
Abstract
Background:
Patients with cancer present a higher risk of vaccine-preventable diseases. Recommended vaccinations are the most cost-effective measure to reduce the risk of transmission and related complications. Nevertheless, vaccination rates are inadequate. Oncologists have a central role in tailored vaccine communication to their patients. We present the results of a survey conducted by AIOM in 2022, focusing on the perception of the problem by oncologists.
Materials and Methods:
An anonymous 31-item online questionnaire was shared on 15 September 2022 on the AIOM website. The objectives of this survey were to examine the perception of Italian oncologists on vaccine-preventable diseases and the main available vaccines, their attitude towards recommending vaccines and the COVID-19 pandemic impact on their habits regarding vaccine-preventable diseases.
Results:
Between September 2022 and January 2023, 114 medical oncologists (5% of the members) completed the anonymous questionnaire. At the first oncological visit, only 30% of respondents usually propose a vaccination schedule to all their patient, 41% do not usually discuss vaccinations at the first visit and 29% recommend vaccines exclusively to specific categories of patients. For 56% of respondents, patients are more aware of the benefits of vaccines, whereas 36% reported that patients are worried of receiving too many vaccines.
Conclusion:
This is the first survey conducted among Italian oncologists to better understand the perception and attitudes towards the vaccination. It highlights the urgent issues of educating and training oncologists in vaccine-preventable diseases and vaccine awareness and the need to build (or implement) a network of multidisciplinary collaborations.
Keywords
Introduction
Patients with solid tumors present a higher risk of vaccine-preventable diseases (VPDs). 1 The incidence of VPDs is higher among immunocompromised subjects compared to healthy subjects. VPDs represent an economic burden with increased all-cause healthcare costs and, most importantly for patients with cancer, causing delays in cancer treatment. 2 Recommended vaccinations are the most cost-effective measure to reduce the risk of transmission and related complications. Nevertheless, vaccination rates are inadequate. For instance, in Italy the seasonal flu vaccination coverage decreased from 65.3% in the 2020/2021 season to 58.1% in the 2021/2022 season, 87.8% received the first anti-SARS-CoV-2 booster dose, while only 38.1% received the second booster. 3 Vaccine hesitance is defined as ‘the reluctance or refusal to vaccinate despite the availability of vaccines’ and represents a significant threat to global health by the World Health Organization. 4 The Italian Association of Medical Oncology (AIOM) has been involved in promoting recommendations about COVID-19 vaccination since the beginning of the vaccination campaign. 5 It takes forward the mission of promoting vaccinations of major VPDs such as seasonal flu,6,7 pneumococcal disease7,8 and herpes zoster (HZ). 9 In brief, AIOM recommends seasonal flu and anti SARS-CoV-2 vaccination for every patient with solid tumors candidate to oncological active therapy, irrespective of the type of anticancer treatment (chemotherapy, ICIs, targeted therapy, hormonotherapy or a combination of these therapies), while pneumococcal vaccination is recommended to all the patients with lung and/or head and neck cancer. 7
Moreover, AIOM, together with the other scientific societies (the Italian Society of Infection and Tropical Diseases [SIMIT], the Italian Association of Clinical Microbiologists [AMCLI], the Italian Society of Hygiene, Preventive Medicine and Public Health [SITI]) will soon produce the first national guidelines on vaccinations for patients with cancer.
Oncologists have a central role in tailored vaccine communication with their patients; however, vaccination coverage rates are still far from optimal.
Here, we present the results of a survey conducted by AIOM in 2022, focusing on oncologists’ perceptions of the problem.
Materials and methods
Participants and period
An anonymous 31-item online questionnaire was shared on 15 September 2022 on the AIOM website (www.aiom.it) in a reserved section. It was accessible through a direct link that was sent by email to all regular AIOM members (n=2265). The link remained active until 15 January 2023. This study conforms to broad EQUATOR guidelines. 10
Study objectives
The objectives of this survey were to examine the perception of Italian oncologists about VDPs and the main available vaccines, their attitude towards recommending vaccines and the COVID-19 pandemic impact on their habits regarding VPDs.
