
Abstract
Objective
To evaluate the repeatability and reproducibility of central axial length and peripheral axial length measurements in children using the Swan 660 M.
Methods
This cross-sectional study was conducted from August to September 2024. A total of 60 children (6–15 years; no significant ocular diseases) were recruited from Zhoupu Hospital, Shanghai (30 males and 30 females; mean age 10.67 ± 2.47 years), and only right eyes were included in the analysis. The Swan 660 M was used to measure central axial length and peripheral axial length. Measurement variability across operator and time was evaluated using the intra-group SD, test–retest repeatability, coefficient of variation, and intraclass correlation coefficient.
Results
The Swan 660 M demonstrated good repeatability and reproducibility for the measurements of central axial length and most peripheral axial length points, including Nasal 1, Temporal 1, Temporal 2, and Temporal 3 (coefficient of variation <5%, intraclass correlation coefficient >0.9). However, measurement reliability was lower for certain peripheral axial length points, such as Nasal 5 (intraclass correlation coefficient <0.75). The device also showed high stability in the measurements of central axial length (intraclass correlation coefficient = 0.999).
Conclusions
The Swan 660 M demonstrates high repeatability and reproducibility for central axial length and most peripheral axial length measurements in children, suggesting its potential application in tracking the progression of myopia and investigating the relationships between peripheral retinal morphology and refractive status in this population.
Keywords
Introduction
With the increased use of electronic devices and reduced time spent outdoors, childhood myopia has emerged in recent years as a major global public health concern.1,2 Existing data indicate that by 2050 an estimated 4.758 billion individuals worldwide will be affected by myopia, accounting for 49.8% of the global population. 3 Currently, myopia shows a trend toward earlier onset and higher incidence, and dioptric power tends to increase progressively with age. Therefore, children with rapid early myopia progression constitute a priority group for myopia control. Prior studies have identified ocular biometric parameters as key determinants of myopia. Comprehensive investigation of these parameters is essential for developing effective interventions for childhood myopia.4–6 In China, pediatric ocular biometry primarily includes refraction, lens thickness, axial length (AL), corneal curvature, and anterior chamber depth.6,7 As AL, including central axial length (CAL) and peripheral axial length (PAL), can be obtained noninvasively and conveniently with stable outcomes and is unaffected by accommodative status, it has gained increasing attention and widespread application in childhood myopia prevention and control.5,8,9
Optical biometers remain the gold standard for measuring CAL and PAL. Their noncontact nature for obtaining measurement avoids patient discomfort and corneal complications associated with contact-based methods. These devices offer high repeatability with user-friendly operation, which has led to their widespread use in diagnosing pediatric ocular conditions.8,10 A variety of optical biometers are available internationally, including the IOLMaster 500 (Carl Zeiss; Germany), Lenstar (Haag-Streit AG; Switzerland), Aladdin (Topcon; Japan), Pentacam AXL (Oculus; Germany), and IOLMaster 700 (Carl Zeiss; Germany). 11 The Swan 660 M optical biometer is a newly developed domestic instrument from China. Based on optical low-coherence reflectometry (OLCR) implemented via a Michelson interferometer architecture, it measures PAL with retinal contour visualization and enables assessment from parafoveal eccentricities spanning 0°–30° nasally and temporally. Although reports indicate that a new OLCR device from the same series as the Swan 660 M shows no statistically significant difference compared with the IOLMaster 500 in CAL measurements, 12 a separate project using an agreement-based study design is underway comparing CAL and other biometric parameters with a gold-standard biometer. This complementary work will provide accuracy data that cannot be obtained for PAL in the current study.
However, to date, no studies have reported the accuracy and repeatability of the Swan 660 M for the simultaneous measurement of CAL and PAL.
This study aimed to evaluate the repeatability and reproducibility of the Swan 660 M in measuring CAL and PAL in a pediatric cohort, thereby providing clinical evidence for the widespread application of this novel PAL measurement device and offering a new reference for developing personalized myopia prevention and control strategies.
