
Abstract
This systematic review provides a summary of all studies published between 2000 and 2019 using a health-related quality of life (HRQOL) patient-completed questionnaire to report outcomes following diagnosis and treatment of thyroid cancer. The search terms were “thyroid cancer” or “thyroid carcinoma,” “quality of life” or “health related quality of life,” and “questionnaire” or “patient reported outcome.” EMBASE, PubMed, Medline, PsycINFO, CINAHL, and HaNDLE-On-QOL search engines were searched between 2 February and 23 February 2020. A total of 811 identified articles were reduced to 314 when duplicates were removed. After exclusion criteria (not thyroid specific, no quality of life questionnaires, and conference abstracts) were applied, 92 remained. Hand searching identified a further 2 articles. Of the 94 included, 16 had a surgical, 26 a primarily medical, and 52 a general focus. There were articles from 27 countries. A total of 49 articles were published from 2015 through 2019 inclusive. A total of 72 questionnaires were used among the articles and a range of 7 to 2215 participants were included within each article. This review demonstrated an increasing number of publications annually. The scope of enquiry into aspects of HRQOL following thyroid cancer is broad, with relatively few addressing surgical aspects and many focusing on the impact of radio-iodine. More research is required into shared decision-making in initial management decisions and HRQOL and interventions aimed specifically at addressing long-term HRQOL difficulties.
Introduction
The diagnosis of thyroid cancer (TC) is increasing globally1,2: in the United States, it accounts for 3.4% of all new cancers annually, 3 and through earlier diagnosis and improvement in treatments, 2 TC mortality is falling and the survivor population rising. TC diagnosis and management can have a detrimental impact on the health-related quality of life (HRQOL) of patients and their carers, not only during initial management but also in the long term, given that survival is increasing. The overdiagnosis of TC, particularly papillary TC, in the last 3 decades due to incidental findings on medical imaging or ultrasonography-based population screening has been described as a major global public health challenge. The potential repercussions of unnecessary treatment exposures and the impact on HRQOL are of great concern to clinicians globally, considering the relatively low morbidity of the clinical diagnosis.4 –6
TC prognosis is variable and depends on the combined effect of diagnostic stage, patient factors, such as age, and geographic variation in treatment protocols.4 –8 The HRQOL outcomes associated with surgery or medical treatment are varied and influenced by the consequence of cancer diagnosis, its treatment, and individual patient characteristics.9,10 The effect on functional, emotional, and social aspects of a patient’s life has previously been underappreciated, but with the more frequent use of patient-reported outcomes more data have emerged concerning HRQOL. This information aids improved treatment protocol, enhances care pathways, and drives new areas for intervention.
Published HRQOL outcomes focus on the effects of hormonal balance, surgery, radioiodine ablation (RIA), demographics, psychosomatic interventions, and behavioral help; the evidence base for these HRQOL concerns is growing with increasing numbers of studies published annually. However, there is a paucity of systematic reviews on HRQOL and TC. Husson et al. 9 reported 27 studies published from 1997 to 2010 and Bãrbuş et al. 11 reported 16 studies published from 2008 to 2016. As optimal treatment strategies and patient/carer support continue to evolve, the aim of this systematic review is to provide a summary of all studies published from 2000 to 2019 that have used HRQOL patient-completed questionnaires following TC. This time period was chosen as it includes the most up-to-date publications and captures the surge of quality of life (QOL) articles published in recent decades.
Methods
Search strategy
Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed in the reporting of this systematic review. 12 Six search engines were used: EMBASE, PubMed, Medline, PsycINFO, CINAHL, and HaNDLE-On-QOL. Searches were assisted by Leeds Teaching Hospitals NHS Trust and Liverpool University Hospitals NHS Foundation Trust between 2 February and 23 February 2020. To avoid missing relevant articles, one author (M.S.) hand searched the reference lists of a random 10% of articles.
The search terms used were “thyroid cancer,” “quality of life,” and “questionnaire”; however, these terms were expanded to achieve the most thorough results possible:
“thyroid cancer” or “thyroid carcinoma”
“quality of life” or “health-related quality of life”
“questionnaire” or “patient reported outcome”
No ethical approval was required to complete this review.
Study selection
We looked at TC articles between January 2000 and December 2019 inclusive involving humans of any age where full text was available in English, including those with nonvalidated, study-specific questionnaires. Studies where TC was part of a larger cancer cohort were included if the proportion of TC was at least 20% of the sample. Review articles, conference abstracts, and opinion articles were excluded. Qualitative research was included in this review. All forms of study design were included.
The research team included all the authors. Results of the literature search were downloaded into an Excel spreadsheet and screened by two independent reviewers (E.W., M.S.) who separately analyzed search results. Each article was categorized by year of publication, title, authors, cohort, design of study, theme and type of questionnaire, and then documented as included, excluded, or unable to decide from the abstract/title information, with inclusion disagreements resolved by the four remaining authors (A.K., S.N.R., J.W., D.K.).
Hand searching of a random 10% of articles (9) was completed by a single author (M.S.). Following the initial screening phase, full article consideration was undertaken by two independent reviewers (E.W., M.S.), and again escalated to the remaining four authors (A.K., S.N.R., J.W., D.K.) if inclusion disagreements occurred.
Data extraction and quality assessment
All authors were involved in data extraction from the selected articles, including recording the publication title, authors, cohort, design of study, theme, type of questionnaire, and summary of article conclusions and key findings.
Quality appraisal and assessment of risk of bias was performed on all included articles by a single author (E.W.). Quality appraisal was guided by the Joanna Briggs Institute critical appraisal checklists.13,14
Results
Following removal of duplicates, 314 articles were identified, of which 222 were excluded (99 not thyroid-specific, 28 no QOL questionnaires, 58 conference abstracts, 13 not written in English, 2 qualitative, 1 protocol, 12 benign thyroid lesions, 2 clinician-focused questionnaires, 2 literature reviews, and 5 could not be located). Hand-searching of articles identified two further eligible articles, resulting in 94 total articles. Figure 1 demonstrates the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart for this selection process.