Survey design
The survey was divided into three sections (See Online Supplementary Appendix 1). The first set of questions collected the demographic, training and employment details of respondents (Q1-Q9), the second one included general questions about attitudes toward vaccines for patients with cancer (Q10-Q19). The third part reported specific questions focused on the main vaccine-preventable diseases (Q20-Q31). Open and closed (multiple-choice, with either single or multiple permitted answers) questions were included.
Statistical analysis
Considering the descriptive nature of the study and the intention of inviting all the AIOM members, pre-planned sample size was not established. Data were analysed by descriptive statistics and they were presented as absolute numbers or percentages.
Results
Demographic, training and employment details of respondents (Q1-Q9)
Between September 2022 and January 2023, 114 medical oncologists (5% of the members) completed the anonymous questionnaire. Table 1 reports the demographics and working positions of the participants.
Demographic, training and employment details of respondents.
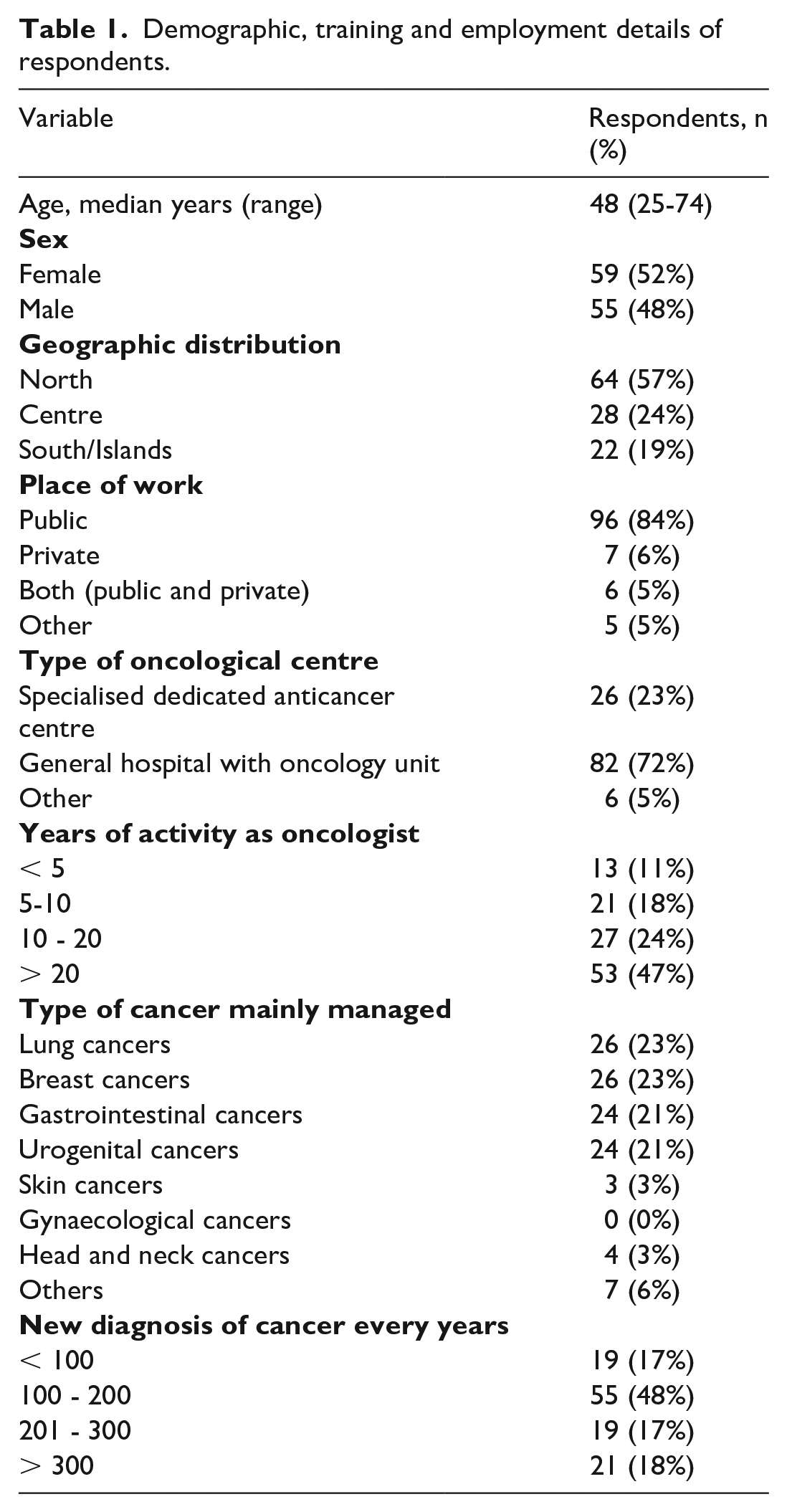
The median age was 48 years (range 25-74), and 52% (n=59) were female. The majority of respondents worked in Northern Italy (n=64, 57%), mainly in public general hospitals (n=96, 84%) with an oncology unit (n=82, 72%). Forty-six percent have worked in oncology for at least 20 years, including fellowship.
