
Abstract
Objective
To describe a rare case of concurrent emphysematous cholecystitis, emphysematous cholangitis, and ischemic bowel in an older patient.
Conclusions
Emphysematous cholangitis is a life-threatening condition requiring prompt computed tomography–based diagnosis and urgent multidisciplinary management with antibiotics, surgery, and endoscopic intervention.
Keywords
Introduction
Emphysematous infections of the abdomen represent severe bacterial processes characterized by gas formation within tissues. Although uncommon, these are associated with high morbidity and mortality. The reported entities of emphysematous gastritis, cholecystitis, pancreatitis, and pyelonephritis typically result from polymicrobial infections facilitated by host factors such as ischemia, diabetes, or immunosuppression.1–3
Emphysematous cholecystitis accounts for approximately 1% of acute cholecystitis cases but is associated with a significantly worse prognosis. Conversely, emphysematous cholangitis is exceedingly rare and usually coexists with cholecystitis. 1
Simultaneous occurrence of emphysematous cholecystitis and emphysematous infection in other abdominal organs has been rarely reported.3–6 Such concurrence carries a high risk of life-threatening complications if not promptly recognized and managed.
We report a unique case of concurrent emphysematous cholecystitis, emphysematous cholangitis, and ischemic bowel in an older hemodialysis patient, highlighting the diagnostic and therapeutic challenges.
Case report
The reporting of this study conforms to the Case Report (CARE) guidelines. 7
An 88-year-old hypertensive man with end-stage renal disease who was on hemodialysis presented with a 24-h history of nausea, vomiting, abdominal fullness, watery diarrhea, and intermittent drowsiness.
On arrival at the emergency department of Chang Gung Memorial Hospital, Linkou, Taiwan, in July 2023, the patient’s vital signs were as follows: (a) heart rate, 135 bpm (indicative of tachycardia); (b) blood pressure, 135/61 mmHg; and (c) body temperature 36.4°C. The abdomen was distended without peritoneal signs. Laboratory tests revealed leukocytosis (12,600/μL), bandemia (5%), markedly elevated C-reactive protein (140 mg/L), and severe lactic acidosis (lactate 113.95 mg/dL ≈ 6.33 mmol/L).
Contrast-enhanced abdominal computed tomography (CT) demonstrated intramural gas within the gallbladder wall (Figure 1) and distal common bile duct (CBD) (Figure 2), consistent with emphysematous cholecystitis and cholangitis. Imaging revealed no portal venous gas or thromboembolic occlusion involving the mesenteric arteries or veins.

Intramural air (arrow) within the gallbladder wall consistent with emphysematous cholecystitis.
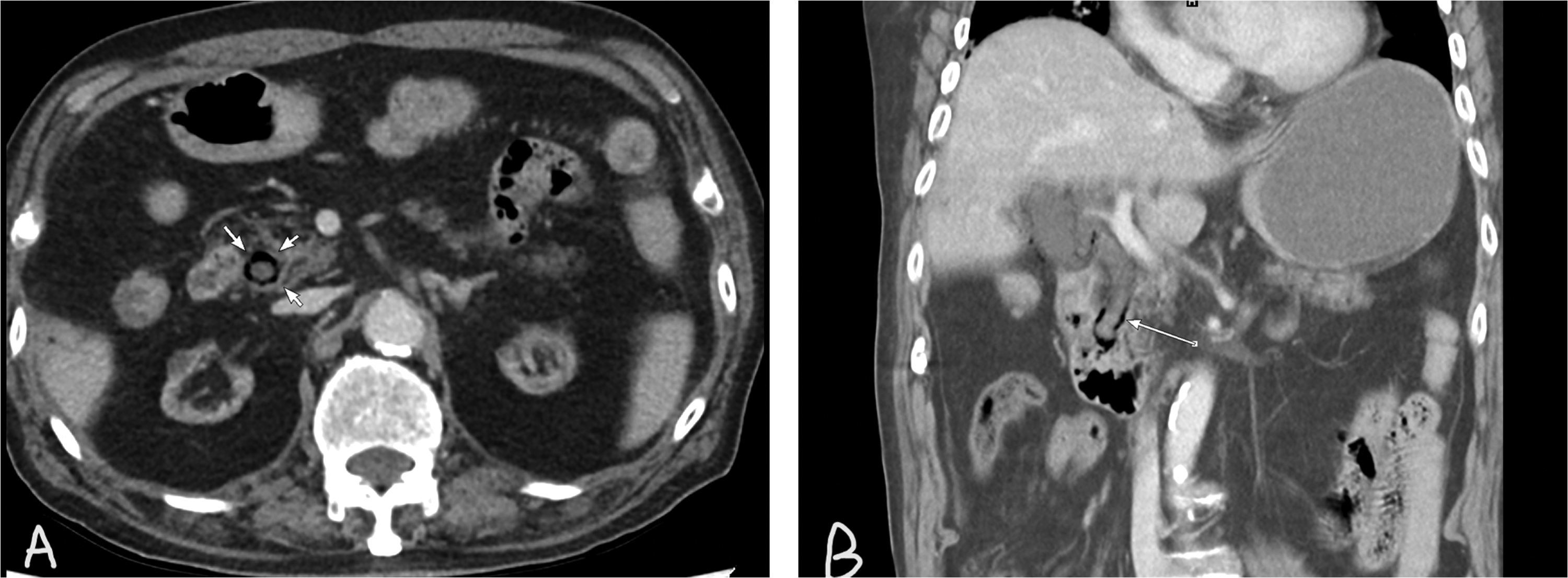
(a and b). Circumferential intramural gas (arrow) outlining the distal CBD on (a) axial and (b) coronal CT views, representing emphysematous cholangitis. CBD: common bile duct; CT: computed tomography.