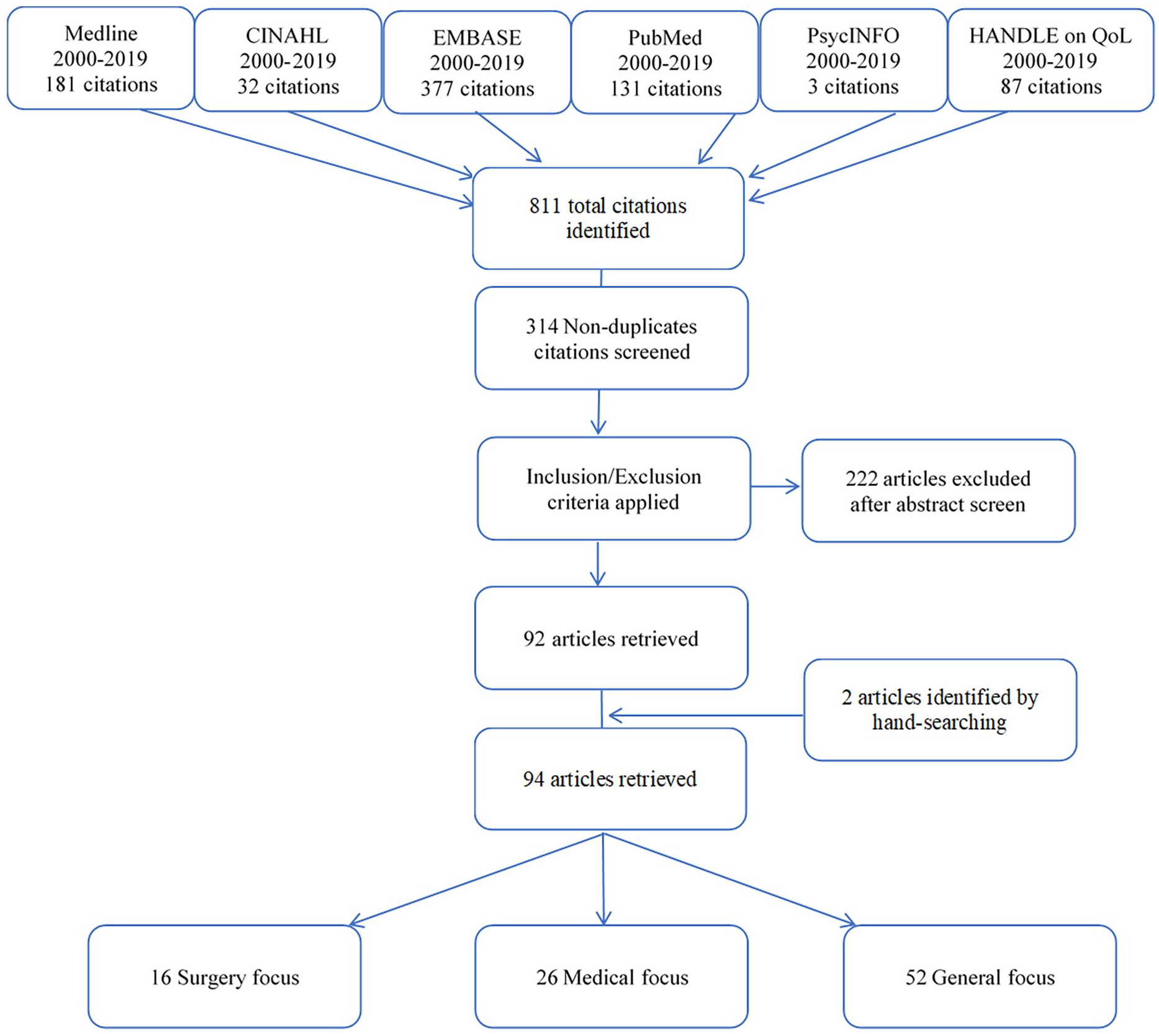
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart demonstrating the search and selection pathway for articles.
The articles were subcategorized into having a surgical (16), medical (26), or general (52) focus, which aided descriptive analysis and enabled development of key themes relating to HRQOL. Subcategorization was completed during the full article review phase and agreed between all authors. For articles to qualify as being in the surgical category, the primary focus of the article must have been on HRQOL following surgical management of TC. Those articles categorized as being medical were focused on endocrinologic and nuclear medicine treatments of TC. In comparison, the general category encompassed articles whose focus was on the impact of TC on HRQOL