
Abstract
Objectives
This study aimed to evaluate the clinical efficacy and cost-effectiveness of using a disposable bendable negative pressure suction sheath in combination with a disposable ureteroscope for treating upper urinary tract calculi and to compare it with the conventional ureteral access sheath with a lassoed mesh basket.
Methods
A retrospective analysis was conducted on clinical data from patients with upper urinary tract calculi who underwent flexible ureteroscopy at a tertiary hospital in Beijing between March 2023 and March 2024. The study included two groups: 69 patients were treated with disposable bendable negative pressure suction sheaths (negative pressure group) and 83 with conventional ureteral access sheath combined with lassoed mesh baskets (conventional group). Variables analyzed included operative time, stone-free rate, length of postoperative hospital stay, postoperative complication rate, and hospitalization cost.
Result
The operative time for the negative pressure group was 119.8 ± 10.4 min, which was longer than that in the conventional group (93.2 ± 9.8 min). The postoperative hemoglobin drop was 5.3 ± 2.2 g/L in the negative pressure group and 4.7 ± 1.2 g/L in the conventional group. The hospitalization cost for the negative pressure group was ¥28,273 ± 5389, which was significantly lower than that for the conventional group (¥30,786.1 ± 4055). The stone-free rate at 1 week postoperatively was 84.1% (58/69) in the negative pressure group, which was significantly higher than that in the conventional group (68.7%). However, there was no statistically significant difference in stone-free rate at 1 month postoperatively between the two groups.
Conclusions
The use of a disposable ureteroscope with a bendable negative pressure suction sheath can improve short-term postoperative stone-free rate. However, this approach may increase surgical complexity, extend operative time, and heighten the risk of intraoperative bleeding. This procedure is recommended to be performed by physicians with extensive experience in flexible ureteroscopy to ensure safety and efficacy.
Keywords
Introduction
Significant advancements have been made in the treatment of urinary tract calculi, a common urological condition, alongside developments in medical technology. 1 For kidney stones with a diameter of less than 2 cm, ureteroscopic lithotripsy has become the treatment of choice because of its minimally invasive and highly effective nature. 2 The introduction of various ureteral flexible lens sheaths has further improved the efficacy and safety of lithotripsy treatments.3,4 Among these, the conventional ureteral access sheath combined with a lassoed mesh basket has been widely recognized. In recent years, the bendable negative pressure suction ureteroscopic sheath has emerged as an innovative tool that can actively reduce intrarenal pressure during lithotripsy, allowing deep penetration into the renal calyces to aspirate the stones. This technique effectively reduces the risk of intraoperative complications and improves the stone-free rate (SFR).5–7
This retrospective analysis study aimed to compare the clinical efficacy of a disposable bendable negative pressure suction sheath combined with a disposable ureteroscope with that of the conventional ureteral access sheath paired with a lassoed mesh basket for the treatment of upper urinary tract calculi. We comprehensively evaluated attributes such as operative time, SFR, length of postoperative hospital stay, postoperative complication rate, and hospitalization cost. Furthermore, to provide a more scientific and reasonable treatment option for urinary tract stones and promote the further development of ureteral flexible lens technology, we analyzed the cost-effectiveness of the two surgical methods. With a detailed analysis of the available clinical data, we expect to provide valuable reference and guidance for future clinical practice.
Materials and methods
General information
This study entailed a retrospective analysis of clinical data from patients diagnosed with upper urinary tract calculi who underwent flexible ureteroscopy (FURL) at a tertiary hospital in Beijing from March 2023 to March 2024. The patients were categorized into two groups based on the surgical instruments used for the treatment: one group was treated with a disposable bendable negative pressure suction sheath (negative pressure group) and the other with a conventional ureteral access sheath paired with a lassoed mesh basket (conventional group). This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024. All patient details had been deidentified to ensure patient privacy and confidentiality.
Inclusion criteria
The study included patients aged 18 years or older, who presented with unilateral or bilateral upper urinary tract calculi with a diameter of less than 2 cm, with the renal calculi located in the renal pelvis or calyces. Additionally, the present study included patients who had unsatisfactory outcomes with extracorporeal shockwave lithotripsy and patients who were otherwise ineligible for this treatment method.
Exclusion criteria
Exclusion criteria included the presence of structural renal abnormalities such as renal hypoplasia or significant anatomical variants, severe urethral or ureteral stenosis, significant coagulation disorders, severe cardiopulmonary dysfunction precluding surgical intervention, and an inadequately managed positive urine culture.