The main cancer type managed in their daily clinical practice was lung (n=26, 23%), breast (n=21, 23%), gastrointestinal (n=24, 21%), and genitourinary (n=24, 21%).
General attitudes toward the types of specific vaccines for cancer patients (Q10-Q19)
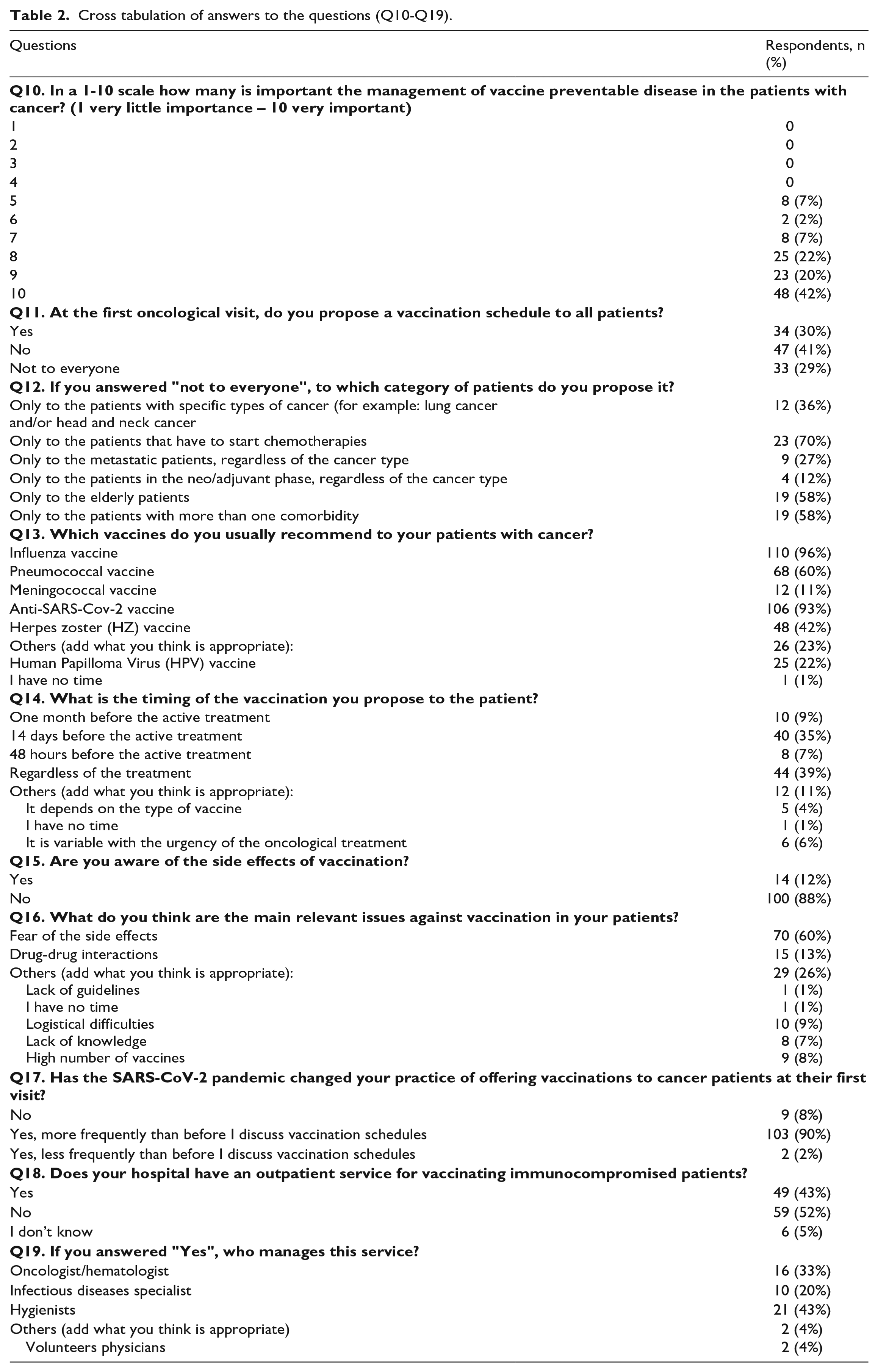
On a 1-10 scale 42% (n=48) consider the management of VPDs in patients with cancer very important and assigned a score of 10, 20% (n=20) assigned a score of 9, and 22% (n=25) assigned a score of 8 (1 very little important – 10 very important). No one assigned a score between 0 and 4. At the first oncological visit, only 30% of respondents (n=34) usually propose a vaccination schedule to all their patients, 41% (n=47) do not usually discuss vaccinations at the first visit and 29% (n=33) recommend vaccines exclusively to specific categories of patients. In particular, a vaccination schedule is proposed if patients are going to receive chemotherapy (70%) and if they have comorbidities (58%).
The seasonal flu vaccine is recommended by 96% of respondents, followed by an anti-SARS-CoV-2 vaccine (93%), pneumococcal (60%), and anti-HZ vaccines (42%). Meningococcal and human papilloma virus (HPV) vaccines are proposed by 22% and 11% of oncologists, respectively.
Concerning the most appropriate timing of the vaccination, the answers are highly variable: 39% of respondents (n=44) recommend vaccines regardless of the treatment, 35% (n=40) 14 days before starting oncological treatment, and 11% of respondents the timing of the vaccination proposal is difficult to determine and is generally made before treatment.
The majority of respondents (n=100, 88%) report that they are not worried about adverse events, but believe that the main issue against vaccination in cancer patients is the fear of side effects (n=70, 61%) or the drug-drug interactions (n=15, 13%). Question Q16 also provided the opportunity to specify their opinions on this topic.
Almost all respondents agreed that the COVID-19 pandemic has changed their habits, 'forcing' them to discuss vaccination schedules with patients (n=103, 90%). In the last part of this second section, the survey investigated whether there is an outpatient vaccination service for immunocompromised patients in their hospital. For 52% of respondents (n=59), such a service does not exist, 5% do not know, and 43%answered affirmatively. Where such service exists, in 43% of cases (n=21) it is managed by hygienists, in 33% of cases (n=16) by oncologists themselves, and in 20% (n=10) of cases by infectious disease specialists. In the remaining 4%, volunteer physicians provide the service.
A detailed description of the answers is reported in Table 2.
Cross tabulation of answers to the questions (Q10-Q19).
