endothelial cell–mediated angiogenesis is not the only mechanism responsible for tumor growth and metastasis. 42 Evidence of VM has been described in several malignant tumor types in humans by experimental studies 39,57,66 and by the direct observation on human tumor paraffin sections. 16,26,27,38,66,72,81 VM has been also described in experimental and spontaneous malignant breast cancer. 4,36,58,60-63 To our knowledge, there are no previous studies of VM in spontaneous animal tumors, including canine mammary tumors and IMC.
In the present study, 41 specimens of highly malignant canine mammary tumors were examined for the evidence of VM, using HE, immunohistochemistry, and electron microscopy: 21 specimens of IMC and 20 specimens of metastatic high-grade noninflammatory MMT. In 7 IMC cases (33%) and in 1 MMT case (5%), highly malignant neoplastic cells were found resembling endothelial cells forming structures similar to small capillaries. The higher frequency of this phenomenon in inflammatory versus noninflammatory canine mammary cancer is in agreement with previous studies of in vivo and in vitro experimental human IBC and spontaneous human IBC. 59-63 Therefore, the presence of VM has been reported in IBC mouse xenografts 59,60,62 but not in noninflammatory breast cancer mouse xenografts. 59,60,62 Similar results have been obtained within in vitro assays comparing IBC culture cells and noninflammatory breast cancer culture cells 62 where VM was present in only the former. The higher frequency of VM in IBC (15.8%) with respect to noninflammatory breast cancer (7.4%) has been confirmed using HE-stained paraffin sections of surgically excised human breast tumors. 63 Moreover, another study demonstrated that VM could be present in a primary noninflammatory breast cancer neoplasm and in the corresponding metastatic lymph node. 4 In agreement with these reports in human IBC, our findings indicate that VM is not specific for canine IMC, although it is much more frequent in this type of cancer, given that VM was present in a third of the IMC tumors and in only 1 case of the MMT (5%). Likewise, according to our results and previous studies in human IBC, 63 VM is not confined to one histological type of malignant mammary tumor, although in canine IMC it is more frequent in anaplastic carcinoma (38%). This fact suggests that VM could be not only related to the inflammatory phenotype but also to undifferentiated cellular attributes, given that anaplastic carcinoma is the most undifferentiated type of canine malignant mammary tumor (Misdorp et al., 1999).
The immunohistochemistry confirmed the epithelial and neoplastic origin of the ELCs; these cells were positive for epithelial markers (CK and CK 14) and for the same markers used for the rest of the tumor cells. A high percentage of ELCs were positive for vimentin, given that some were neoplastic cells in the same tumor. Coexpression of cytokeratin and vimentin in epithelial human mammary tumor cells has been related to a more aggressive phenotype and poor prognosis. 8,29,73,80 Regarding these studies, the coexpression of cytokeratin and vimentin of ELCs could be associated with their poor differentiation and agressive behaviour. In all cases, ELCs were negative for smooth muscle actin and desmin, meaning that myoepithelial cells are not the cell of origin of ELCs.
The immunostaining with specific endothelial markers, vWF, CD31, and CD34, was inconclusive, although it was considered mostly negative; some tumors presented some ELCs positive for WF with variable intensity. This result cannot be considered as a positive immunostaining for a specific endothelial marker, because in the same tumor, even in the normal mammary gland (data not shown), groups of normal and neoplastic mammary cells are usually stained by this antibody. The low specificity of this antibody against vWF has been indicated in human soft tissue tumors. 19 The antibody against vWF has been used in several studies of angiogenesis in human cancer; 2,67,75 but on the contrary, there are a limited number of studies in canine tumors where vWF has been used as an endothelial marker, 9,10,40,50,51,79 including canine mammary tumors. 23,24 Regarding the rest of the endothelial markers studied, some ELCs of a single case were slightly positive of CD31; in all samples, ELCs were negative of CD34.