as a broader construct, including functional, emotional, social, and existential considerations such as self-esteem and purpose.
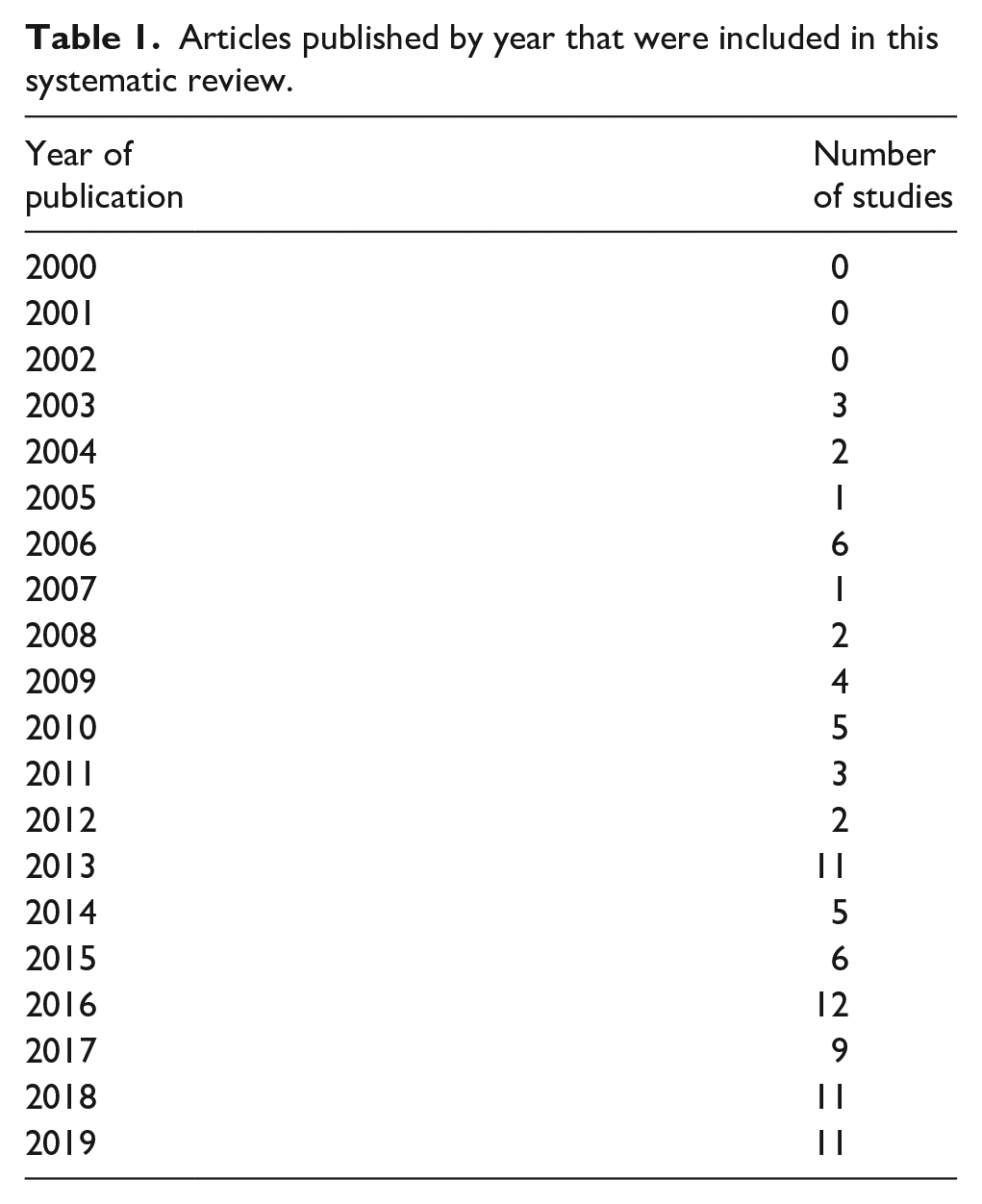
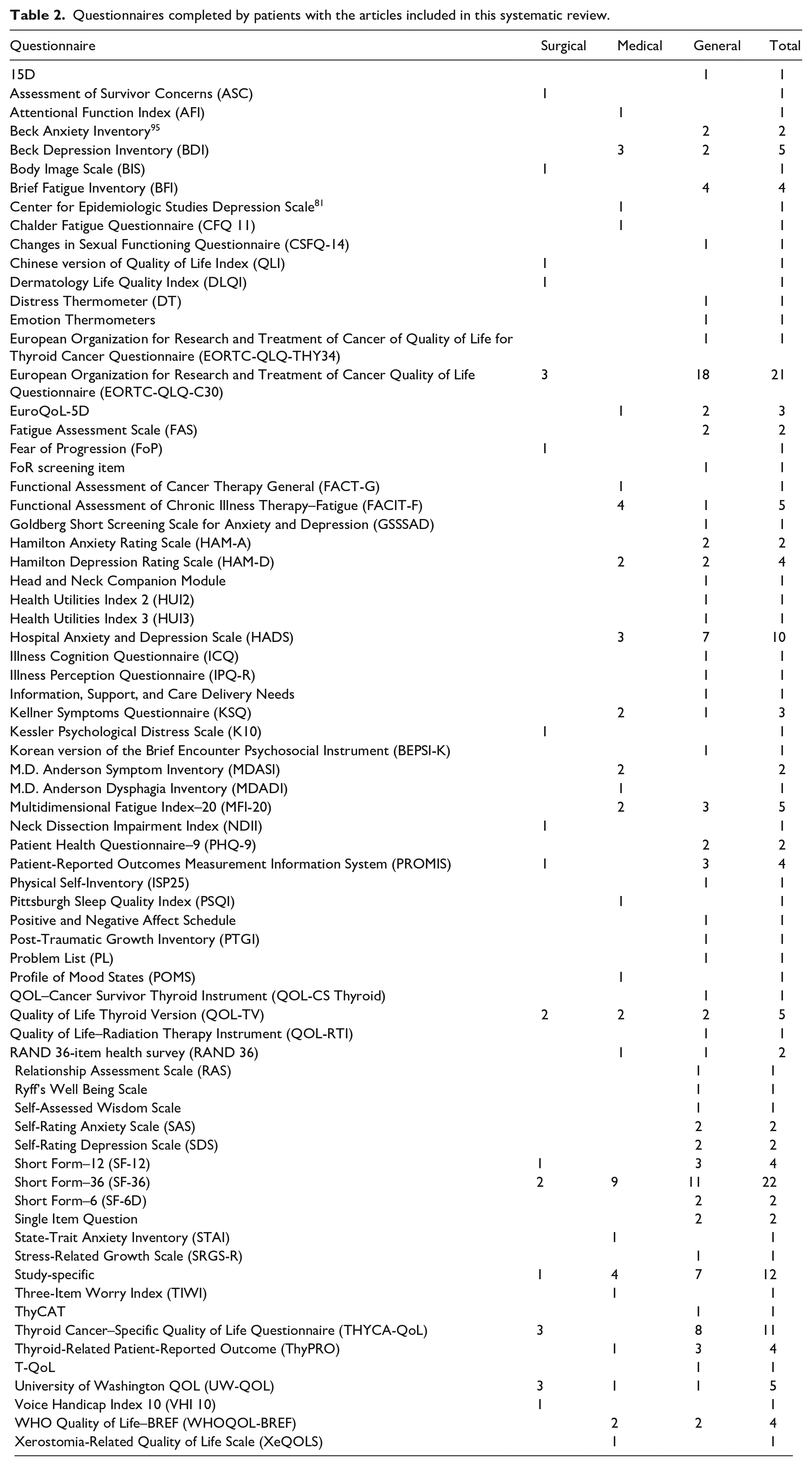
The number of articles published annually shows a general trend towards increased volume with time (Table 1). A large variety of validated and nonvalidated patient-reported questionnaires (including study-specific) were utilized (total 72, range of 1–8 per article) (Table 2). The most commonly used was the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC-QLQ-C30), followed by Short Form–36 (SF-36). Articles were published from 27 countries (Table 3), with no clear geographic pattern, although Korea had more surgical articles (7 of 11) and the Netherlands a tendency to general HRQOL (9 of 12).