Specific questions focused on the main vaccine-preventable diseases (Q20-Q31)
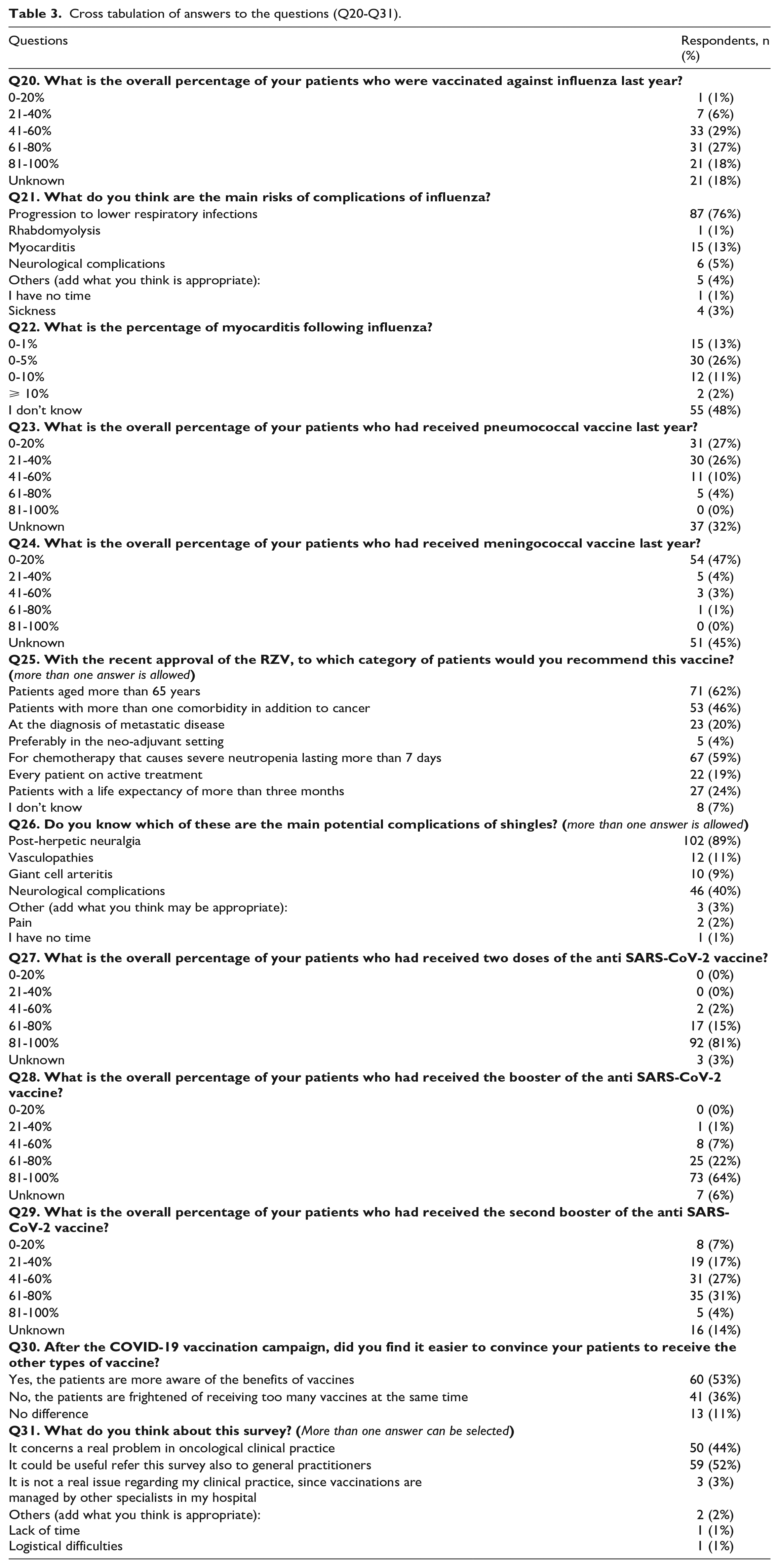
In this section, we interviewed oncologists about the main VPDs and their vaccines. The overall percentage of the patients who were vaccinated against the main VDPs as reported by the oncologist is reported in Figure 1. The progression to a lower respiratory infection is considered the main complication of influenza for 76% of respondents (n=87), followed by myocarditis and neurological complications. Forty-eight percent of respondents cannot quantify the risk of post-influenza myocarditis, while for 26% of physicians, it is between 0%-5%. With the recent approval of the recombinant herpes zoster vaccine (RZV), the majority of respondents believe it should be recommended for elderly patients (62%) and those who have to start a chemotherapy regimen at high risk for severe neutropenia/ lymphopenia (59%). Most of the respondents know that post-herpetic neuralgia is a complication of HZ (89%), but only 11% know that there can be post-HZ vasculopathy.