Emergency exploratory laparotomy revealed a gangrenous gallbladder containing gas and bowel necrosis extending from the terminal ileum to the ascending colon. Cholecystectomy and segmental bowel resection were performed.
Postoperatively, the patient developed localized abdominal pain. Follow-up CT revealed fluid collection suggestive of bile leakage, which was confirmed on endoscopic retrograde cholangiopancreatography (ERCP), originating from the cystic duct stump. ERCP also revealed distal CBD irregular narrowing (Figure 3). A pigtail biliary stent was subsequently placed to manage the leakage and ensure biliary drainage.
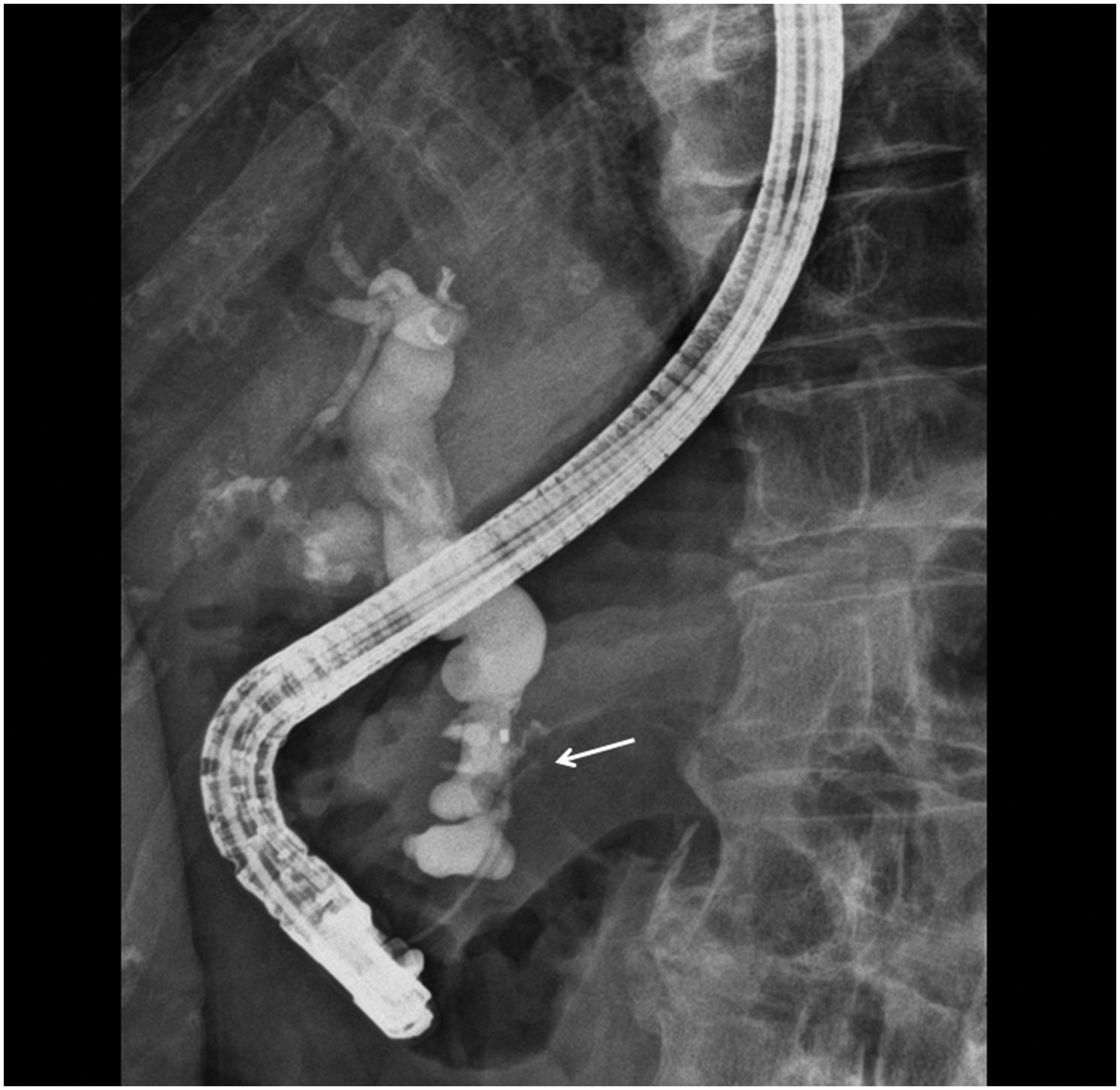
ERCP performed after cholecystectomy demonstrates a bile leak originating from the cystic duct stump as well as irregular narrowing of the distal CBD (arrow). ERCP: endoscopic retrograde cholangiopancreatography; CBD: common bile duct.
