
Abstract
Introduction
Multilocus Inherited Neoplasia Allele Syndrome (MINAS) is a condition defined by the presence of germline pathogenic variants in more than one Cancer Susceptibility Gene (CSG). MINAS is still underreported in the literature and public databases. Since MINAS-related phenotypes are difficult to predict, case descriptions may contribute to risk assessment, treatment, and personalized surveillance for proband and relatives.
Case Description:
Here we report a unique case of early onset, bifocal, non-Triple Negative breast cancer in a 31-year-old woman. Fast metastatic dissemination involving the brain caused the death of the patient in a few months. Her multigene panel testing showed the co-occurrence of pathogenic variants in PALB2 (c.1221del; p.Thr408fs*40), ATM (c.8545C>T; p.Arg2849*), PMS2 (c.1919C>A; p.Ser640*), and MUTYH (c.1103G>A; p.Gly368Asp). The patient inherited the ATM and MUTYH variants from the mother, and PALB2 and PMS2 variants from the father. The brother inherited the maternal ATM and paternal PMS2 variants. A baseline imaging-based family screening excluded malignancies in both parents and in the brother. Tailored monitoring is ongoing based on the risk predicted by pathogenic variants identified in family members.
Conclusions:
Currently, there are no predictive tools available to determine organ-specific cancer risk in MINAS patients. Given the uncertainty in predicting the phenotypic effect of multiple variants in CSGs, ongoing clinical surveillance and sharing data from complex cases are crucial for improving risk stratification in this condition.
Introduction
Multilocus Inherited Neoplasia Allele Syndrome (MINAS) was first described in 2016 by Whitworth and colleagues to characterize the occurrence of germline pathogenic variants in more than one cancer-susceptibility gene (CSG) in a single patient. 1 This definition focuses on the pathogenicity of the variants and the number of genes involved. Most CSGs exhibit an autosomal dominant pattern of inheritance; therefore, in cases where CSGs are associated with autosomal recessive syndromes, both alleles must carry a pathogenic variant to meet the MINAS criteria. The database provided by Whitworth’s group (https://databases.lovd.nl/shared/diseases/04296) is a valuable tool for categorizing malignancy types and identifying CSG defects in individual cases, including only patients with likely pathogenic/pathogenic variants in two different CSGs. A recent comprehensive review reported 385 cases of MINAS, with 287 BRCA-related cases (74.5%) and 98 non-BRCA cases (25.5%), featuring a variety of CSG combinations. 2
The clinical phenotypes associated with MINAS are heterogeneous. Although they might be expected to reflect the sum of the clinical manifestations associated with each gene, 3 the possibility of a synergistic effect between pathogenic variants cannot be ruled out. 4 For example, in a series of 13 biallelic MINAS cases, 10 presented clinical manifestations associated with only one of the two mutations. 5 Family segregation studies can help clarify genotype-phenotype correlations and may inform clinical decisions regarding surveillance and prevention. However, when more than two pathogenic variants occur in non-BRCA CSGs, and the malignancy is typically associated with a BRCA-related phenotype, estimating the risk of a second malignancy in probands and developing a surveillance plan for healthy carriers can be challenging. To date, only one patient has been described carrying heterozygous pathogenic variants in three different CSGs (BRCA2-MLH1-NBN); this patient and family members had malignancies consistent with Lynch syndrome and Hereditary Breast and Ovarian Cancer syndrome spectrum. 6
We recently identified a non-BRCA MINAS case characterized by the co-occurrence of four germline pathogenic variants in CSGs in a young patient with non-triple negative breast cancer. Family segregation studies and somatic genetic testing raised several questions regarding the predisposing role of each variant and complicated the task of providing prognosis and surveillance information for her relatives.
Case Description
The proband, a 31-year-old Caucasian woman, was referred to our oncogenetic clinic due to early-onset breast cancer. She had been diagnosed the previous year with bicentric invasive ductal breast cancer (pT2pN0M0), G2, ER 40%, PgR 60%, Her2/neu 0, Ki67 25%, and was surgically treated with nipple-sparing mastectomy. Sentinel lymph node biopsy was negative, and she underwent chemotherapy with four three-weekly cycles of Epirubicin-Cyclophosphamide and Exemestane. Then she was addressed to our oncology clinic. However, fast metastatic dissemination involving the brain caused the death of the patient in a few months.
