
Abstract
Objective
Surgery for aphakic eyes without capsular bag support is challenging and remains a key area of research for ophthalmologists. This retrospective study introduces a novel surgical method for suture fixation of intraocular lenses in such eyes.
Methods
The modified surgery was performed on eight eyes without a natural lens. The two haptic tabs of the three-piece intraocular lens were secured with two crystal sutures using a wireless junction—defined as a connection point where the loop or haptic is anchored to the eye wall without knots through techniques such as intrascleral pocket embedding, flanged end creation, or sutureless tuck—without creating a scleral flap.
Results
All eight patients demonstrated improved postoperative visual acuity. The intraocular lenses were reliably fixed, properly centered, and well positioned. No serious complications occurred after the surgery.
Conclusions
This modified technique appears to offer procedural simplification and a favorable trend in postoperative visual acuity improvement. However, its long-term safety and efficacy require confirmation through larger, controlled studies.
Keywords
Introduction
Intraocular lens (IOL) implantation, a standard procedure in cataract treatment, has become one of the most commonly performed surgeries worldwide. 1 However, IOL implantation in the capsular bag or ciliary sulcus can be challenging in certain patients due to factors such as capsular bag rupture, suspensory ligament rupture, lens dislocation, postoperative ocular trauma, or prior vitrectomy. Consequently, there remains a need to improve IOL suture fixation—a surgical technique used to secure an IOL to the scleral wall using sutures when the natural lens capsule provides insufficient support.
Early IOL suture procedures present several challenges, including prolonged surgical duration, strict requirements for lens type, blood accumulation in the vitreous cavity, suture knot reactions, lens displacement, and a steep learning curve for surgeons. 2 In aphakic eyes, maintaining intraocular pressure (IOP) and anterior chamber stability after vitrectomy is critical, as intraoperative stability directly influences postoperative outcomes. To minimize trauma and suture-related complications while achieving stable IOP, we performed the procedure in eight aphakic eyes and developed a new IOL suture technique based on previous surgical methods and our own experience.
Methods
The study was conducted in accordance with the Declaration of Helsinki (1975, revised 2024), and all patient details were de-identified. This retrospective study was reviewed and approved by the Institutional Review Committee of the General Hospital of Xinjiang Military Region, granting exemption from patient informed consent (2025RR1213). Patient data were anonymized prior to analysis. Follow-up assessments were conducted at 1 week, 1 month, and 3 months post-surgery. Corneal endothelial cell counts were measured preoperatively and at 3 months postoperatively using noncontact specular microscopy. The study was reported following the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines. 3
We consecutively included all eligible aphakic patients who underwent the modified pre-set double-wire IOL suture fixation procedure at our center between June and December 2023. All eight eyes were aphakic and lacked capsular support. Three eyes were “aqueous eyes” that underwent traumatic lens resection using a vitrectomy handpiece and subsequent vitrectomy. Two eyes had complete lens dislocation, with the lens falling into the vitreous cavity, and underwent vitrectomy. Three eyes had partial lens dislocation identified before high-power phacoemulsification. These patients underwent intracapsular cataract extraction, with the modified IOL suture fixation procedure performed in a second-stage surgery.
Preoperative visual acuity ranged from 0.05 to 0.12 on the logMAR scale. Corneal endothelial cell counts were within the normal range, and optical coherence tomography (OCT) indicated normal macular and optic disc structures.
Pre-positioned double line
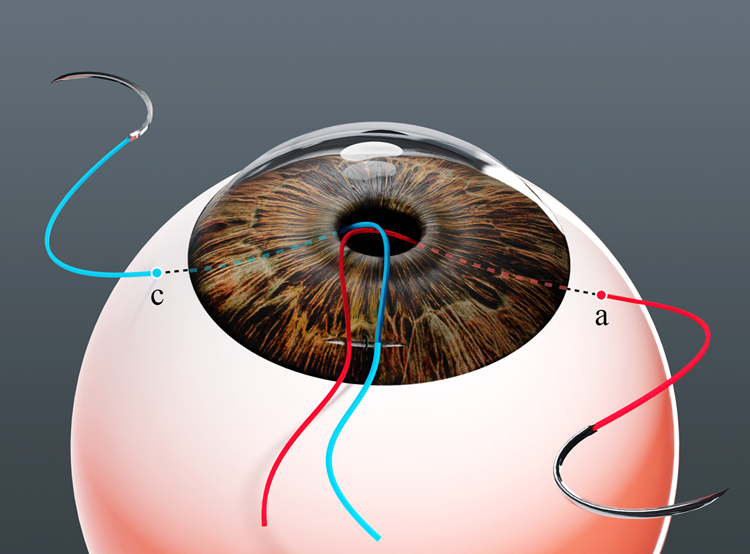
Before pupil dilation, the conjunctival sac was opened at 11 o’clock, 2 mm from the corneoscleral margin, to fully expose the peripheral sclera. The conjunctival flap measured approximately 2 × 3 mm, with adequate hemostasis achieved. From point A, the 9-0 IOL fixation suture was introduced into the eye through the flat part of the ciliary body. As the suture passed through the pupillary area, the needle and thread were brought out through the pupil, placing the suture in the anterior chamber. The needle was then advanced forward, passed through the clear cornea, and emerged externally at point B, pulling the suture with it, after which the suture was cut. Similarly, the suture was introduced at point C (4 o’clock). As it passed through the pupillary area, the needle and thread were brought out through the pupil, placing the suture in the anterior chamber. The needle was then passed through the clear cornea at the corneoscleral margin at point D and the suture was cut. At this stage, the pre-set suture was completed (Figure 1). As shown, the distances from points A and C to the limbus were both 2 mm.