Articles published by year that were included in this systematic review.
Questionnaires completed by patients with the articles included in this systematic review.
Articles published by country included in systematic review.

The number of participants included within these studies varied significantly, between 7 15 and 2215. 16 Study design was variable, but the majority of studies were cross-sectional in nature (78 of 94 [83%]).
The majority of articles focused on the HRQOL of participants with differentiated TC. A total of 12 articles did not specify histologic diagnosis of TC for included participants, and only 14 included medullary TC. Further presentation of the results have been divided into the three subcategories and are presented narratively in Tables 4, 5, and 6.
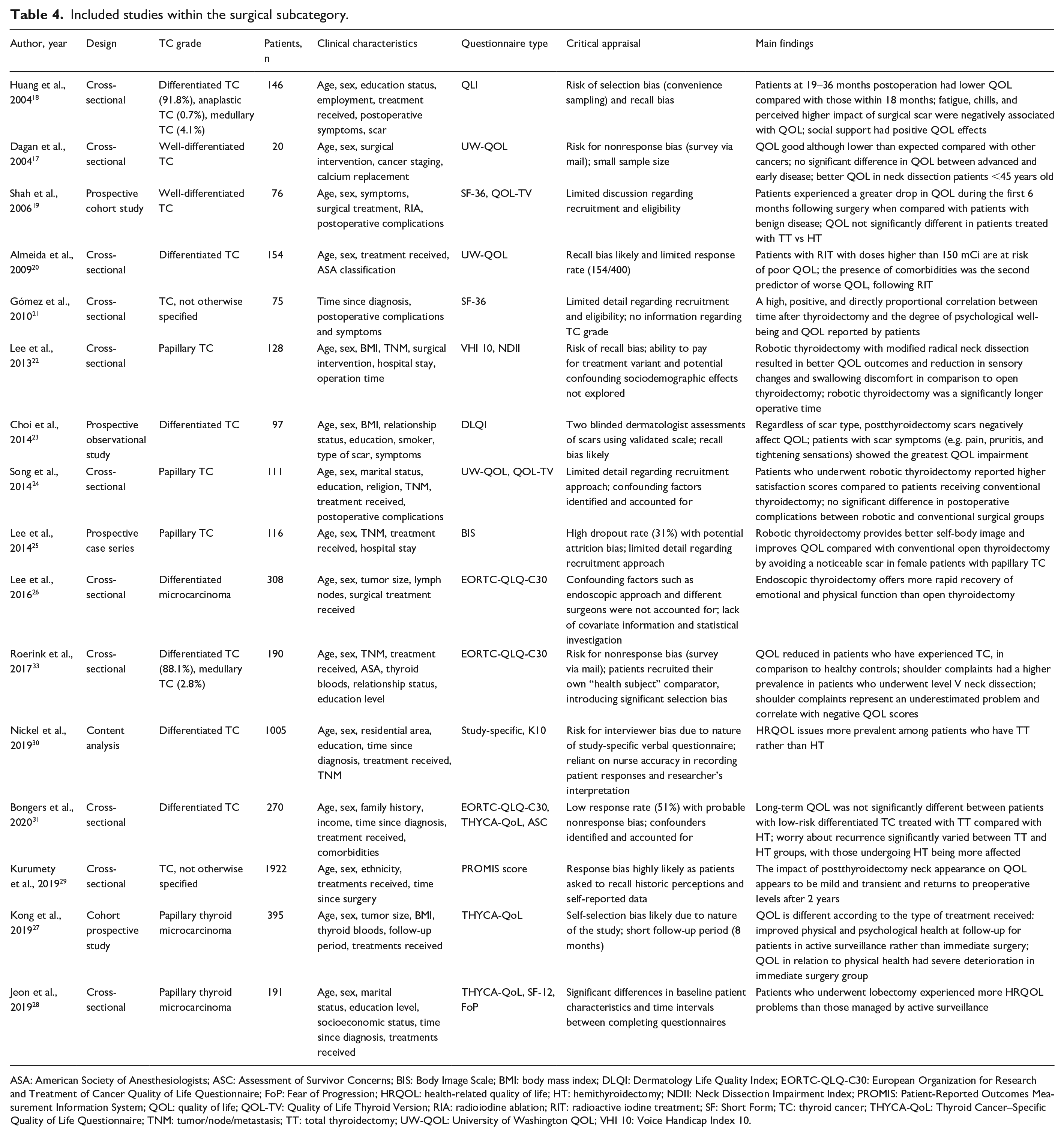
Included studies within the surgical subcategory.
ASA: American Society of Anesthesiologists; ASC: Assessment of Survivor Concerns; BIS: Body Image Scale; BMI: body mass index; DLQI: Dermatology Life Quality Index; EORTC-QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; FoP: Fear of Progression; HRQOL: health-related quality of life; HT: hemithyroidectomy; NDII: Neck Dissection Impairment Index; PROMIS: Patient-Reported Outcomes Measurement Information System; QOL: quality of life; QOL-TV: Quality of Life Thyroid Version; RIA: radioiodine ablation; RIT: radioactive iodine treatment; SF: Short Form; TC: thyroid cancer; THYCA-QoL: Thyroid Cancer–Specific Quality of Life Questionnaire; TNM: tumor/node/metastasis; TT: total thyroidectomy; UW-QOL: University of Washington QOL; VHI 10: Voice Handicap Index 10.
Included studies within the medical subcategory.