Both parents (father aged 60, mother aged 61) and her 28-year-old brother were cancer-free. The mother had undergone hystero-salpingo-oophorectomy at the age of 40, and five maternal uncles (ages 47, 49, 54, 57, and 58) and their offspring were all alive and cancer-free. The maternal grandfather died at 69 from gastric cancer, while the maternal grandmother, now 90, had a prior gynecological surgery and non-otherwise proven ‘chemotherapy’ (possibly for endometrial cancer; no medical records). On the paternal side, two uncles (ages 57 and 64) were living, with the former having had larynx cancer at 30. The paternal grandmother was alive and cancer-free at 89, while the paternal grandfather died of colorectal cancer at 85.
A prior BRCA1 and BRCA2 germline test conducted in another laboratory returned negative results. Somatic genetic testing revealed variants in ATM (p.Arg2849*), CTNNB1 (p.Gln773*), ERRFI1 (p.Lys116fs*7), MUTYH (p.Gly382Asp), PALB2 (p.Ser640*), PIK3CA (p.Cys901Phe, p.Arg93Trp, and p.Glu542Lys), PMS2 (p.Thr408fs*40), PTEN (p.Pro248fs*5; splice site 635-1G>A - subclonal), and TP53 (p.Arg248Gln). Additionally, rearrangements were detected in ARID1A and RB1, and equivocal amplification was reported in AURKA, GNAS, IGF1R, and ZNF217 genes.
At the request of the patient’s oncologist, a genetic re-evaluation was performed, expanding the test to non-BRCA risk genes. After genetic counseling and patient consent, an NGS multigene panel (Illumina TruSight Cancer) comprising 94 genes was analyzed. This test identified the following pathogenic variants in the heterozygous state: c.8545C>T (p.Arg2849*) in ATM; c.1103G>A (p.Gly368Asp) in MUTYH; c.1919C>A (p.Ser640*) in PALB2; and c.1221del (p.Thr408fs*40) in PMS2. These variants were interpreted according to the international 5-class IARC classification system and confirmed with Sanger sequencing, as per diagnostic genetic testing protocols. The panel did not include the eight genes that showed somatic variants (ARID1A, AURKA, CTNNB1, ERRFI1, GNAS, IGF1R, PIK3CA, and ZNF217); therefore, their germline status could not be assessed, though the somatic origin of PTEN and TP53 variants was confirmed.
During post-test counseling, the patient was informed of the genetic test results, which included germline heterozygous variants in ATM, PALB2, PMS2, and MUTYH. We provided an interpretation of both germline and somatic test data, particularly emphasizing the non-heritability of the PTEN and TP53 variants. Cascade genetic testing in the family revealed that PALB2 and PMS2 variants were of paternal origin, while ATM and MUTYH variants were inherited from the mother. The brother shared the ATM and PMS2 variants with the proband (Figure 1). Imaging-based screening excluded malignancies in the parents and the brother. They are currently followed up at the onsite Hereditary Cancer Clinic.