Materials and methods
Participants
This cross-sectional study consecutively enrolled 60 children who attended the Ophthalmology Clinic of Zhoupu Hospital, Pudong New Area, Shanghai, from August to September 2024. Only the right eye of each participant was included in the analysis. The cohort comprised 30 males (50%) and 30 females (50%), with a mean age of 10.67 ± 2.47 years (range, 6–15 years) and a cycloplegic subjective refraction spherical equivalent of −1.66 ± 1.75 D. The study was conducted in accordance with the principles of the Declaration of Helsinki (1975, as revised in 2024) and was approved by the Medical Ethics Committee of Zhoupu Hospital, Pudong New Area, Shanghai (Approval Number: 2023-C-189-E01; Approval Date: 26 October 2023). Written informed consent was obtained from the guardians of all participants after an explanation of the study objectives. Details of all participants were deidentified.
Inclusion criteria
Inclusion criteria were as follows: (a) age 6–15 years; (b) best-corrected visual acuity (BCVA) ≥1.0 in both eyes; (c) normal intraocular pressure in both eyes (10–21 mmHg).
Exclusion criteria
Exclusion criteria were as follows: (a) strabismus, amblyopia, or a history of ocular trauma or surgery; (b) systemic diseases affecting visual or refractive development, including diabetes mellitus and atopic dermatitis;13,14 (c) ocular diseases affecting refractive development or AL measurement, including corneal disease, uveitis, glaucoma, fundus pathology, and retinal or optic nerve disorders.
Routine examinations
Uncorrected visual acuity was measured using a standard logarithmic visual acuity chart. The anterior segment was examined by slit-lamp biomicroscopy.
AL measurement procedures
CAL and PAL were measured using the Swan 660 M optical biometer (Anshikang; China). CAL was defined as the distance from the anterior corneal surface to the retinal pigment epithelium (RPE) along the visual axis. PAL was defined as the corresponding distance measured with the beam displaced from the visual axis but passing through the pupil center on the temporal (T) and nasal (N) sides relative to the foveal center at eccentricities of 5° (T1 and N1), 12° (T2 and N2), 17° (T3 and N3), 22° (T4 and N4), 26° (T5 and N5), and 30° (T6 and N6).
The Swan 660 M optical biometer is designed with a built-in fixation target system (Figure 1(a)) that uses fixation lights to guide the participant to fixate on targets at different eccentric angles. During measurement, the instrument directs the participant’s gaze toward the target using the built-in fixation light points, ensuring consistent and repeatable displacement of the laser beam relative to the visual axis. The operator aligns the device with the participant’s eye until the central light spot appears, ensuring that the laser beam is incident along the corneal normal and confirming that the participant is correctly fixating on the corresponding fixation target, as shown in Figure 1(b). The system then automatically performs beam displacement and measurement. Therefore, we did not employ external auxiliary devices or manual adjustment methods and relied solely on the device’s own optical and fixation system to achieve consistent beam displacement.