AFI: Attentional Function Index; AJCC: American Joint Committee on Cancer; BDI: Beck Depression Inventory; BMI: body mass index; CES-D: Center for Epidemiological Studies-Depression; DTC: differentiated thyroid cancer; EU: euthyroid; FACIT: Functional Assessment of Chronic Illness Therapy; FACIT-F: Functional Assessment of Chronic Illness Therapy–Fatigue; FACT-G: Functional Assessment of Cancer Therapy–General; HADS: Hospital Anxiety and Depression Scale; HAM-D: Hamilton Depression Rating Scale; HRQOL: health-related quality of life; KSQ: Kellner Symptoms Questionnaire; MDADI: M.D. Anderson Dysphagia Inventory; MDASI: M.D. Anderson Symptom Inventory; MDASI-THY: M.D. Anderson Symptom Inventory–thyroid cancer module; MFI-20: Multidimensional Fatigue Index–20; POMS: Profile of Mood States; PSQI: Pittsburgh Sleep Quality Index; QOL: quality of life; QOL-TV: Quality of Life Thyroid Version; RAI: radioactive iodine; RAND-36: RAND 36-item health survey; rhTSH: recombinant human thyroid-stimulating hormone; RIT: radioactive iodine treatment; RRA: radioiodine remnant ablation; rTSH: recombinant thyroid-stimulating hormone; SCH: subclinical hypothyroidism; SF: Short Form; STAI: State-Trait Anxiety Inventory; TC: thyroid cancer; THW: thyroid hormone withdrawal; ThyPRO: Thyroid-Related Patient-Reported Outcome; TIWI: Three-Item Worry Index; TNM: tumor/node/metastasis; TSH: thyroid-stimulating hormone; UICC: Union for International Cancer Control; UW-QOL: University of Washington QOL; XeQOLS: Xerostomia-Related Quality of Life Scale.
Included studies within the general subcategory.
ATA: American Thyroid Association; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; BEPSI-K: Korean version of the Brief Encounter Psychosocial Instrument; BFI: Brief Fatigue Inventory; BMI: body mass index; CSFQ-14: Changes in Sexual Functioning Questionnaire; DT: Distress Thermometer; DTC: differentiated thyroid cancer; EORTC-QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; EORTC-QLQ-THY34: European Organization for Research and Treatment of Cancer of Quality of Life for Thyroid Cancer Questionnaire; FACIT: Functional Assessment of Chronic Illness Therapy; FAS: Fatigue Assessment Scale; FC: functional connectivity; GSSSAD: Goldberg Short Screening Scale for Anxiety and Depression; H+N: Head and Neck; HADS: Hospital Anxiety and Depression Scale; HADS-A: Hospital Anxiety and Depression Scale–Anxiety; HADS-D: Hospital Anxiety and Depression Scale–Depression; HAM-A: Hamilton Anxiety Rating Scale; HAM-D: Hamilton Depression Rating Scale; HRQOL: health-related quality of life; HUI2: Health Utilities Index 2; HUI3: Health Utilities Index 3; ICQ: Illness Cognition Questionnaire; IPQ-R: Illness Perception Questionnaire; ISP25: Physical Self-Inventory; KSQ: Kellner Symptoms Questionnaire; KT-QoL: Korean version of the self-reported thyroid-specific quality of life questionnaire for thyroid cancer patients; MBMI: modified body mass index; MFI-20: Multidimensional Fatigue Index–20; PHQ-9: Patient Health Questionnaire–9; PL: Problem List; PROMIS: Patient-Reported Outcomes Measurement Information System; PTGI: Post-Traumatic Growth Inventory; QOL: quality of life; QOL-CS: QOL–Cancer Survivor; QOL-RTI: Quality of Life–Radiation Therapy Instrument; QOL-TV: Quality of Life Thyroid Version; RAI: radioactive iodine; RAS: Relationship Assessment Scale; RIA: radioiodine ablation; SAS: Self-Rating Anxiety Scale; SDS: Self-Rating Depression Scale; SF: Short Form; SRGS-R: Stress-Related Growth Scale; TC: thyroid cancer; THYCA-QoL: Thyroid Cancer–Specific Quality of Life Questionnaire; ThyPRO: Thyroid-Related Patient-Reported Outcome; TNM: tumor/node/metastasis; UW-QOL: University of Washington QOL.
Surgical
Sixteen articles had a surgical emphasis (Table 4). The most frequently utilized questionnaires were EORTC-QLQ-C30 (3), Thyroid Cancer–Specific Quality of Life Questionnaire (THYCA-QoL) (3), and University of Washington QOL (UW-QOL) (3). HRQOL issues focused around the following themes, in order of decreasing frequency:
Robotic and endoscopic surgical approaches (versus conventional technique)
Surveillance vs surgical management
Total thyroidectomy (TT) vs hemithyroidectomy (HT)
Other
Robotic and endoscopic surgical approaches
Up to 2013, five studies explored the effects of thyroid surgery on HRQOL. These varied in scope with no consistent findings. They reported lower HRQOL in TC than other cancers 17 and negative scar perception 18 was associated with long-term reduced HRQOL. However, there was no clear relationship between HRQOL and the extent of surgery.17 –21 Since 2013, there have been increased publication rates exploring thyroid surgery and HRQOL, mainly driven by the advent of novel endoscopic and robotic-assisted techniques aimed at minimizing surgical scars. Seven studies from Korea (where remote-access techniques have been most rapidly adopted) demonstrate the importance of scarring after thyroidectomy and the HRQOL conferred by its reduced visibility with minimally invasive procedures.22 –28 Conversely, a US study found scar visibility to have only mild negative HRQOL influence, returning to normal after 2 years. 29
Song et al. 24 found that patients were more satisfied with their scar after robotic surgery, although no significant difference in overall HRQOL was found between robotic and conventional surgical approaches to papillary TC resection. They observed that despite surgical approach, the most important issues relating to ultimate HRQOL scores were baseline anxiety and humor. Reduced paresthesia to the neck (i.e. reduced hyperesthesia or paresthesia), better swallow function, and scar satisfaction resulted in better HRQOL following endoscopic/robotic thyroidectomy and neck dissection in patients with metastatic TC, in comparison to open approach. 22 The duration of surveillance, differences in patient groups, and bias of preselection due to patient preference into comparative groups are highlighted by all the studies to likely influence the study findings. Prospective randomized trials are needed to resolve these issues.
Surveillance vs surgical management
More recent studies exploring thyroid surgery impact on HRQOL have been driven by changes in practice and international guidelines in the management of low-risk TC.4 –7 Until 2015, almost all patients with TC underwent thyroidectomy. Those with macroscopic disease (>1 cm) were managed with TT and RIA. However, recent guidelines 7 have moved clinical practice towards offering patients with microcarcinoma surveillance only, and for those with small cancers (without high-risk features), HT. Two articles compared HRQOL in patients diagnosed with microcarcinoma offered surveillance versus thyroidectomy. Kong et al. 27 reported lower psychological and overall HRQOL after surgery. The study is significantly limited by a much smaller surgical cohort and higher proportion of females within the operated group and a short follow-up period (8 months median). Jeon et al. 28 reported lower HRQOL in the surgical group compared to the surveillance group. They observed that level of diagnosis-related anxiety and fear of recurrence were similar for both groups. The median follow-up was 6–7 months and there was clear selection bias into the comparative cohorts.