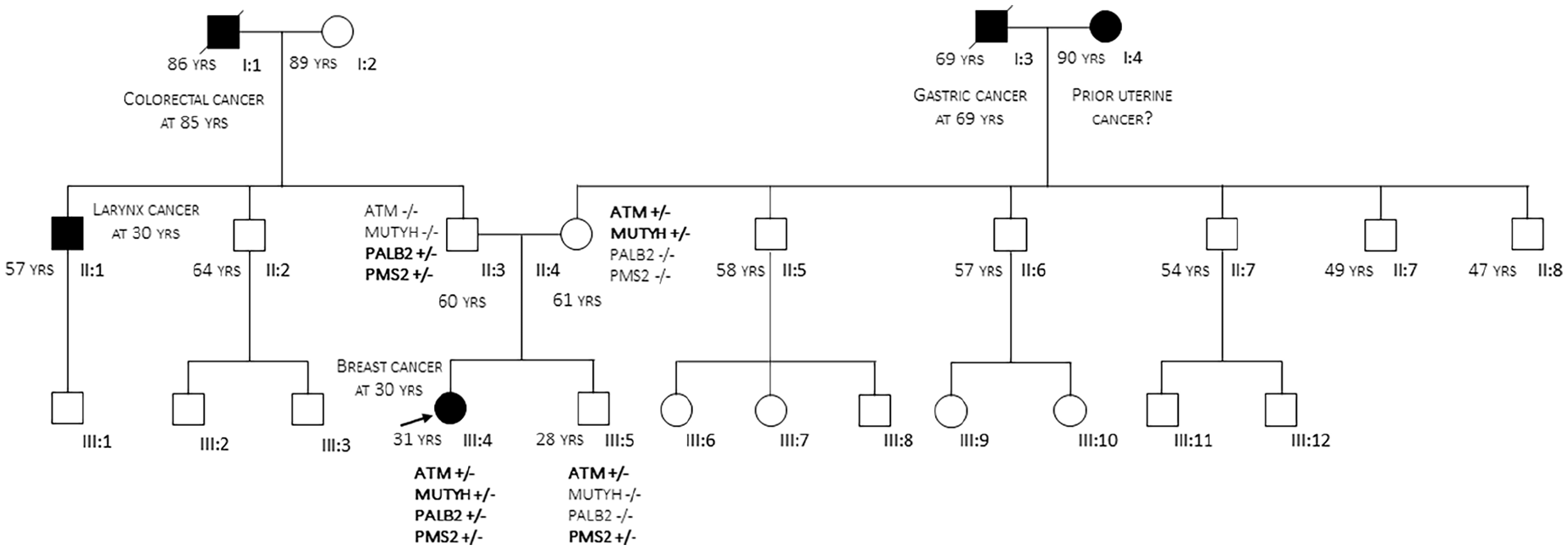
Pedigree of the family. The arrow points to the proband.
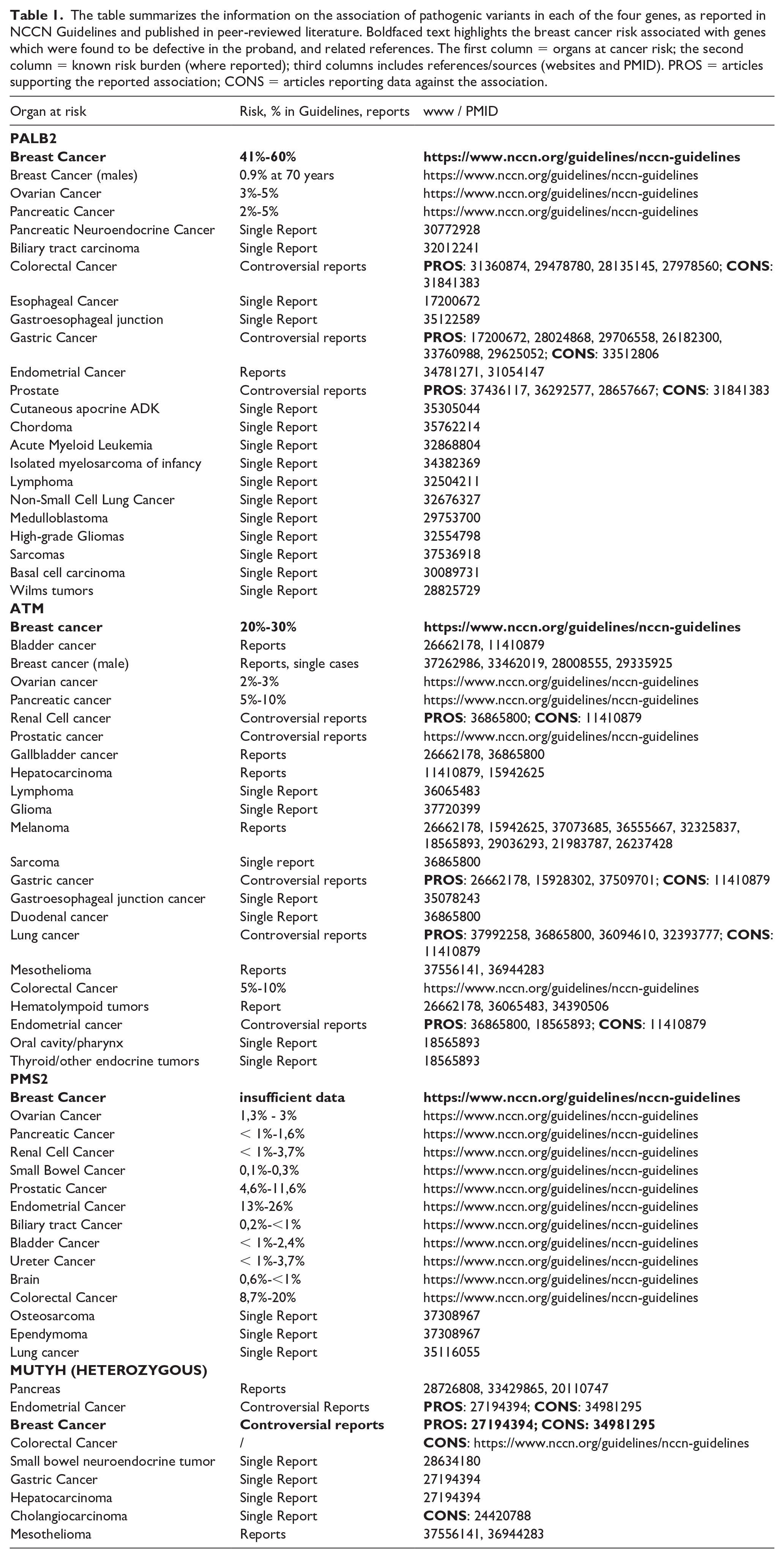
In addition, we provided information on the current understanding of MINAS, including associated risks and prevention strategies. To offer the most accurate information on the risks associated with each gene defect, we conducted two comprehensive reviews: one covering the cancer risks for each gene recognized by the scientific community (e.g., ClinGen and international guidelines like National Comprehensive Cancer Network - NCCN), and another review that included individual case reports of patients with pathogenic variants and malignancies in organs not typically linked to the corresponding cancer syndrome. The results are shown in Table 1 and were communicated to the patient.
The table summarizes the information on the association of pathogenic variants in each of the four genes, as reported in NCCN Guidelines and published in peer-reviewed literature. Boldfaced text highlights the breast cancer risk associated with genes which were found to be defective in the proband, and related references. The first column = organs at cancer risk; the second column = known risk burden (where reported); third columns includes references/sources (websites and PMID). PROS = articles supporting the reported association; CONS = articles reporting data against the association.
Conclusions
The presence of four heterozygous pathogenic variants in ATM, MUTYH, PALB2, and PMS2 supports a diagnosis of Multilocus Inherited Neoplasia Allele Syndrome (MINAS) as defined by Whitworth and colleagues. 