
Abstract
Objective
Retrospective database study to determine the clinical usefulness of repeat blood cultures in antibiotic-treated neonates.
Methods
Data regarding blood culture indication and findings for patients admitted to a neonatal intensive care unit (NICU) over a 2-year period were obtained from the hospital database. Repeat blood culture was defined as culture performed <7 days from initial testing in a patient receiving antibiotic treatment.
Results
Repeat cultures made up 21.3% of all blood cultures originating in the NICU (500/2352 cultures; 338 initial positive cultures; 210 patients). The most common indications for repeat culture were follow-up of clinically well babies with previous positive culture findings and the development of new symptoms. The majority of culture findings were negative (60.2%), with 7.2% indicating the presence of a new pathogen. Cultures repeated on day 5 were significantly more likely to reveal a new pathogen than those repeated on days 1–4.
Conclusions
Repeat blood cultures in neonatal patients who have developed new symptoms >4 days after initial testing may be beneficial. The use of repeat blood culture is not recommended for any other indication.
Introduction
Clinical practice, in particular in the case of neonatal medicine, is not always evidence based. This includes the use of repeat blood cultures during antibiotic treatment as a follow-up to positive culture findings, before adding a new antibiotic, or on the development of new symptoms. Repeat blood culturing is more common in neonates than in patients of other age groups, partly due to the high morbidity and mortality rates of infection in neonates, 1 and partly due to inconclusive culture findings resulting from the small volumes of blood sampled.2–4
A major drawback of repeat blood culturing is the cost of such testing. In addition, the contamination rate increases with each test performed, thereby creating diagnostic confusion and prolonging hospitalization. Such factors lead to higher hospital and pharmacy costs,5,6 and may result in increased morbidity from treatment-related side-effects and increased risk of nosocomial infection. 7 In neonates, repeat blood cultures require more blood withdrawal for the culture, and further blood tests for monitoring side-effects and drug levels; such factors contribute to the development of anaemia and the potential need for blood transfusion, especially for very low birth-weight infants. 8
The use of guidelines for repeating blood cultures has been found to decrease unnecessary testing. 9 There are no guidelines regarding repeat blood cultures in neonates, however, despite the fact that these infants are prone to multiple septic episodes during their hospital stay with a rate of sepsis higher than any other age group. 10
We hypothesized that follow-up of positive blood cultures in clinically well neonates being treated with antibiotics is a waste of resources, creates confusion regarding treatment, and does not provide additional valuable information. In order to evaluate this, we studied repeat blood culture practices in our Level 3 neonatal unit and thereafter generated a protocol for repeating blood cultures.
Patients and methods
Study population
This retrospective study included all neonatal patients (aged 0–28 days at admittance) who were admitted to the level 3 Neonatal Intensive Care Unit (NICU), Jordan University Hospital, Amman, Jordan, between August 2009 and December 2011, and underwent repeat blood cultures (<7 days after initial culture). Hospital charts were reviewed for demographic and clinical data. Data including date of culture, culture findings, time between blood cultures and the type of pathogen were recorded. The indication for repeat blood culture was determined by reviewing physicians’ and nurses’ progress notes.
The scientific research committee of the University of Jordan, Amman, Jordan approved the study. Due to the retrospective nature of the study, informed consent from participants’ parents or guardians was not required.
Blood culture protocol
According to our NICU protocol, blood was drawn for culture and antibiotic treatment was initiated under the following circumstances: prematurity (≤32 weeks’ gestational age); presence of major risk factor for sepsis (i.e. prolonged rupture of membranes); signs of neonatal sepsis. Duration of treatment depended on the clinical status of the patient, blood culture findings (positive or negative), causative micro-organism, presence of meningitis and C-reactive protein concentrations.
Peripheral blood (1 ml) was collected aseptically and placed in an aerobic bottle. Blood was then incubated for 7 days using an instrumented blood culture system (BACTEC™, Becton, Dickinson and Co., Franklin Lakes, NJ, USA). Indication for repeat blood culture was classified as one or more of the following: failure to improve/addition of new antibiotic; development of new symptoms (any symptom other than the presenting symptom developing after the initiation of treatment in a previously stable patient); follow-up of positive blood culture in clinically stable patients. All patients were receiving antibiotics when blood culture was repeated (ampicillin and an aminoglycoside or vancomycin and Imipenem). Culture findings were classified as negative, same pathogen, new pathogen or contaminant (Diphtheria spp. and Streptococcus viridans without any signs of sepsis). For the purposes of this retrospective study, coagulase-negative Staphylococcus (CONS) was classified as a separate category, to avoid the debate whether it is an infection or a contamination.
Statistical analyses
Data were presented as n (%). Cross-tabulations with Pearson’s χ2-test were used to evaluate the association between variables. P-values <0.05 were considered statistically significant. Cramer’s V is presented as a measure of effect size. Follow-up Z-tests of proportions were conducted on all significant χ 2 results. Bonferroni adjusted P-values <0.05 for pairwise comparisons were considered statistically significant. SPSS® version 21(SPSS Inc., Chicago, IL, USA) was used to conduct statistical analyses.