Total thyroidectomy vs hemithyroidectomy
Two studies compared HRQOL in patients undergoing HT versus TT. Nickel et al. 30 reported more prevalent HRQOL issues after TT whereas Bongers et al. 31 did not observe differences in the long term. Nickel et al. 30 reported only short-term follow-up, with a median <6 months in 60% of 1005 patients. Physical complaints were frequent, with fatigue and inconvenience of taking thyroxine being most common. However, the effects of RIA, which is used only after TT, may be responsible, and there were no data on adequacy of thyroxine replacement. The study design did not allow comparison of the relative impact of the psychological issues related to emotional distress of diagnosis and fear of recurrence. Bongers et al. 31 reported a long-term follow-up study of 529 patients 31 and no significant differences in HRQOL between HT and TT were observed. Their findings are supported by Shah et al., 19 who reported comparable HRQOL in the short term (12 months) regardless of surgical extent. However, HT was associated with higher levels of recurrence anxiety. It is well known that worry about recurrence continues long-term and significantly affects HRQOL.16,32 The importance of the relationship between surgery extent and recurrence concern should be explored further.
Other
The negative HRQOL repercussions of neck dissection was highlighted, in particular shoulder complaints, loss of neck sensation, swallowing discomfort, and reduced chewing ability.17,20,22,33 Almeida et al. 20 found patients who had level II to VI neck dissections to have significantly worse chewing and shoulder scores relative to QOL, in comparison to those who underwent level VI alone. Lee et al. 22 reported the potential benefit from robotic surgery in patients undergoing neck dissection. They report better swallow function, less paresthesia of skin, and improved scar satisfaction.
The surgical risk of hypoparathyroidism following central compartment lymphadenectomy was acknowledged by numerous articles. The prevalence of permanent hypoparathyroidism varied significantly (0–18.5%),19,22 but no study reported any specific HRQOL changes due to this altered hormonal state.
Medical
The 26 medically focused articles are summarized in Table 5. The most common questionnaire was SF-36 (9). The main HRQOL aspects pertained to the following themes in decreasing frequency:
Thyroid hormone withdrawal (THW) prior to radioiodine therapy or imaging
Chronic subclinical hyperthyroidism (thyroid-stimulating hormone [TSH] suppression)
RIA therapy
Therapies for advanced disease
Other
Thyroid hormone withdrawal
A significant decrease in HRQOL following the onset of hypothyroid symptoms after THW in preparation for therapy or imaging was frequently reported.10,34 –45 The cross-sectional study by Tagay et al. 40 demonstrated overall anxiety and depression prevalence of 63% and 17%, respectively, in patients undergoing THW. Rubic et al. 10 found significant negative determinants of HRQOL at the time of diagnosis: fear of metastases, family distress, and the need for surgery/RIA. Females had significantly more concerns. Tan et al. 45 found patients of a lower education level and increased age had the most significant HRQOL decrease. Interestingly, they did not find a negative HRQOL impact (as measured by SF-36) for those patients who had ceased thyroxine in the preceding 6 weeks, despite the expectation that it would. Recommencement of thyroid hormone supplementation was shown to improve HRQOL (particularly fatigue) within patients who had experienced a 6-week hypothyroid state following THW. 44
The relatively positive HRQOL of those patients who were provided with recombinant TSH (rTSH) as opposed to THW was reported.34,37,39,43,46 –50 These positive HRQOL implications further support recent changes to clinical guidance, advising routine use of rTSH prior to imaging or RIA.
Chronic subclinical hyperthyroidism (TSH suppression)
The impact of chronic TSH suppression on HRQOL was explored.41,42,51 –54 HRQOL was negatively affected by TSH suppression when compared with euthyroid reference groups with no history of thyroid disease.41,42,51 –54 Jung et al. 42 found women receiving thyroxine following thyroidectomy were at increased risk for attention and memory problems, and those with TC had greater reported fatigue and sleep problems. However, a blinded randomized control study in which L-thyroxine was titrated to continue TSH suppression or establish euthyroidism demonstrated no HRQOL benefit to restoring euthyroidism. 52 These findings were reinforced by Massolt et al., 54 who found no improvement in HRQOL relating to fatigue and well-being with increased L-thyroxine dosages. Vigário et al. 41 found a supervised exercise program improved relatively low HRQOL of TSH-suppressed patients.
RIA therapy
The potential toxicities of RIA were highlighted, as the increased risk of sialadenitis and reduced swallowing capability negatively affected HRQOL. 55 Despite >50% of patients having anxiety and concerns prior to RIA, Barbus et al. 56 found most patients would undergo further courses if indicated, suggesting treatment burden has a relatively low HRQOL effect. This was supported by Taïeb et al., 50 who reported RIA to have no significant effect on HRQOL in the medium term (9 months). They did find younger age, sex (male), and higher pre-RIA HRQOL scores to have significant positive effects on ultimate HRQOL.
Therapies for advanced disease
A small number of studies investigated the effect of drug treatments on the HRQOL of patients with advanced TC. The utilization of axitinib in patients with iodine refractory differentiated TC was shown to maintain HRQOL as well as improve progression-free survival. 57 There was a notable absence of HRQOL data relating to licensed treatments for advanced disease, such as Sorafenib and Lenvatinib.