1 While these findings did not influence the patient’s therapeutic regimen, they raised significant concerns regarding the risk of a second malignancy in the proband and the development of surveillance and prevention strategies for her relatives. The potential for these genetic defects to act additively, synergistically, or through more complex mechanisms in increasing cancer risk is an area of ongoing inquiry. In this complex estimation of the oncogenetic risk, there are at least four levels of evaluation: the number of defective genes, the pathways in which these genes operate, the cancer-predisposing genes, and their variants.
Most MINAS have been described in carriers of pathogenic variants in two different genes, more commonly BRCA1/2. The co-occurrence of three variants is far less common, 6 while four pathogenic variants are exceptional. The four variants observed in our proband affect three different pathways: the Homologous Recombination (HR) (the double heterozygosity ATM and PALB2) that repairs double-strand breaks in DNA; the Mismatch Repair (MMR) (PMS2) that is essential for correcting errors that occur during DNA synthesis; the Base Excision Repair (BER) (MUTYH) that repairs oxidative DNA damage. The spectrum of malignancies in MINAS with defects in HR and MMR genes includes female breast, endometrial, ovarian, and renal cell carcinomas (BRCA1 + MLH1) 7 ; female and male breast carcinoma (BRCA1 + MLH1) 8 ; endometrial cancer and Hereditary Breast and Ovarian Cancer Syndrome predisposition (BRCA1 + MSH6) 9 ; colorectal cancer, breast and endometrial cancer (MSH2 + BRCA2), with no apparent increased susceptibility to colorectal cancer in BRCA2 mutation carriers or to breast cancer in MSH2 mutation carriers. 10 In non-BRCA-MINAS with defects in MMR and BER pathways such as MSH6 and MUTYH, a higher incidence of urothelial cancers was found compared to MSH6 defect alone, suggesting that a single heterozygous MUTYH defect modifies the risk for developing urothelial cancers in MSH6 mutation carriers 11 .