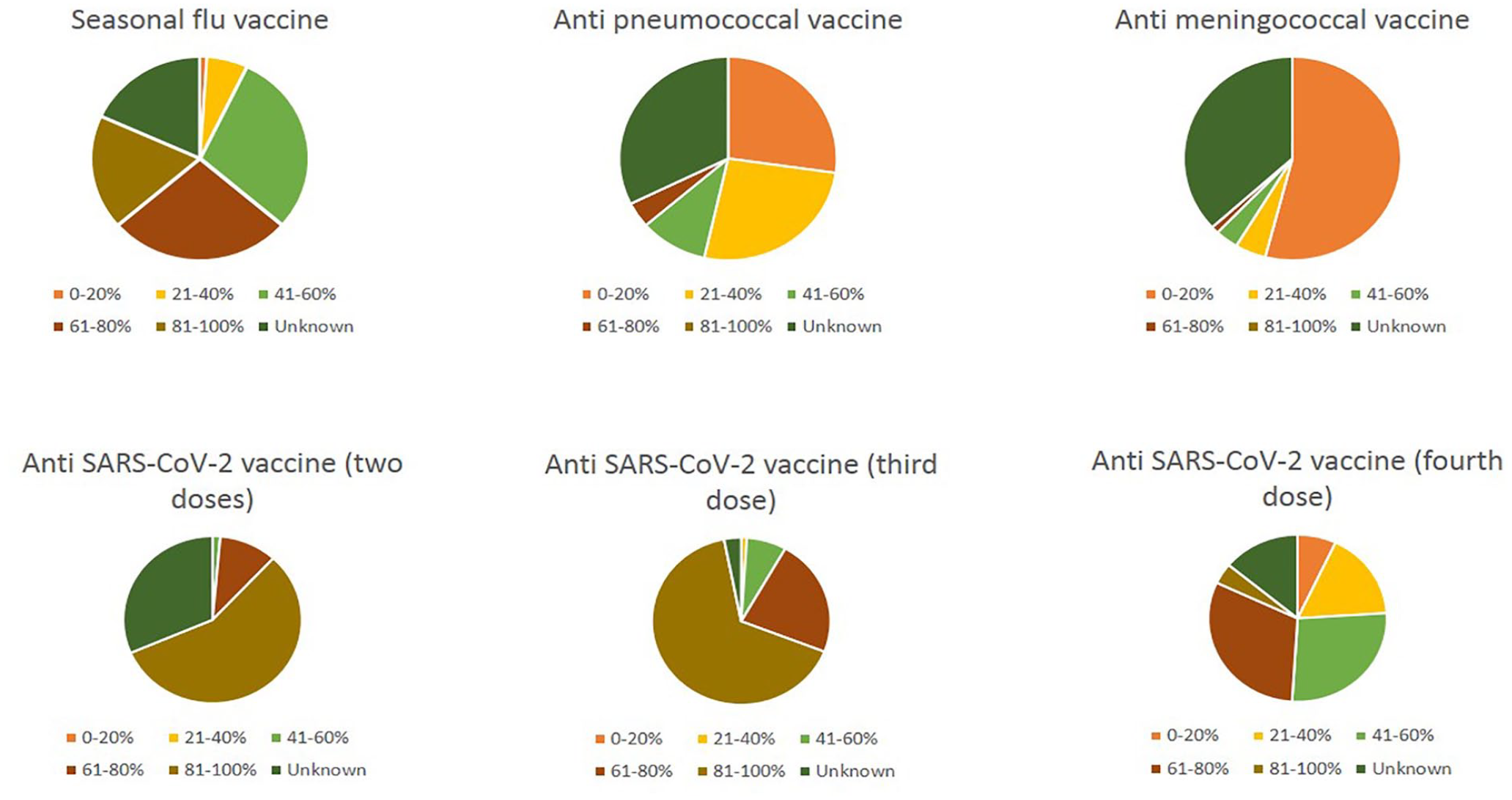
The overall estimated percentage of the patients who were vaccinated against the main vaccine-preventable diseases (VPDs).