The absence of a specific immunoreaction of ELCs with endothelial markers confirms the neoplastic origin of these cells and is in agreement with other authors' findings in human mammary tumors and other cancer types. Thus, it has been reported in human noninflammatory breast carcinomas 4 and in human ocular melanomas 42 that the tumor cells that developed the VM channels were negative of vWF. The anti-CD31 antibody has been employed to determine the tumor microvascularization in several types of human neoplasias; 7,14,45,46,67,75 however, there are limited studies in canine tumors, 40,41 including canine mammary tumors. 53 The immunostaining of the ELCs for CD31 was negative in 7 of 8 cases included in our study. Only in 1 case did a few ELCs show slight positive cytoplasmic reaction to CD31. This result is in agreement with previous similar studies in human intraocular melanoma, 42 human ICB xenograft, 62,63 human noninflammatory breast carcinoma, 4 Ewing sarcoma, 78 and hepatocellular carcinoma. 25 Finally, the ELCs were negative for CD34 in all of our cases. There are no previous studies of CD34 immunohistochemistry in canine tissues (including mammary tumors). The negative immunoexpression of ELCs for CD34 has been reported in human intraocular melanoma 42 and Ewing sarcoma. 78
The electron microscopy study revealed some important features that confirmed the epithelial nature of the ELCs and VM. Thus, ELCs lacked Weibel-Palade bodies (which are characteristic of endothelial cells 82 ) and presented desmosomes (the type of junction between epithelial cells) instead of the fascia occludens, which are endothelial cell-to-cell junctions. 83 Beside this, tumor and/or blood cells contained in the ELCs channels were not inside a vacuole, as in emperipolesis 55,56 or phagocytosis; 37 rather, they were inside a real internal space (channel) without secretions and limited by a cytoplasmic membrane. To our knowledge, there are no previous studies about the ultrastructure of ELCs. The presence of free blood cells in the central spaces formed in VM has been observed by electron microscopy in experimental IBC 59,62 and ocular melanoma. 42
The limited presence of red blood cells and the numerous white blood cells and neoplastic cells observed inside the VM channels seem to indicate that the VM channels found in our study are mimicking lymph vessels rather than blood vessels. This fact could be associated with the extremely high lymphangiogenic capacity and metastatic lymphangiotropism characteristics of IBC, 34,76,77 instead of a nutritional mechanism. The lymphatic VM has been proposed, 28 and it could be related to an attempt to develop an additional mechanism to spread the disease. Nowadays, the mechanisms that lead to cancer cells developing channels of VM are unknown. If a lymphatic VM in canine IMC is hypothesized, then a high expression of specific lymphangiogenic factors, such as VEGF-C (vascular endothelial growth factor-C) and VEGF-D (vascular endothelial growth factor-D) and their receptor VEGFR-3, should be expected to switch the neoplastic cells to the angiogenic phenotype. Further studies should confirm all these assumptions.
It is well known that human IMC 5,20,32,70 and canine IMC 31,47-49,54 exhibits special features and pathogenetic mechanisms. This study indicates that the presence of ELCs and VM is more frequent in canine IMC than in other, noninflammatory highly malignant mammary cancer types, as demonstrated in human IBC. 59,60,62,63 This fact is probably related to the special angiogenic and metastatic capacities of this type of cancer. 20,35,43,70 The confirmation of different angiogenic mechanisms in IMC (ie, VM) supports the idea of developing new, targeted antiangiogenic therapies for human and canine IMC.
Footnotes
Acknowledgements
We are grateful to Ana Vicente, Agustín Fernández, and Dr Maria Luisa García for their assistance processing the electron microscopy samples and to Pedro Aranda for his histotechnology assistance.
The authors declared that they had no conflicts of interests with respect to their authorship or the publication of this article.
The authors declared that they received financial support for their research. This research was supported by the Spanish Ministry of Science and Education (research project No. SAF 2005/03559 and PhD fellowship).