Pre-positioned double-wire IOL suture.
Making an auxiliary and a main incision
First, an auxiliary incision was made at 6 o’clock, and viscoelastic was introduced through this incision. The aqueous humor was replaced, stabilizing the anterior chamber. Subsequently, the main incision was made at 12 o’clock, measuring 2.4 mm in width. At this stage, the anterior chamber was relatively stable due to the pre-set suture and the replacement of aqueous humor, allowing the operation to proceed smoothly. The sutures at point B were hooked out using an IOL manipulator or micro-forceps, and the original sutures were threaded through the main incision. Similarly, the suture at point D was hooked out, and the original suture was threaded through the self-sealing corneal incision. At this point, the anterior chamber and IOP remained stable, with one suture threaded from point A to the main incision and another from point C to the main incision (Figure 2).
Creation of an auxiliary incision and the main incision.
Lens implantation and fixation
A preloaded three-piece IOL (Hoya PY-60AD) was introduced into the anterior chamber through the main corneal incision using a viscoelastic-filled injector. The leading haptic was deliberately left outside the eye, protruding from the main incision. The main incision was temporarily closed with a single 10-0 nylon suture to maintain anterior chamber stability, while the two pre-inserted sutures originating from points A and C remained externalized at the wound.
First haptic (E) fixation: One end of the externalized suture from point A was tied to the base (E-point) of the leading haptic, approximately 2.5 mm posterior to its tip (Figure 3). After securing several knots, an IOL manipulator was used to rotate the IOL within the anterior chamber. This rotation simultaneously introduced the fixed leading haptic (E) into the anterior chamber and externalized the trailing haptic (F) through the main incision.

The other end of the suture passing through point A is fixed to the loop of the IOL that has not yet been inserted into the anterior chamber. IOL: Intraocular lens.
Second haptic (F) fixation: With the trailing haptic now externalized, the same procedure was repeated. The suture from point C was tied to the base of the trailing haptic (F-point), 2.5 mm from its tip. After securing the knots, the IOL was rotated again with the manipulator to re-introduce the second fixed haptic (F) into the anterior chamber.
At this stage, the IOL was fully positioned within the anterior chamber, with one haptic (E) connected to the suture from point A and the other haptic (F) connected to the suture from point C (Figure 4). The subsequent steps involved tensioning and securing these sutures at their respective scleral fixation points.

The other end of the suture passing through point C is fixed to the loop of the IOL that has not yet been inserted into the anterior chamber. IOL: Intraocular lens.
Suture fixation
Epinephrine was injected into the anterior chamber to dilate the pupil. After tightening the sutures, the IOL was pushed under the iris through the pupil with the crystal repositioning hook. The sutures at points A and C were tightened to stabilize and fix the crystal, confirming that the IOL was centered and free of skew, inclination, or deviation from its proper position (Figure 5). The suture with a curved needle at point A was passed through the lamina sclera from the central zone. It then traversed the interlayer for approximately 1.5–2 mm before exiting the sclera. After an interval of 1.5–2 mm, the suture re-entered the scleral interlayer following an arc-shaped path. After repeatedly crossing the lamina sclera, the radius of curvature reached nearly 3 mm, and the suture was buried in the interlaminar layer. The suture needle was then cut (Figure 6). The c-point suture was fixed using the same method. Finally, 8-0 Vicryl absorbable sutures were used to close both sides of the conjunctival sac.