At the gene and variant levels, the genetic defects observed in our proband may be associated with heterogeneous effects. The nonsense ATM p.Arg2849* leads to premature termination of the protein, which is predicted to undergo nonsense-mediated decay. This variant has been reported as associated with multiple malignancies (e.g. gastrointestinal and prostatic).12,13 The PALB2 p.Ser640* variant is well-known and predicts a premature protein truncation: for example, it has been associated with breast cancer in two young unrelated female patients and with prostatic cancer in the father of one of them.14,15 The PMS2 p.Thr408fs*40 variant predicts a frameshift defect that introduces a premature termination codon, leading to a truncated, likely non-functional protein; this variant has been associated with Turcot syndrome (Mismatch repair cancer syndrome 1) in compound heterozygosity. 16 The heterozygous MUTYH p.Gly368Asp missense variant has been reported in multiple cancer types, e.g. breast and colorectal cancer.17,18 Although the risk of malignancy in carriers of single gene defect seems to be higher than that of MINAS, we are not able to precisely estimate the risk nor to define whether the effect is a sum of the probabilities of developing tumors in the different organs due to an independent effect of the two or more genes, or whether there is a reciprocal or collective potentiation.
The impact of these observations concerns patients and families, in which segregation studies may help but not be sufficient to contribute to the definition of pathogenicity. In our family, each first-degree relative carried two pathogenic variants in genes acting in two different pathways; to date, none of them show oncological manifestations. We excluded a de novo origin of the germline variants, a possibility that was initially suspected, given that first-degree relatives were cancer-free. The mother’s oophorectomy may have prevented the manifestation of an ATM-related effect on her gynecological health: ATM, defects may increase the risk of ovarian cancer (with a 2-3% associated risk according to the NCCN 2.2024 guidelines).19,20 A similar ‘preventive’ effect could have occurred in the maternal grandmother, who underwent unspecified gynecological surgery; her carrier status is unknown, but she had a 50% chance of being the carrier of the variant. The potential role of the PMS2 variant in the paternal grandfather’s colorectal cancer remains unknown due to the non-feasibility of genetic testing, and similar considerations apply to gastric cancer reported in the paternal family. Based on the spectrum of reported cancer associations with single defects in heterozygous ATM, MUTYH, PALB2, or PMS2 (Table 1), no organ or tissue could be considered cancer risk-free in our proband and her first-degree relatives. The co-occurrence of these variants, coupled with the absence of tools to estimate overall risk, suggests the need for maintaining comprehensive clinical surveillance in first-degree relatives, including monitoring of at-risk organs in the PALB2- and PMS2-carrier father (HR and MMR pathways), the ATM- and MUTYH-carrier mother (HR and BER pathways), and the PALB2- and PMS2-carrier brother (HR and MMR pathways).
To our knowledge, there are no predictive tools or recommendations to establish organ-specific cancer risk in MINAS patients unless we sum gene-specific risk estimates. A recent report describing two additional MINAS cases highlights the challenging predictability of the phenotypic effect of harboring two (or more) variants in cancer-susceptibility genes. 21 Given this uncertainty, detailed information and clinical surveillance appear to offer the best protection. Sharing data from complex cases like the one we observed will contribute to advancing our understanding and improving risk stratification in MINAS, a condition that is likely to become more prevalent as NGS multigene panel testing continues to expand.
Footnotes
Author contributions
DB: Conceptualization, clinical data collection, writing original draft. EA: writing, critical revision and editing. MG and CG: genetic testing and text revision. MU: NGS data analysis and text revision. CC, AS, AF, GR: provided the oncological care to the patient and text revision.
Data Availability
The data reported in this article will be made available by the authors, without undue reservation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research on oncogenetics is supported by IRCCS Fondazione Policlinico San Matteo, grant 741-rcr2013-71.
Ethical approval
The local ethical committee has approved the oncogenetic work-up at the Fondazione IRCCS Policlinico San Matteo
(EUSOMA-certified).