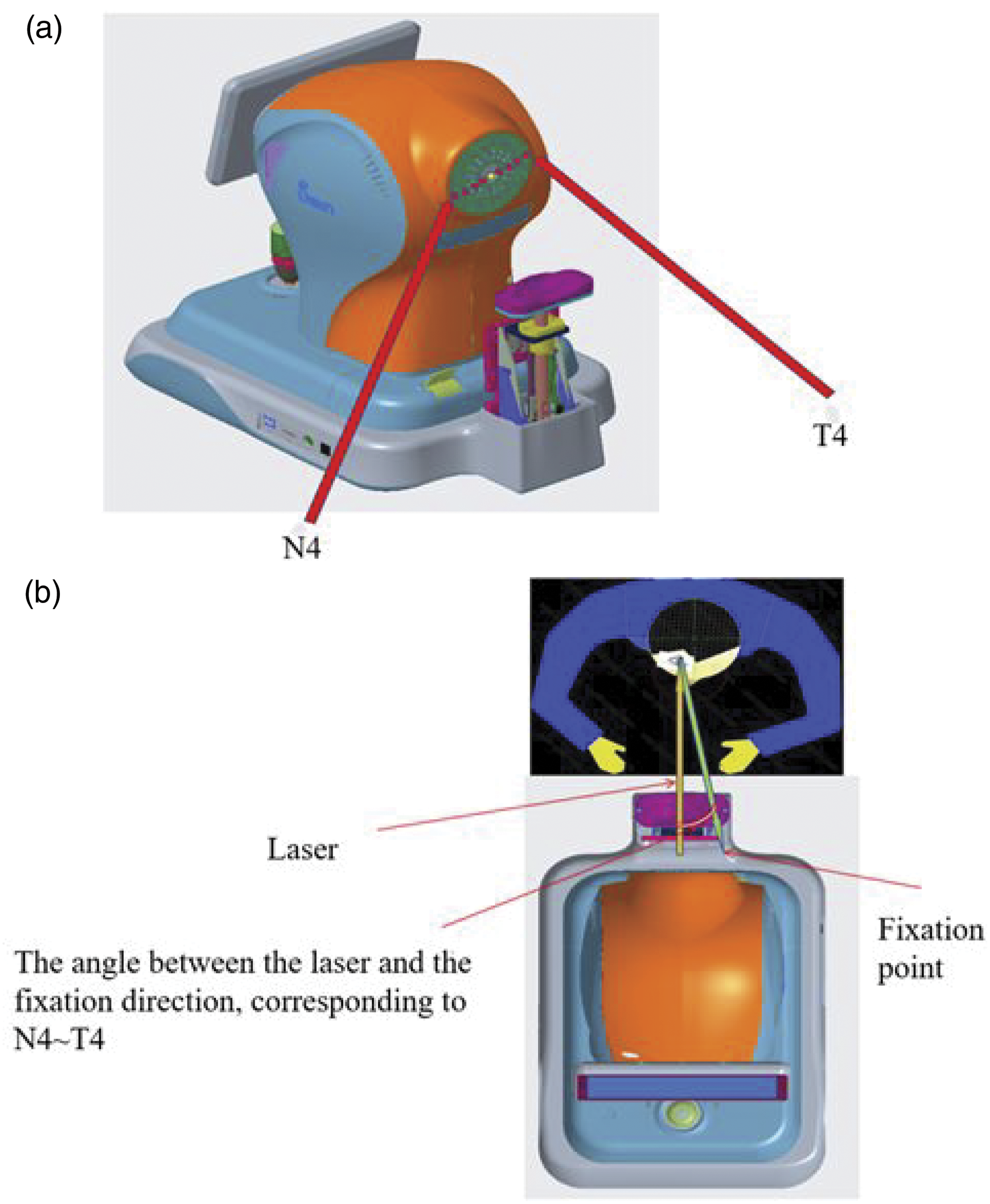
Schematic diagram of the Swan 660 M optical biometer. (a) Built-in fixation target system of the Swan 660 M and (b) schematic diagram of the beam displacement measurement principle of the Swan 660 M.
Operational details
All measurements were performed between 9:00 AM and 5:00 PM to minimize the effects of diurnal fluctuations on the measurements. AL measurement were obtained under nonmydriatic conditions. Participants were seated with their chins on the rest and foreheads against the headrest, with eyes fully open and fixating on the target light corresponding to each direction within the instrument. The operator pressed the handle button to enter measurement mode. After focusing the device on the central fixation spot, the instrument performed automatic acquisition, with the green light indicating successful measurement. The handle was then moved to the next angle. When orange light appeared, indicating abnormal acquisition, the measurement was repeated. To ensure the independence of each measurement, participants lifted their heads after each acquisition, rested for 1 min, and were then repositioned. Before the subsequent measurement, the operator refocused the device using the handle.
Outcome measures
Repeatability (within-operator variability)
The same operator performed three consecutive measurements of the right-eye AL for each participant using the Swan 660 M optical biometer within a short timeframe. Each measurement was separated by an interval of at least 30 s, during which participants were instructed to gaze into the distance to relax. This approach minimized the interference of ocular accommodation on measurement outcomes and allowed assessment of measurement repeatability.