Finally, we asked whether, after the COVID-19 vaccination campaign, it was easier to discuss the opportunity of receiving other types of vaccines with patients. For 56% of respondents, patients are more aware of the benefits of vaccines, whereas 36% reported that patients are worried about receiving too many vaccines, and 11% found no difference.
For 55% of respondents, it could be useful to address this survey also to general practitioners and 44% recognise that it concerns an actual issue in oncological clinical practice.
The complete answers are shown in Table 3.
Cross tabulation of answers to the questions (Q20-Q31).
Discussion
Oncologists have a key role in the education of patients about vaccination. Several models explain the various components of vaccination hesitancy. In 2015, the US National Vaccine Advisory Committee released a position paper that recommends the ‘development of an index, composed of a range of individual and societal dimensions, to measure trust in vaccines. This index should be able to (1) quickly, reliably, and validly monitor vaccine trust at the national level; (2) detect and identify variations in vaccine trust at the community level; and (3) diagnose key dimensions that influence vaccine trust’. 11 There is broad consensus that a valid and reliable measure to diagnose why people do not vaccinate will enable the design of interventions to increase vaccine uptake. Several models were considered to explain the various components of vaccination hesitancy, such as the '3C' model (confidence, complacency, and convenience), '7C' models (confidence, complacency, constraints, calculation, collective responsibility, and conspiracy), and the '5A' taxonomy of vaccination determinants (access, affordability, awareness, acceptance, and activation. 12 In a recent review, Welch and colleagues 13 have reported that trust in healthcare workers (HCWs) was considered the promoter of vaccine acceptance with the highest agreement rate (68.1%). Moreover, among the 80 papers included in this review, 64 recommended that improved education might increase the uptake of the influenza vaccine and that physicians have a central role. 13
On the other hand, patients tend to accept vaccines with less doubt if they are proposed and administered by oncologists themselves. 14
This survey serves some food for thought. First of all, only 5% of AIOM members completed the survey, despite several recalls during the time the survey was active. This very low percentage may reflect an attitude of neglect towards a topic of scarce oncological relevance rather than a lack of confidence in vaccines. Also relevant is the fact that few oncologist treating head and neck cancers (4%) responded to the survey, with those involved in lung and breast cancers being the most prevalent, despite patients with head and neck cancer having a high risk of VPDs. For example, Hansson and colleagues 15 found a positive association between oral and esophageal cancers and HZ (adjusted OR=1.41, 95% CI 1.11–1.79; and 1.41 95% CI 1.13–1.76), respectively. However, the proportion of respondents is not much lower than that observed for several other surveys launched by AIOM in recent years. 16 Of course, this low proportion of respondents emphasises the risk of bias in the results: probably those who replied to the survey are more sensitive to the topic. Consequently, the results could overestimate the attitudes and the awareness of Italian oncologists about vaccines in patients with cancer.
Another interesting result is the low percentage of respondents (30%) who discuss vaccinations with patients at their first oncological visit. If someone answered that they did not address this topic with all the categories of patients, but selected those at the highest risk (elderly or before chemotherapy), 41% reported that they did not talk about vaccines due to the lack of time, lack of knowledge of the topic or they felt it was not their responsibility (Q16,Q31).