Results
Demographic and clinical data from 210 neonatal patients included in a retrospective study to determine the clinical value of repeat blood culture.

Findings of repeat blood cultures in neonatal patients undergoing antibiotic treatment in a neonatal intensive care unit (500 blood cultures from 210 patients).

Diphtheria spp. or Streptococcus viridians.
CONS, coagulase-negative Staphylococcus.
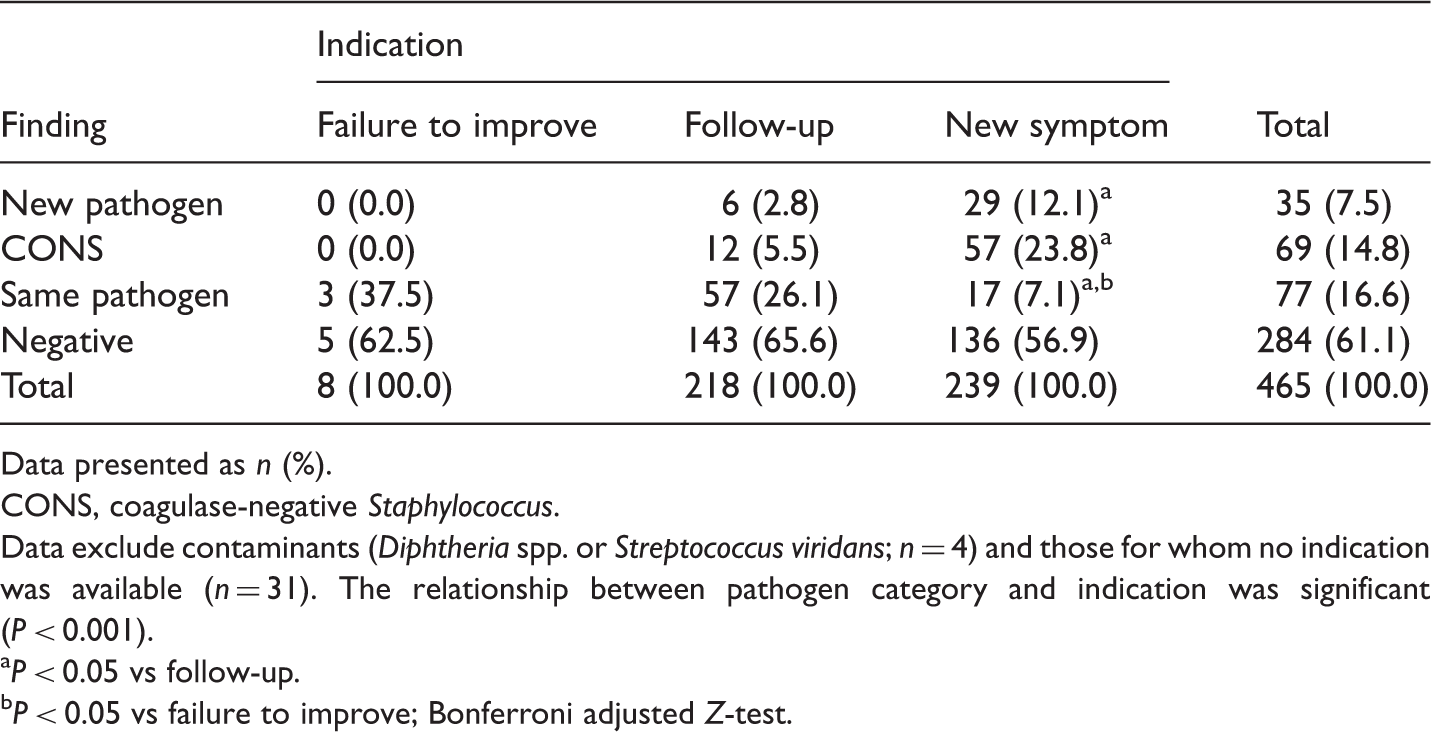
Findings of repeat blood cultures in neonatal patients undergoing antibiotic treatment in a neonatal intensive care unit, stratified according to indication for repeat culture (500 blood cultures from 210 patients).
Data presented as n (%).
CONS, coagulase-negative Staphylococcus.
Data exclude contaminants (Diphtheria spp. or Streptococcus viridans; n = 4) and those for whom no indication was available (n = 31). The relationship between pathogen category and indication was significant (P < 0.001).
P < 0.05 vs follow-up. bP < 0.05 vs failure to improve; Bonferroni adjusted Z-test.
Indication for (and findings of) repeat blood cultures in neonatal patients undergoing antibiotic treatment in a neonatal intensive care unit, stratified according to day of repeat culture (500 blood cultures from 210 patients).

Data presented as n (%).
CONS, coagulase-negative Staphylococcus.