Extensive clinical data were extracted from the hospital’s electronic medical record system, encompassing detailed records of patients’ basic information, presurgical and postsurgical examination results, surgical procedure documentation, postsurgical recovery, and follow-up data (Table 1).
General characteristics of the patients.
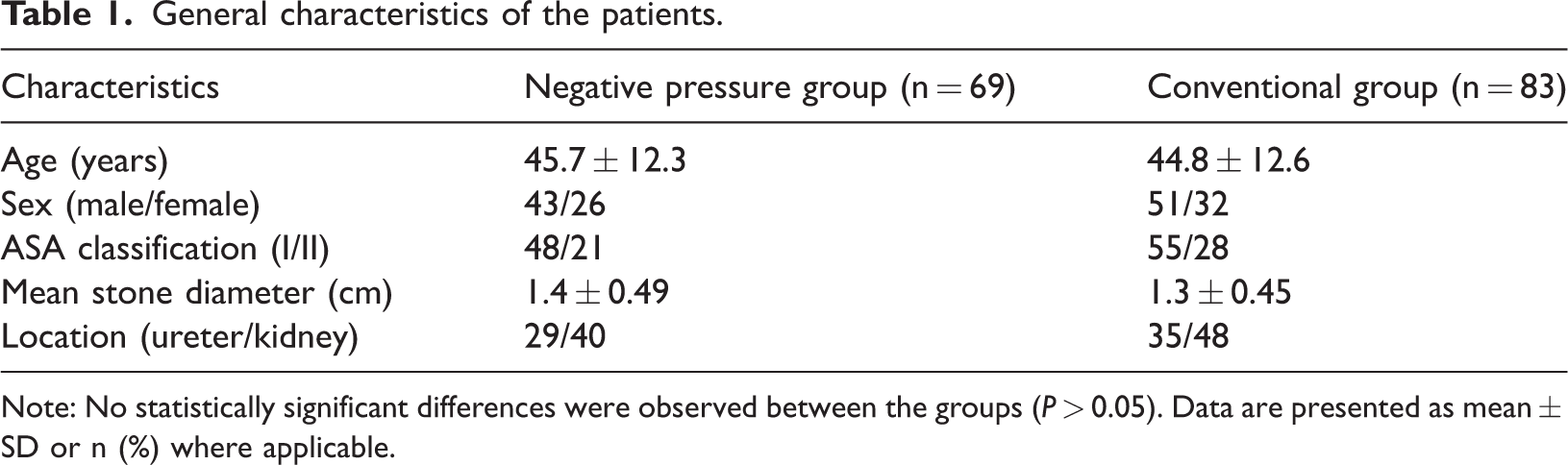
Note: No statistically significant differences were observed between the groups (P > 0.05). Data are presented as mean ± SD or n (%) where applicable.
Surgical methods
The surgical procedures within this study were conducted under general anesthesia, with patients positioned in lithotomy. An 8/9.8-F ureteral rigid scope was initially used for exploratory purposes, and upon confirmation of the stone’s location, a safety guidewire was inserted and left in situ. For upper ureteral calculi, pneumatic ballistic or holmium laser energy was applied to achieve fragmentation and facilitate the movement of stone fragments into the renal pelvis.
Negative pressure group
Following the initial probing, an ureteroscopy sheath with 10/12-F specifications (manufactured by Zhejiang Medical Gao Medical Technology Co., Ltd; approval number: 20212020030) was advanced along the guidewire to the upper ureter (Figure 1). Subsequently, a Zebra disposable ureteral flexible scope, with an outer diameter of 8.6 F (produced by Anhui Happy Workshop Medical Equipment Co., Ltd.), was introduced. A holmium 200-μm laser fiber, set at 1.5 J energy and a 20–25 Hz frequency, was used for lithotripsy. During lithotripsy, the sheath was carefully adjusted to remain close to the treatment area, and the negative pressure port in the sheath was actuated at precise moments to aspirate the fragmented material. A perfusion pump was calibrated to a pressure of 120 mmHg and a flow rate of 0.3 L/min to ensure continuous irrigation. The sheath’s outer end was connected to a stone collection receptacle, and the central negative pressure mechanism was set to a range of 150–200 mmHg. In instances where sizable stone fragments entered the sheath, the scope was carefully retracted while using negative pressure to facilitate the effective extraction of these fragments.

Bendable negative pressure suction sheath. (a) Diagram of the proximal end of the sheath with ureteral flexible scope. (b) Diagram of the distal end of the sheath and (c) whole view of the sheath with ureteral flexible scope.