McGinnis et al. 17 conducted a quality improvement study in their cancer centre in Hamilton, Ontario, to increase the number of patients with planned chemotherapy for gynecologic neoplasm receiving pneumococcal and influenza vaccinations. After the introduction of three simple interventions (an in-house vaccination programme, a staff education campaign, and a patient care bundle), they observed an increase in the vaccination rate. 17 The possibility of a close collaboration with other HCWs such as infectious disease specialists, hygienists or dedicated nurse practitioners could yield good results.
One relevant issue investigated concerns the best timing of the vaccination schedule. Guidelines suggest scheduling the vaccination before starting oncological therapies to avoid the phase of leucopenia.9,18 Recent studies conducted on different cancer populations and with different types of vaccines seem to indicate that the vaccine is effective regardless of the timing of administration.19,20 The majority of respondents seem to share this opinion, although they are aware that it is preferable to vaccinate before starting treatment.
The lack of time to discuss these issues with patients during the visits and the absence of an outpatient vaccination service in their hospital are matters of concern for most respondents. Local and regional realities differ greatly in the type of organisation and distribution of vaccination competencies. A network of multidisciplinary specialists is, therefore, increasingly necessary.
Another important topic is the fear of side effects or drug-drug interactions. Some case reports described immune-mediated vaccine-associated adverse events such as hepatitis, 21 but we have to consider that these immune-mediated mechanisms can also be caused by the viral infections themselves and that vaccines are indispensable to minimise these risks. 22
In the third part of the survey, we investigated which vaccines patients with cancer typically receive, as estimated by the oncologists. The full course of anti-SARS-CoV-2 and anti-seasonal flu are the most widely administered vaccines, while less than half of the patients received the pneumococcal or anti-meningococcal vaccine. Indeed, it is intriguing to notice that oncologists more often are aware of the anti-SARS-CoV-2 and seasonal flu vaccine uptake in their patients, and are less aware of the other vaccines uptake. This might reflect the relevance COVID-19 and influenza have had for the oncology community and the call for action for neglected VPDs which still have a high impact on patients with cancer.
The low number of respondents that may only be a partially representative sample of the Italian oncological reality is the main limitation of this survey. Yet, one may speculate that the time and willingness to fill in a quick questionnaire can be found if an issue is believed to be relevant. Therefore, a high rate of non-respondents might highlight a clear gap in the formation of oncologists. This low percentage of responders is in line with what has been observed in a survey conducted in 2016 by AIOM and the Italian Society of Artificial Nutrition and Metabolism (SINPE) on the issue of malnutrition. 23 The low response rate reflected the lack of awareness of this frequent problem in cancer patients among Italian oncologists but was the starting point for implementing intersociety initiatives, including the publication of position papers and specific guidelines24,25 capable of making the healthcare personnel more aware of this issue, allowing an increasing number of patients to receive adequate nutritional support.
To our knowledge, our paper reports the first survey conducted among Italian oncologists to better understand the perception and attitudes towards vaccination. Provided that vaccination holds significant benefits at an individual level, beyond a population and socio-economic level, and this is particularly true for cancer patients, this survey highlights the urgent issues of educating and training oncologists in VPDs and vaccine awareness and the need to build (or implement) a network of multidisciplinary collaborations between the various HCW and the general practitioners.
Supplemental Material
sj-pdf-1-tmj-10.1177_03008916231191547 – Supplemental material for Italian oncologists and vaccinations against infectious diseases: Results of a survey of the Italian Association of Medical Oncology
Supplemental material, sj-pdf-1-tmj-10.1177_03008916231191547 for Italian oncologists and vaccinations against infectious diseases: Results of a survey of the Italian Association of Medical Oncology by Angioletta Lasagna, Antonella Brunello, Nicola Silvestris, Paolo Pedrazzoli, Massimo Di Maio and Saverio Cinieri in Tumori Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.