
Abstract
In this report, we present a case of a patient with bile peritonitis caused by gallbladder perforation associated with acute cholecystitis, which required intensive postoperative care. The patient was a woman in her 40s who presented with abdominal pain. Upon examination, she was diagnosed as having acute cholecystitis and bile peritonitis caused by gallbladder perforation. Subsequently, a partial cholecystectomy, omental pack, and drainage were performed. Initially, her bile duct enzyme levels improved; however, they subsequently increased again. An endoscopic nasobiliary drainage tube was inserted, and thereafter, a decrease in inflammatory response and bile duct enzyme levels was observed. During the course of treatment, respiratory failure and renal impairment occurred, necessitating mechanical ventilation management and continuous hemodiafiltration. In patients with severe acute cholecystitis, in addition to treating the underlying condition, it is crucial to perform procedures perioperatively, in anticipation of the development of additional organ dysfunctions postoperatively.
Keywords
Introduction
Acute cholecystitis is a frequently encountered disease in clinical practice. It is estimated that 1%–4% of patients with gallstones develop associated complications, such as acute cholecystitis, each year. 1 The management of acute cholecystitis requires not only local interventions (such as surgery or drainage) but also perioperative care focusing on systemic management after the intervention. 2 Furthermore, in cases of severe inflammation, acute renal impairment, shock, liver dysfunction, and signs of disseminated intravascular coagulation, careful monitoring, and appropriate management of organ function are necessary from an early stage. 3 Considering the possibility of the exacerbation of cholecystitis and deterioration of the overall condition of a patient leading to a critical situation, the early and accurate diagnosis of acute cholecystitis, determination of appropriate treatment strategies, and timely implementation of treatments are essential. In this report, we present a case of a patient with bile peritonitis caused by gallbladder perforation associated with acute cholecystitis, who required intensive care postoperatively. The patient provided written, informed consent for the publication of this case report.
Case presentation
The patient was a woman in her 40s, with a height of 148 cm and a weight of 60 kg. She had no notable past medical history. Three days before admission, she developed a fever of about 38 °C, as well as coughing. The following day, she began to have abdominal pain, with no bowel movements. As her symptoms worsened and she had difficulty moving, she was transported to our hospital by ambulance. Upon arrival, she was conscious and alert, with a blood pressure of 133/91 mmHg, a heart rate of 146 bpm, peripheral oxygen saturation of 90%, and a body temperature of 38.2 °C. Regarding the blood test results, she had a white blood cell count of 27,100/μL and a C-reactive protein level of 49 mg/dL, indicating an increased inflammatory response. Her liver enzyme and bile duct enzyme levels were increased, with aspartate aminotransferase at 68 U/L, alanine aminotransferase at 266 U/L, lactate dehydrogenase at 323 U/L, and total bilirubin at 3.5 mg/dL. In addition, renal dysfunction was observed, with her blood urea nitrogen level at 40 mg/dL and serum creatinine (Cr) at 2.8 mg/dL. A blood gas analysis performed under atmospheric pressure demonstrated the following values: pH 7.42, arterial partial pressure of oxygen (PaO2) 60 mmHg, arterial partial pressure of