The IOL is secured by sutures passing through both ends at points A and B. IOL: Intraocular lens.

Sutures are passed repeatedly through the sclera to achieve fixation.
Ethics approval and consent to participate
The experimental protocol was established in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Xinjiang Military Region General Hospital. Written informed consent was obtained from all participants or their guardians. All interventions were conducted following relevant guidelines and regulations.
Results
We retrospectively analyzed the postoperative outcomes of eight eyes from eight patients. All surgeries were performed by an experienced cataract surgeon, and the procedures proceeded smoothly, with an average operative time of 29 minutes. Patients reported no specific complaints or discomfort after surgery. No postoperative complications, such as endophthalmitis, corneal endothelial loss, secondary glaucoma, vitreous hemosiderosis, choroidal detachment, fulminant suprachoroidal hemorrhage, or macular cystoid edema, were observed. A transient increase in IOP occurred in three eyes within 3 days after surgery; it was treated symptomatically, and IOP returned to normal. Visual acuity improved to 0.5–0.8 at 1 week postoperatively and reached 1.0 in three eyes at 3 months.
At postoperative reviews in January and March, the visual acuity of all eight eyes ranged from 0.6 to 1.0, with no reported discomfort. There was no evidence of subconjunctival or scleral inflammatory reactions, suture exposure, IOL tremor (pseudophacodonesis), or IOL displacement. Individual preoperative and 3-month postoperative clinical data for all patients are presented in Table 1. Postoperatively, best-corrected visual acuity (BCVA) improved significantly in all cases (p < 0.01, paired t-test). The mean BCVA improvement corresponded to 4.7 lines on the Snellen chart (SD ± 0.63 lines). Corneal endothelial cell density decreased from a mean of 1974 cells/mm² preoperatively to 1790 cells/mm² at 3 months postoperatively, representing a mean cell loss of 9.4%. The IOL was in a normal and central position after pupil dilation, and the sutures were properly tied (Figure 7) with acceptable tension. Ultrasound biomicroscopy (UBM) and anterior segment OCT confirmed correct IOL positioning. Ultrasound examination revealed no vitreous cavity or retinal abnormalities (Figure 8). The spherical equivalent ranged from 0 to ±0.75 D, and cylinder power ranged from 0 to ±1.25 D.
Preoperative and 3-month postoperative clinical data of the patients (n = 8).

BCVA: best-corrected visual acuity; ECD: endothelial cell density.