Other
Medullary TC-related diarrhea reduces HRQOL in relation to fatigue, disturbed sleep, distress, and sadness; the use of calcium aluminosilicate antidiarrheal improved HRQOL. 15
General
Fifty-two articles had a general focus (Table 6). EORTC-QLQ-C30 was the most frequently used questionnaire (n=18), followed by SF-36 (n=11). This category was broken down into the following categories in decreasing frequency:
HRQOL with and without comparison to normative data
Development of questionnaires and translations
Lifelong distress within at-risk groups
Other
HRQOL with and without comparison to normative data
The majority of articles found HRQOL to be good when compared to normative data. Most were published since 2013, and focused on anxiety, depression, fatigue, and recurrence concerns. Prior to 2013, four articles found HRQOL to normalize following a short-lived drop after diagnosis and treatment.39,58 –60 Lee et al. 61 and Singer et al. 62 both found HRQOL to be lower than comparative populations and anxiety, depression, and levels of fatigue significantly impacted this. Following 2013, a large number of articles revealed specific areas that impacted a survivor’s HRQOL. Fatigue,63 –66 concentration ability,63,67 pain, 68 swallowing difficulties, 68 anxiety, 67 depression, 66 comorbidity,65,67 increased age,69,70 decreased age, 71 sex,69,72,73 lower education status, 69 financial distress, 74 RIA requirement, 75 and fear of recurrence 32 significantly reduced HRQOL. TC survivors highlighted having their cancer referred to as the “good kind” trivialized their diagnosis and decreased HRQOL as they felt unsupported by physicians and family. 76 Wu et al. 77 found a 12-month psychological support program resulted in higher HRQOL compared to those who did not receive such support, although their sample size was small (60) and participant selection bias likely. Büel-Drab et al. 78 found TC to have very small impacts on patient–partner relationships and intimacy.
There is an equally large evidence base reporting good HRQOL that does not compare to reference populations. Roberts et al. 79 found high HRQOL and any patient-reported information needs were covered within routine follow-ups. However, multiple authors reported factors that reduced HRQOL, including the number of RIA treatments required, 80 treatment side effects, 81 fear of recurrence,16,82 employment status, 82 sudden tiredness,82,83 age, 84 nausea and vomiting, 84 and lower education level. 16 Surprisingly, HRQOL was not significantly impacted when patients experienced voice problems, despite the expectation that recurrent laryngeal nerve damage following thyroidectomy would result in decreased HRQOL. 84
Development of questionnaires and translations
Six articles focused on developing and translating questionnaires.85 –90 THYCA-QoL was developed 86 and recommended for use in combination with EORTC-QLQ-C30. Jeong et al. 87 published their validation of THYCA-QoL for use in the Korean language, after determining strong Cronbach α coefficient scores in the majority of multi-items. The third phase of developing an EORTC QOL module for TC (EORTC-QLQ-THY34) was published. 89 The EORTC-QLQ-C30 was further analyzed by Bernardo et al., 88 who found acceptable validity and internal consistent reliability with Filipino adults with differentiated TC. Watt et al. 85 found ThyPRO to have good clinical validity and reliability in a variety of thyroid diseases. Ryu et al. 90 found KT-QoL to be valid in evaluating QOL in Korean patients with TC.
Lifelong distress within high-risk groups
Three articles identified lifelong distress in groups considered to be at high risk of distress, as determined by the authors of this systematic review. Roerink et al. 91 found lower education levels correlated with worse HRQOL scores. Two articles looked at long-term HRQOL of young patients treated for TC and found generally comparable scores with normative data.92,93 Metallo et al. 93 identified female survivors diagnosed <25 years old, and found no difference in HRQOL compared to the reference population. Pregnancy outcomes following historic I131 treatment and miscarriage rates were comparative and no birth defects observed. Nies et al. 92 included participants diagnosed <18 years old and found no significant HRQOL differences compared to controls.
Other
Two articles focused on areas not covered by the previous subcategories.94,95 Employment and insurance factors were explored and found 62% of survivors struggled to obtain life insurance and increased age, level of fatigue, and lower educational obtainment were associated with unemployment. Employed TC survivors had improved HRQOL compared to unemployed survivors. 94 Liu et al. 95 described a mindfulness-based stress reduction program for those undertaking RIA. This randomized controlled trial found an 8-week program reduced depression and anxiety and improved emotional function. This effect was particularly evident in the first 4 weeks during THW but also 3 months following treatment.
Discussion
This is the first systematic literature review of studies using patient-reported questionnaires published from 2000 to 2019 on HRQOL and TC. The authors worked independently and in collaboration to ensure robustness of the review process.
Until 2013, only five studies examined effects of surgery on HRQOL in patients with TC. They varied in their design and aims. These early studies revealed low HRQOL in patients with TC after surgery and that the extent of surgery did not have a clear effect on HRQOL. These early studies also alluded to scar and its perception as an important factor for patients.17 –21 From 2013, driven by development of new endoscopic and robotic techniques to hide visible scarring, several studies examined the impact of endoscopic/robotic techniques compared to conventional open surgery and whether improved aesthetics affected HRQOL. The symptoms of surgical scars such as pruritus, tightening, and pain also lower HRQOL.23,25 These studies, mainly arising from Korea, report improved swallow function, less scar-related symptoms, and improved HRQOL as a result of improved aesthetics from a hidden scar, particularly in setting of metastatic TC requiring additional neck dissection. In contrast, a US study showed little impact of scar visibility on HRQOL after thyroidectomy, which may be due to the cultural differences between the countries. 29 The confounding effects of disparate study groups, partly as a result of self-selection bias for those patients who underwent endoscopic versus open surgical approaches, was highlighted by multiple studies.26,29
Subsequent to changes in international guidelines (2014/2015) in the management of low-risk TC, more recent studies have explored the effect of HT versus TT, and compared HRQOL in patients with microcarcinomas undergoing surgery versus active surveillance. The HRQOL effects of TT versus HT were inconclusive, with disagreement between published articles.30,31 However, the concern of recurrence within the HT population is considerable and worthy of future research. Postoperative hypocalcemia is an important issue that is central to the debate on the benefits of HT versus TT. However, no studies examining its effect on HRQOL were revealed in this systematic review. A randomized trial to address the question of TT vs HT is soon to open in the United Kingdom (HoT trial). The primary endpoint of this study will be recurrence-free survival, but the study will also address HRQOL aspects and provide more robust data.
Patients with microcarcinomas appear to have better HRQOL compared to those who undergo HT.27,28 However, patients undergoing surveillance may have higher level of fear/anxiety of future disease recurrence. The main cause for the reported reduced HRQOL was related to physical health such as muscle discomfort, scar, and throat symptoms, which may be expected considering the short follow-up after surgery (6–8 months). The operation group had a larger cohort of females and much higher rate of ongoing thyroxine treatment. 28 There may be significant selection bias as the operated group showed lower baseline QOL scores, and there was self-selection into the surveillance group by patients with lower anxiety of recurrence. 27 Again, a prospective randomized study is required to resolve these important confounding factors.