carbon dioxide 40 mmHg, bicarbonate ion 26 mmol/L, base excess 1.0 mEq/L, arterial oxygen saturation 90%, and lactate 1.6 mmol/L. These results indicated a slight decrease in oxygenation and an increase in lactate levels. A computed tomography scan was performed to investigate the cause of the abdominal pain and displayed irregularities in gallbladder morphology and evidence of adhesion between the gallbladder and the duodenum (Figure 1). Furthermore, the presence of ascites was observed. Based on these findings, the patient was diagnosed as having bile peritonitis caused by gallbladder perforation, necessitating emergency surgery. Simultaneously, based on the examination findings, a diagnosis of severe acute cholecystitis (bile peritonitis) and severe sepsis was made. Blood cultures were obtained, and the administration of antibiotics (tazobactam/piperacillin) was initiated. During the surgery, bile-containing peritoneal fluid was found around the gallbladder, and strong inflammatory adhesions were observed in the greater omentum. Owing to the extensive adhesions between the gallbladder and surrounding tissues, detachment and extraction of the gallbladder was concluded to be difficult. Therefore, a partial cholecystectomy was performed, and gallstones were removed (Figure 2). The opened gallbladder was filled with the greater omentum, and subsequently, the abdominal cavity was irrigated, and the procedure was completed. The anesthesia time was 4 h and 6 min, surgical duration was 2 h and 59 min, estimated blood loss was 506 mL, urine output was 60 mL, and water balance was +1300 mL. Her intraoperative hemodynamics remained stable without the use of any vasopressor agents. After the surgery, the patient was admitted to the intensive care unit (ICU). Blood cultures were taken upon hospital admission and at the time of ICU admission, but no bacterial growth was detected in either culture. In addition, no bacterial growth was observed in the analysis of the intraoperative ascitic fluid. On day 2 of ICU admission, the patient developed acute respiratory failure (PaO2/fraction of inspired oxygen (FiO2) ratio <200) and required mechanical ventilation. Furthermore, owing to worsening renal function with a serum Cr level of 4.4 mg/dL, continuous hemodiafiltration (CHDF) was initiated. On day 6 of ICU admission, the patient’s oxygenation improved, and she was successfully weaned off the mechanical ventilator. On day 9 of ICU admission, owing to the recurrence of an increase of bile duct enzyme levels, endoscopic retrograde cholangiopancreatography (ERCP) was performed to investigate the cause (Figure 3). During the ERCP, no apparent biliary obstruction was found, but biliary sludge discharge was observed. Therefore, an endoscopic nasobiliary drainage (ENBD) tube was inserted. Continuous drainage was observed through the ENBD tube, and bile duct enzyme levels significantly decreased over time. Moreover, following the insertion of the ENBD tube, the infection gradually came under control, and the inflammatory response decreased (Figure 4). On day 18 of ICU admission, the patient was transferred to a general ward. Because of prolonged decline in renal function, the patient was on dialysis three times a week in the general ward. The patient’s renal function gradually improved and she no longer needed dialysis, so she was discharged from the hospital on the 50th day after surgery.

Abdominal computed tomography image of the patient.

Surgically removed gallbladder and gallstones.

Changes in white blood cell and C-reactive protein levels.
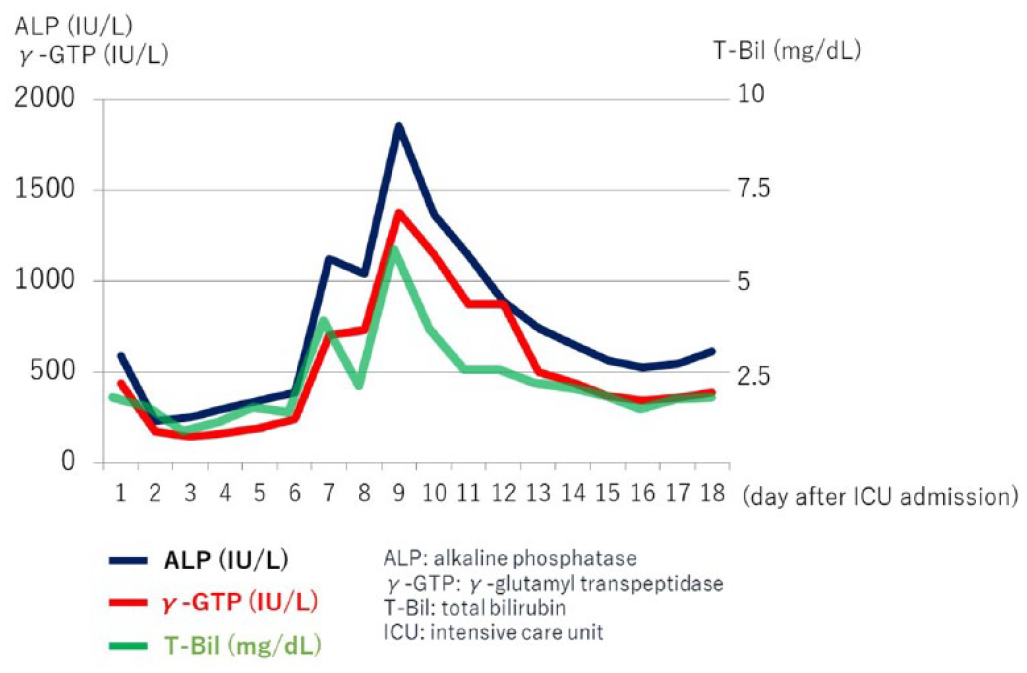
Changes in biliary enzyme levels.