Postoperative view showing the IOL in an upright, stable position without tilt. IOL: Intraocular lens.
Postoperative UBM image of the anterior segment. UBM: Ultrasound biomicroscopy.
Discussion
Ensuring anterior chamber and IOP stability
Maintaining a stable anterior chamber is a well-known challenge in traditional scleral-fixated IOL surgery, particularly in eyes that are fluid-filled following vitrectomy. The requirement for multiple ports and a main incision can lead to persistent aqueous egress, 4 resulting in chamber instability and an increased risk of serious complications, including suprachoroidal hemorrhage and choroidal detachment. Although anterior chamber maintainers are frequently employed to address this instability, they may introduce trade-offs, such as increased postoperative astigmatism, reduced intraoperative maneuvering space, and added complexity in suture handling. 5
Our modified technique addresses this issue through a sequenced approach designed to minimize fluid egress. First, IOL insertion and initial haptic manipulation are performed under a physiological (nondilated) pupil, which acts as a natural barrier, helping to maintain a relatively closed system and stabilize the viscoelastic-filled anterior chamber. The iris itself provides temporary support to the IOL during initial positioning. Second, key sclerotomies (Points B and D) for suture externalization are created using small-gauge needles prior to opening the main incision. Pre-placement of these sclerotomies minimizes the size and duration of simultaneously open wounds, thereby reducing uncontrolled fluid flow. Finally, after IOL insertion, the main incision is immediately secured with a single 10-0 nylon suture, and the chamber is maintained with a cohesive viscoelastic, creating a sealed environment for subsequent fixation steps. This controlled approach is designed to reduce intraoperative IOP fluctuations without the need for high-flow irrigation, which may be particularly beneficial in eyes prone to instability. 6
Simplification of surgical steps to shorten duration
A significant challenge in traditional suture fixation is the complexity and number of steps, particularly during suture externalization and haptic fixation, which often requires bimanual intraocular maneuvers (e.g. the “handshake” technique). 7 Our procedure is designed to streamline this process. By pre-positioning sutures through specific limbal/pars plana points (A, B, C, D) and using the main incision for both suture retrieval and haptic externalization, we eliminate the need for additional contralateral paracenteses solely for suture guidance. This approach reduces instrument passes and minimizes potential intraocular trauma.
The fixation process itself is further simplified. By leaving one haptic temporarily outside the eye through the main incision, the IOL fixation sutures can be tied to the haptic base (2.5 mm from the tip) under direct visualization in an extraocular manner. Sequential rotation of the IOL then allows the second haptic to be externalized for identical fixation. This “external-in” fixation method bypasses the challenge of intraocular knot-tying. Finally, the fixation geometry, with sutures securing the haptic 2.5 mm from its tip, provides a broad contact area between the haptic and the ciliary sulcus. The resulting three-plane force distribution (two suture points and the sulcus) may enhance IOL stability. 8
Wireless and knotless scleral fixation
The construction of scleral flaps to cover and secure knots in conventional methods not only prolongs surgery but also carries a long-term risk of knot erosion through ocular tissues, potentially causing inflammation or exposure. 9 To address this, we employ a wireless, knotless intrascleral fixation technique. After externalization, each end of the IOL fixation suture is routed through a circular intrascleral tunnel at approximately half the scleral thickness over a 1.5–2 mm arc and then trimmed flush. This creates a self-locking, nonsliding fixation point within the scleral lamellae, distributing tension over a broader area and eliminating the need for a superficial knot or full-thickness scleral flap.
This method offers several advantages. By omitting flap dissection and knot burial, it reduces operative time and minimizes disruption to the conjunctival and scleral surfaces. It may also lower the risk of late-onset suture-related complications, including erosion and infection. The intrascleral tract may further promote faster tissue adhesion and fibrosis, contributing to long-term IOL stabilization. 10 Compared with other knotless techniques, such as the flanged intrascleral approach, 11 our method does not require haptic externalization to create a flange, potentially preserving haptic integrity while achieving the same goal of eliminating externalized knots.
Objective comparison with existing techniques and study limitations
It is important to contextualize our findings within the range of existing secondary IOL fixation techniques. Compared with traditional ab externo sutured methods, our technique aims to enhance anterior chamber stability and simplify the procedure while retaining the fundamental use of permanent sutures. Relative to the established flanged intrascleral (or “glued IOL”) technique, our method employs a different haptic fixation mechanism (suture-based versus flange-based) and may be advantageous in cases where haptic rigidity or length is insufficient for flange creation. Unlike anterior chamber IOLs, it avoids potential compromise of the corneal endothelium or the anterior chamber angle. Compared with the Yamane technique (a double-needle flanged method), our approach uses pre-placement of all sutures and a distinct sequence for externalized haptic fixation, potentially providing a more accessible learning pathway for surgeons accustomed to suturing.
Nevertheless, the promising aspects of our modified technique must be interpreted in light of the study’s significant limitations. The most notable limitations are the small sample size (n = 8) and the absence of a control group, which preclude definitive conclusions regarding superiority. The retrospective design may also introduce selection bias. While the short-term outcomes are encouraging, long-term data on IOL stability, suture integrity, endothelial cell loss, and late complication rates are necessary but not yet available.
Conclusion
The modified pre-positioned double-wire IOL suture suspension technique demonstrates potential advantages in minimizing IOP fluctuations, shortening operative time, and achieving stable, knotless fixation. These procedural features may help reduce surgical complexity and could contribute to favorable postoperative outcomes. While our initial experience is encouraging and suggests a manageable learning curve, these findings remain preliminary. Consequently, further investigation through larger-scale, prospective, and comparative studies is warranted to rigorously evaluate the efficacy, safety, and broader applicability of this technique, particularly in complex cases such as vitrectomized eyes with fluid-filled chambers. Ensuring anterior chamber stability and controlled IOP remains a critical consideration in such procedures.
Footnotes
Acknowledgements
The authors thank the surgical and nursing teams of the Ophthalmology Department of 474 Hospital for their clinical support. We also extend our sincere gratitude to Botuhui001 for creating the illustrative figures included in this article.
Author contributions
Zhao Li and Wen Gao contributed to the study conception and manuscript drafting. Wen Gao performed data collection and statistical analysis. Yongli Yang was responsible for patient follow-up, data interpretation, and surgical technique design. Yongli Yang and Xiao Wang critically reviewed and edited the manuscript. All authors read and approved the final version of the manuscript.
Data availability statement
This article describes a surgical technique. No datasets were generated or analyzed during the current study; therefore, a data availability statement is not applicable.
Declaration of conflicting interests
The authors declare that they have no potential conflicts of interest related to the research, authorship, or publication of this article.
Funding
The authors received no financial support for this research.