The cost difference between endoscopic and open thyroid surgery was not explored within any included article. This important factor should be considered in future analysis of HRQOL following different surgical approaches, as the subconscious cost–benefit analysis applied by a patient may have significant implications on both short- and long-term HRQOL. This is particularly relevant to healthcare systems that financially supplement some surgical options and not others.
The effects of THW, TSH suppression, and RIA all reduce HRQOL. The negative implications on attention span, memory capability, fatigue, disturbed sleep, anxiety, depression, and distress have all been demonstrated. The use of rTSH instead of THW prior to RIA and imaging is supported by the relatively positive HRQOL. The randomized HiLo and ESTIMABL trials both support the findings from this systematic review that patients undergoing THW had significantly worse HRQOL than those receiving thyrotropin-α treatment.96,97
Rendering patients into chronic subclinical hyperthyroidism (TSH suppression) is a topic of debate, considering the potential negative implications on cardiac and bone health. This review found reports of mixed impact following TSH suppression, and that recovery of HRQOL depletion could occur with a supervised exercise routine.
We did not find any reliable evidence regarding the effect of RIA on long-term HRQOL. Any potential negative effects on HRQOL may be obviated considering the use of thyroglobulin monitoring and reassurance of all thyroid tissue being ablated could obviate these deleterious effects; however, we found no evidence to support or disprove this.
The consequences of systemic therapies on HRQOL have been poorly represented. Locati et al. 57 discuss the unlicensed use of axitinib, which maintained HRQOL. However, the use of licensed treatments (such as Sorafenib and Lenvatinib) and HRQOL has not been thoroughly explored and would be of interest. Singer et al. 89 found nine patients who had experienced tyrosine kinase inhibitor (TKI) treatment reported more frequent problems with thin or lifeless hair. Since our literature search was performed, a systematic review primarily focused on the objective response of medullary TC after TKI use has been published. This article did not include investigation into HRQOL but found moderate therapeutic benefit to their use. 98
The 2020 QaLM study investigated HRQOL for patients diagnosed with medullary TC. This prospective multicenter randomized study utilized 4 patient-reported validated QOL questionnaires and found the least popular questionnaire focused on gastrointestinal symptoms, suggesting diarrhea was not a significant concern to the study participants. 99
The review highlights diverse issues in respect to HRQOL that can be associated with detrimental outcomes following TC. There are physical, emotional, and social ramifications. The impact on HRQOL can be underestimated by professionals because, when compared to other head and neck cancers (HNCs), which might involve tracheostomy, free-tissue microvascular transfer, or chemoradiotherapy, the surgical and nonsurgical treatment of TC is less. However, from the patients’ perspective, the diagnosis of cancer can have profound negative repercussions. Although the prognosis and treatment morbidity can be much better than for other HNCs, the HRQOL response might be worse than expected given the younger age of the patient group. 100 It seems that patients with TC have been compared to healthy populations and their HRQOL much more frequently than patients with other HNCs. 100 The inference might be that their outcomes are not that different from those of noncancer comparisons, but this assessment might belittle the true impact on HRQOL of TC. Given the potential for unmet needs and the difficulties that clinicians might have to identify these in routine practice, further research has potential value around the development of a prompt list approach 101 such the Patient Concerns Inventory (PCI). 102 Fear of recurrence is a common concern across all cancers and is evident in TC in spite of a favorable prognosis. Cancer fears can be raised by patients in their consultations through a PCI approach 103 and more research in TC is needed to assess this and also the benefit of interventions such as the Mini-AFTER. 104 The other area where HRQOL information might inform future practice and clinical outcome research is around the issue of shared decision-making.
Limitations
Meta-analysis was not possible from this literature search as there was such large variation in the range of clinical characteristics and questionnaires included. Uniformity in study designs, questionnaire choice, and clinical characteristics inclusion would aid future research analysis and may enable a future meta-analysis.
The nature of patient-reported questionnaires lends itself to risk of response bias. The majority of included articles within this review were cross-sectional and as such it is difficult to conclusively report causative relationships. These factors result in most articles within this review having significant risk of bias and therefore reported outcomes should be considered within this context.
The review has not uncovered a significant number of articles focused on less prevalent TC histology, including anaplastic and medullary TC. Many articles excluded these diagnoses based on the relatively small numbers of patients. Considering this, the applicability of the findings from this review on these less prevalent TCs should be recognized. The only article focused solely on medullary TC was the one by Dadu et al., 15 in which HRQOL was a secondary outcome following the use of antidiarrheal medication.
There are a paucity of randomized controlled trials to guide TC management, and in those completed, very few use patient-reported HRQOL questionnaires. If further research expands into these domains, it would aid decision-making when clinical outcomes (e.g. recurrence risk and survival) are similar.
Conclusions
We identified, collated, and summarized a substantial number of articles published on HRQOL and TC. It can be a challenge for clinicians and researchers to find all the relevant articles and this structured review gives a synopsis for those published between 2000 and 2019. HRQOL is a crucial outcome following TC, even more so as the prognosis generally is favorable and survivorship is increasing. This review identifies areas for improved clinical care and research regarding TC, including uniformity in validated questionnaire use and the prospect of future randomized controlled trials encompassing HRQOL to enable holistic care of patients diagnosed with and treated for TC.
Footnotes
Acknowledgements
The authors thank the librarians who assisted in performing the literature searches.
Author Contributions
E.G. Walshaw: Literature searching, analysis of literature, drafting of work, final approval. M. Smith: Literature searching, analysis of literature, drafting of work, final approval. D. Kim: Analysis of literature, drafting of work, final approval. J. Wadsley: Analysis of literature, drafting of work, final approval. A. Kanatas: Conception of work, literature searching, analysis of literature, drafting of work, final approval. S.N. Rogers: Conception of work, literature searching, analysis of literature, drafting of work, final approval.
Declaration of conflicting interest
J.W. has received research funding from AstraZeneca and Sanofi-Genzyme and has received payment for acting in an advisory capacity for AstraZeneca, Sanofi-Genzyme, Eisai, Lilly, Ipsen, and Roche.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.