Bile cultures grew Clostridium perfringens and Streptococcus anginosus. The patient received broad-spectrum antibiotics and gradually recovered. He was subsequently discharged in stable condition.
Discussion
Emphysematous cholecystitis, a fulminant variant of acute cholecystitis caused by gas-forming organisms, typically affects older or immunocompromised individuals. 2 Despite its rarity, it is associated with poor prognosis, with mortality rates reaching 15%. 2 The concomitant or isolated presence of emphysematous cholangitis is even more critical, with an associated mortality rate of 16.7%, which is notably higher than the 5.1% reported for grade III acute cholangitis in the Tokyo Guidelines. 1
Emphysematous cholangitis, defined by gas within the biliary wall or lumen, is even rarer and is usually related to cholecystitis. The pathogenesis may involve direct extension from the gallbladder or hematogenous seeding of the biliary tree by gas-forming organisms. 3 Clostridium species are frequently implicated.6,8,9
The coexistence of emphysematous biliary infection and intestinal ischemia, as observed in our case, has been poorly documented in the literature. This rare combination suggests a severe systemic insult—either vascular or septic—that compromises tissue oxygenation in multiple organs.
CT is comparable to ultrasound and demonstrates high sensitivity (approximately 84%–90%) and specificity (up to 100% in some series) in the diagnosis of complicated biliary disease. 10 CT played a pivotal diagnostic role in our case, accurately detecting intramural gas in the gallbladder and CBD while excluding other gas-forming conditions such as portal venous gas and juxta-papillary duodenal diverticulum. Correlation with clinical history is essential to exclude iatrogenic introduction of air as a potential cause of the emphysematous changes within the CBD. The circumferential intramural air distribution along the distal CBD was particularly characteristic of emphysematous cholangitis.
Management requires a multidisciplinary approach in accordance with the Tokyo Guidelines, 2018. 11 Prompt correction of metabolic acidosis and initiation of broad-spectrum antibiotics covering gram-negative and anaerobic pathogens are essential. Biliary decompression via ERCP or percutaneous drainage, along with surgical removal of necrotic tissue, is key to improving survival rates.
In our case, postoperative bile leakage was successfully managed endoscopically, illustrating the complementary roles of surgery and ERCP in treatment. This highlights the need to remain vigilant for postoperative complications and integrate imaging with interventional therapy.
Concurrent emphysematous cholecystitis and emphysematous cholangitis with ischemic bowel is an exceptionally rare and life-threatening condition. CT is indispensable for early detection and differentiation from other causes of intramural gas. Timely multidisciplinary management, including antibiotics, acidosis correction, surgery, and endoscopic intervention, is vital for improving patient outcomes. Clinicians should maintain awareness of this entity, especially in older and immunocompromised patients presenting with sepsis of abdominal origin.
Footnotes
Acknowledgments
We want to thank our colleagues from the Department of Radiology and all the staff members at Chang Gung Memorial Hospital involved in the management of the case.
Authors’ contributions
C-H W drafted the manuscript. S-C K and B-C L performed the surgery. C-H W, Y-C W, S-C K, and B-C L collected and analyzed clinical and imaging data. C-H W critically revised the important intellectual content. C-H W edited the manuscript. C-H W reviewed the draft. All authors read and approved the final manuscript.
Availability of data and materials
The data supporting the conclusion of this article are included within this manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Disclosure statement
We do not have any existing or potential financial or proprietary interest in the material discussed in the manuscript, including employment, consultancies, stock ownership, honoraria, and paid expert testimony.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Research ethics and patient consent
All procedures performed in the study involving human participant were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. We obtained Institutional Review Board (IRB) approval for this study from the Chang Gung Medical Foundation Institutional Review Board, IRB No.: 202501318B0. The need for informed consent was waived. We sincerely thank our institution’s faculty ethics committee and chief privacy officer for reviewing this manuscript.