Reproducibility (between-operator variability)
Two operators each performed one measurement of the right eye for each participant within a 1-h period. The second operator conducted the measurement at least 10 min after the first operator, allowing the evaluation of the reproducibility of the device.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) 25.0 software. All continuous variables were normally distributed, as confirmed by the Kolmogorov–Smirnov test, and are presented as mean ± SD. The within-subject SD (Sw), test–retest repeatability (TRT), within-subject coefficient of variation (CoV), and intraclass correlation coefficient (ICC) were calculated to assess repeatability and reproducibility.15,16 Sw was defined as the square root of the within-subject mean square error. TRT was calculated using the following formula: TRT = 2.77 × Sw, representing the 95% limits of the distribution of repeated-measurement differences. CoV was calculated as follows: CoV = 100 × Sw/mean, reflecting dispersion around the mean, with lower values indicating less variability and better repeatability or reproducibility. ICC was used to assess between-operator reliability and retest reliability (ICC ≥ 0.90, good reliability; 0.75 < ICC < 0.90, moderate reliability; ICC ≤ 0.75, poor reliability).
Sample size was determined based on McAlinden’s study. 17 For three measurements, a minimum of 43 eyes was required to ensure a confidence interval (CI) width of 0.15 for the estimates. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 18
Results
Repeatability analysis
The CoV values for CAL and selected PAL positions (N2, N1, T1, T2, and T3) were <5%. Except for N6, N5, and T4, CAL and other PAL measurements demonstrated good repeatability (ICC ≥ 0.90), with CAL and T1 showing the highest repeatability (ICC (95% CI) = 0.998–0.999) (Table 1).
Repeatability analysis of central and peripheral axial length measurements (mean ± SD; n = 60).

AL: axial length; CAL: central axial length; PAL: peripheral axial length; Sw: within-subject SD; TRT: test–retest repeatability; CoV: coefficient of variation; ICC: intraclass correlation coefficient; CI: confidence interval; T: temporal; N: nasal.
Reproducibility analysis
The CoV values for CAL and selected PAL positions (N2, N1, T1, T2, and T3) were <5%. Except for N6, N5, and T4, the Swan 660 M demonstrated good reproducibility for CAL and other PAL measurements (ICC ≥ 0.90), with CAL showing the highest reproducibility (ICC = 0.999; 95% CI: 0.998–0.999) (Table 2).
Reproducibility analysis of central and peripheral axial length measurements (mean ± SD; n = 60).

AL: axial length; CAL: central axial length; PAL: peripheral axial length; Sw: within-subject SD; TRT: test–retest repeatability; CoV: coefficient of variation; ICC: intraclass correlation coefficient; CI: confidence interval; T: temporal; N: nasal.
Discussion
Myopia is currently the leading cause of reduced visual acuity among school-aged children in China. Its prevalence has continuously increased over recent decades, making it a major focus in vision science. Therefore, effective control of the onset and progression of myopia carries substantial public health significance.1,2 Traditional screening indicators for myopia, including unaided distance visual acuity and noncycloplegic autorefraction, are susceptible to environmental influences, subjective factors, and accommodative function.19,20 In contrast, AL, a core mechanistic indicator of myopia onset and progression, has emerged as a key objective parameter for evaluating ocular development in children and can more accurately reflect the pathological progression of myopia.8,10
In recent years, with advancing research into the central and peripheral retina, ocular shape, and retinal contour and their relationships to refractive error, AL measurement has gained widespread attention. Commonly used metrics include CAL and PAL.21–23 The Swan 660 M optical biometer used in this study was developed on the basis of OLCR. By optimizing the light source design and employing multipath signal correction algorithms, the device markedly improves the resolution and accuracy of AL measurements. The device can simultaneously acquire multiple intraocular biometric parameters, including corneal curvature and anterior chamber depth. Its innovation lies in addressing the lack of pediatric-specific instruments for PAL measurement and in avoiding calibration-related errors associated with modified devices. Our results further confirm that the Swan 660 M exhibits minimal variability in CAL (CoV = 4.48%) and high repeatability and reproducibility (ICC = 0.999). These findings are consistent with the repeatability reported for the IOLMaster 700 and Myopia Master and are comparable to that of the gold-standard IOLMaster 500 (ICC = 1.000), thereby providing guidance and reference for clinical practice and research on visualized retinal morphology.