Discussion
Here we reported a case of a patient with acute cholecystitis who underwent surgical treatment. However, there was inadequate control of the infection, and subsequent insertion of an ENBD tube gradually led to a decrease in the inflammatory response. Acute cholecystitis is a common condition that can vary in severity, ranging from mild inflammation that can be treated with oral antibiotics, to severe cases involving septic shock and biliary peritonitis, which may require specific interventions. 4 Acute cholecystitis is characterized by acute inflammation of the gallbladder, with 95% of cases being attributed to gallstones, known as acute calculous cholecystitis. 5 This is considered to be caused by the impaction of gallstones in the cystic duct, leading to obstruction. This causes stagnation of bile in the gallbladder, resulting in injury to the gallbladder mucosa and subsequent activation of inflammatory mediators, leading to acute cholecystitis. On the other hand, the causes of acute acalculous cholecystitis, which is not associated with gallstones, can vary and include impaired blood supply to the gallbladder, chemical injury, bacterial or parasitic infection, connective tissue disorders, total parenteral nutrition, allergic reactions, and postoperative complications. 6 In addition, inflammation progressing to ischemia and necrosis can cause gallbladder perforation, and it has been reported that gallbladder perforation occurs in 2%–11% of patients with acute cholecystitis. 7 Gallbladder perforation is reported to be more common in men, but the present case was in a woman. The mortality rate of gallbladder perforation is reported to be 9.5%, emphasizing the importance of its early diagnosis and treatment. 8 In the present patient, the abdominal cavity was initially observed using laparoscopy, revealing gallbladder perforation and extensive adhesions. Laparoscopic surgery was hence considered to be difficult, so the approach was switched to open surgery, and cholecystectomy was performed. Regarding the management of acute cholecystitis, there is ongoing debate regarding the best timing for cholecystectomy, the type of surgery (laparoscopic or open), and the use of a cholecystostomy tube. 9 In this case, the patient was relatively young and did not have any coexisting complications, such as cardiovascular disease, which led to the decision for early surgery.
According to the Tokyo Guidelines 2018, the severity of acute cholecystitis is classified into three categories; that is, severe, moderate, and mild, based on the presence of organ dysfunction (circulatory, central nervous system, respiratory, renal, hepatic, and coagulation abnormalities), increased white blood cell count, physical signs of cholecystitis, and local inflammatory signs. 10 As this patient had respiratory dysfunction (PaO2/FiO2 ratio <300) and renal dysfunction (Cr > 2.0 mg/dL), she was diagnosed as having severe acute cholecystitis (Grade III) according to this classification. In cases of severe acute cholecystitis, the administration of antibiotics, organ support, and early surgery are recommended. The patient in this case was able to undergo early surgery, which is favorable for the management of severe acute cholecystitis. However, owing to the severe inflammation caused by acute cholecystitis, the invasiveness of anesthesia and surgery, and contamination of the bloodstream with infected bile, the patient developed severe sepsis leading to acute lung injury and acute kidney injury. Therefore, organ support, such as mechanical ventilation and CHDF was required for these affected organs. In the present patient, procedures to manage organ dysfunction were provided in a timely manner without delay. Additionally, after surgery, an improvement in the inflammatory response and improvement in hepatic enzyme levels associated with the biliary system were observed. However, owing to the inefficient drainage of the bile duct, there was a recurrence of the increase in biliary enzymes, and as a result, an ENBD tube was inserted on day 9 of ICU admission. Subsequently, there was a trend of improvement in inflammatory signs and organ dysfunction. In the perioperative management of severe cholecystitis complicated by severe sepsis, it is important to be vigilant about the development of additional organ dysfunctions in addition to preexisting organ impairments. Therefore, close collaboration between the surgeon and the anesthesiologist, starting from the intraoperative period, is crucial for appropriate intensive care management.
Conclusion
We performed perioperative management in a patient with severe acute cholecystitis that was complicated by gallbladder perforation. In addition to surgical intervention, we recognized the importance of proactive perioperative management to address the possible development of additional organ dysfunctions postoperatively.
Footnotes
Acknowledgements
The authors would like to thank H.A. Popiel for English language editing.
Author contributions
Y.I. contributed to the anesthesia management of the patient, conceptualization of the case report, and writing of the original draft. S.S., Y.T., and A.K. edited the article. M.T. was the overall supervisor of this case. All authors read and approved the final article.
Availability of data and material
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written, informed consent was obtained from the patient for the publication of this case report and its accompanying images.