Significant relationships were found between indication category and days between the repeat culture (P < 0.001), and between new pathogen and days between repeat culture (P < 0.001). For analysis of indication category, the group for whom indication category was not available (n = 31) were excluded.
P < 0.05 vs day 1. bP < 0.05 vs day 2. cP < 0.05 vs day 3. dP < 0.05 vs day 4. eP < 0.05 vs day 5. fP < 0.05 vs day 6; Bonferroni adjusted Z-test.
There was a significant relationship between culture findings and day of repeat culturing (P < 0.001). Cultures repeated on day 5 were significantly more likely to reveal a new pathogen than those repeated on days 1–4 (P < 0.01). There was no statistically significant difference between day 6 and any other day (1–5). CONS was significantly more likely in cultures repeated on day 6 compared with days 1 or 2 (P < 0.05). There was no statistically significant difference in the proportion of CONS found between days 3–5 compared with days 1 or 2. A significantly greater proportion of cultures repeated on day 1 revealed the same pathogen, compared with cultures on day 2, 4, 5 or 6 (P < 0.05).
Findings of repeat blood cultures in neonatal patients undergoing antibiotic treatment in a neonatal intensive care unit, stratified according to day of repeat culture (500 blood cultures from 210 patients). Patients were additionally stratified according to indication for repeat culture (new symptom or follow-up).

Data presented as n (%).
CONS, coagulase-negative Staphylococcus.
Significant relationships were found between pathogen category and day of repeat for new symptoms (P = 0.011), and for day of follow-up (P = 0.005).
P < 0.05 vs day 3. bP < 0.05 vs day 1; Bonferroni adjusted Z-test.
Discussion
Blood culture is the gold standard for diagnosing sepsis 9 but its reliability is affected by many factors,2–4 leading to inconclusive findings and repeated testing. 10 Clinicians have traditionally considered a negative blood culture as objective proof of treatment success. The use of repeat blood cultures in adult patients undergoing antibiotic treatment has been found to be unnecessary,11,12 but this subject has not been studied in the paediatric age groups of patients. The present study investigated repeat blood culture practice in our NICU, and the resulting data were used to generate guidelines for repeat blood culture in neonatal patients receiving antibiotic treatment.
In adults, an additional blood culture is defined as a repeat if it occurs at any point during a hospital stay. 9 Newborn babies, especially if premature, may develop sepsis multiple times during their hospital stay, and commonly undergo multiple blood cultures. Empirical treatment of suspected sepsis with negative culture takes 7 days, 13 therefore we defined repeat blood culture as any blood culture that was taken within 7 days of the initial sample.
In our hospital, 21.3% of all blood cultures requested by the NICU were defined as repeat cultures, representing a significant economic burden beyond the cost of testing. This includes the increased contamination rate due to the high number of cultures, resulting in unnecessarily prolonged treatment and hospitalization, 6 and possible increases in morbidity. High numbers of repeat cultures can result in a heightened requirement for blood transfusion, particularly in premature infants. In addition, the side-effects of prolonged antibiotic treatment due to confusing culture findings are unjustifiable, and may play a role in the development of antibiotic resistance.
The two main indications for repeat culture in the present study were the development of new symptoms or for the purposes of follow-up (i.e., documenting treatment response in clinically improving patients). The majority of repeat culture findings in these two categories were negative, with only 7.2% of cultures revealing the presence of a new pathogen. When cultures that indicated the same pathogen are included in these data, 75.8% of repeat cultures in the present study provided no new information. In the follow-up group, repeat cultures performed early in the treatment course showed a high percentage with the same pathogen, as expected. This information is of limited benefit and may lead to unnecessary changes (or additions) to the antibiotic regimen. In the new symptom group, the majority of cultures repeated within 4 days were found to be negative. We consider that the new symptoms presenting during this time were likely to have resulted from the same septic episode for which treatment was initiated.
Although the number of cultures in the ‘failure to improve’ category was small in the present study (n = 8), 37.5% of results indicated the presence of the same pathogen as the original culture. This suggests that antibiotics were unable to control the infection in this group, justifying the use of repeat culture in this small category of patients.
The relationship between the day of repeat culture and the presence of a new pathogen (for all indications studied) reached significance on day 5 in the present study, indicating that performing repeat culture during the first 4 days of treatment provided no extra information.
Based on the findings of our study, we have developed the following protocol for repeating blood culture in neonatal patients: (i) consider clinical status, antibiotic coverage and time since initial culture; (ii) repeat blood culture is not recommended to document a negative result in clinically stable, antibiotic-treated patients; (iii) in the case of new symptoms, repeat blood culture within 4 days of initial test is not recommended; (iv) repeat blood culture in patients who have developed new symptoms later than 4 days after initial test may be beneficial.
These guidelines require further validation by prospective studies, and may not apply in the case of patients with central line-related or fungal infections.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was funded by the Deanship of Scientific Research at the University of Jordan.