Currently, no gold standard exists for PAL measurement. Previous studies have assessed PAL by customizing or modifying optical biometers, including the IOLMaster and Lenstar, which are the gold-standard devices for CAL. These devices use external fixation targets to guide the eye to different eccentricities so that the instrument’s measuring beam enters the eye obliquely.24–27 For example, Mutti et al. 24 guided participants to fixate on eccentric targets on the surface of a Lenstar LS 900 to measure PAL, whereas other investigators attached external devices capable of altering fixation angles to the IOLMaster or Lenstar LS 900 to obtain PAL.25–27 However, the complexity of these procedures reduces patient cooperation and limitations in target movement and positioning accuracy compromise the stability and precision of the modified systems. Therefore, further improvements in optical biometers are required to address these shortcomings.23–27 In this study, PAL measurements obtained using Swan 660 M demonstrated CoV <5% for N2, N1, T1, T2, and T3. Except for N6, N5, and T4, PAL at other eccentricities demonstrated good repeatability and reproducibility (ICC > 0.900). These findings suggest that the Swan 660 M has strong potential for wider application in PAL measurement. Nonetheless, variability persists at extreme peripheral positions, likely reflecting the combined effects of differing inter-measurement intervals and other factors.28–30
Although the Swan 660 M performs well for measurements at most locations, the measurement variability at extreme peripheral positions may be associated with multiple potential factors. First, a nonuniform or unstable tear film can induce optical aberrations. Measurements of corneal curvature and AL rely on reflected light signals from the air–tear film interface, and tear breakup time is significantly negatively associated with the repeatability and reproducibility of measurements of the steep meridian and AL. Corneal curvature changes in peripheral regions are more complex, and the interference of tear film instability on reflected light is more pronounced. This leads to increased deviations in the reflection and refraction of incident light beams, thereby directly reducing the accuracy and repeatability of PAL measurements. In contrast, measurement signals in the central region are more stable. Second, differences in operator proficiency, particularly at peripheral positions, may introduce greater operational error. Third, children’s limited attention span and suboptimal cooperation may result in ocular movements or unstable fixation. Finally, the optical performance and calibration accuracy of the novel device at specific angles require further verification.
Limitations
This study has several limitations. 1. Agreement analyses with other optical biometers were not performed. However, in an extended study on this device, the agreement and accuracy of key indicators, including CAL and corneal curvature, were assessed against a gold-standard device. 2. The sample size was relatively small and limited to a single ethnicity. Additionally, other refractive error types, including hyperopia and astigmatism, were not included. Therefore, these conclusions require validation through large-sample, multiethnic, and multicenter clinical trials to further assess accuracy and reliability. 3. The impact of mydriasis on central and peripheral ALs was not investigated, which will be a key focus of our future research.
Conclusion
The novel Swan 660 M optical biometer demonstrates high repeatability and reproducibility for CAL and most PAL measurements in children. It shows promise for monitoring myopia progression and investigating the relationship between peripheral retinal morphology and refractive status in children, thereby supporting the development of effective myopia-control strategies. However, the accuracy of PAL measurements at the ocular peripheral margin requires further validation.
Footnotes
Acknowledgments
The authors thank all study participants and medical staff who contributed to this work.
Author contributions
Qingxia Wang: Conceptualization, data collection, and manuscript writing; Huan Yu: Statistical analysis and result interpretation; Dan Zhou: Data validation and figure preparation; Xiaoyun Ma: Study supervision and manuscript revision.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of competing interest
The authors declare no competing interests.
Funding
This work was supported by The Medical Discipline Construction Program of Shanghai Pudong New Area Health Commission (the Key Specialty Program) (PWZzk2022-10), Community Medicine and Health Management, and Evaluation of Integrated Chinese and Western Medicine Treatment (2023SQ03).