Conventional group
As determined by the probe, a sheath of 10/12-F dimensions was navigated along the guidewire and then fixed at an appropriate location. Subsequently, the flexible ureteroscope was reinserted, and lithotripsy was executed using power settings similar to those applied with the holmium laser. For stone fragments exceeding 2 mm in diameter, extraction was attempted using a lassoed mesh basket. Double-J stents were uniformly placed following the procedure in both the cohorts to prevent postoperative stricture or stone fragment displacement. At the 1-week and 1-month postoperative junctures, patients underwent urological computed tomography (CT), and upon confirmation of the absence of residual calculi, the double-J stents were removed from the patients. Furthermore, operational metrics such as procedure duration, intraoperative bleeding, postoperative hospitalization length, and incidence of postoperative complications were carefully documented, which provided a foundation for evaluating the efficacy and safety of the procedure.
Assessment parameters
The efficacy and safety evaluation of the study was based on a meticulous assessment of predefined parameters. The operative time, a critical metric, was measured from the insertion of the ureteral rigid scope into the ureter to the successful placement of the double-J stent. Postoperative hemoglobin levels were analyzed to estimate intraoperative bleeding. The SFR was determined via urological CT at 1 and 4 weeks postoperatively, with its clinical significance attributed to the presence of residual stones exceeding 4 mm. The Clavien classification system was used to assess the severity of any postoperative complications. The duration of postoperative hospital stay was recorded, and discharge protocols relied on the absence of gross hematuria and resolution of complications. The hospitalization costs, including surgical, pharmaceutical, and accommodation expenses, were exhaustively documented.
Statistical analysis
For statistical analyses, SPSS 23.0 software was used to analyze the data. Continuous variables with a normal distribution were presented as mean (x) ± SD, and independent samples t-tests were performed for group comparisons. Categorical data were evaluated using the chi-square test. A p-value of <0.05 denoted statistical significance, thereby supporting the study’s analytical rigor.
Results
Postoperative analysis demonstrated that the negative pressure group significantly differed from the conventional group in terms of the operative time, hospitalization cost, hemoglobin drop values, and the number of cases with SFR at 1 week postoperatively (p < 0.05). Particularly, the mean operative times in the negative pressure group and conventional group were 119.8 and 93.2 min, respectively. In terms of hospitalization cost, the mean costs in the negative pressure group and conventional group were ¥28,273 and ¥30,786, respectively. The postoperative hemoglobin drop values averaged 5.3 g/L in the negative pressure group and 4.7 g/L in the conventional group. However, the postoperative hospital stay was not significantly different between the two groups (p = 0.3993), averaging 4.3 days in the negative pressure group versus 4.4 days in the conventional group. The SFR at 1 week postoperatively was 84.1% (58/69) in the negative pressure group and 68.7% (57/83) in the conventional group, exhibiting a higher rate of stone clearance in the former group. However, the SFR at 1 month postoperatively was 87.0% (60/69) in the negative pressure group and 84.3% (70/83) in the conventional group, with no statistically significant difference between the two groups (p = 0.1029). In terms of complications, there were five cases in the negative pressure group and eight in the conventional group, although the complication rates were not significantly different between the two groups (Table 2).
Comparison of intraoperative and postoperative outcomes between the groups.

Data are presented as mean ± SD or n (%) where applicable.
SFR: stone-free rate.
Discussion
With the increasing incidence of urinary stones, minimally invasive treatments are gradually replacing traditional open and laparoscopic surgeries. FURL has made the leap from artificial to natural channels and is considered a safer and less invasive procedure for treating upper urinary tract stones.8–10 Conventional ureteral access sheath lithotripsy, although minimally invasive, has several limitations. 11 First, during lithotripsy, continuous irrigation is essential to maintain a clear field of vision, and poor drainage can increase internal pressure, potentially increasing the risk of postoperative infection if the safety threshold is exceeded. 12 Second, larger stones require longer operation time. The “blizzard” phenomenon during lithotripsy affects the field of view, and the accumulation of stone fragments may affect the accurate judgment of lithotripsy efficacy, potentially resulting in an inadequate procedure. 13 Although conventional ureteral access sheath lithotripsy often applies a mesh basket to improve the SFR, it may also increase the cost of treatment. 14 Additionally, this procedure may necessitate more personnel and longer operation time, thereby increasing the invisible labor cost. 15
The bendable negative pressure suction sheath is an innovative medical device that, through its unique design, demonstrates significant advantages in retrograde intrarenal surgery. The distal end of this sheath can bend passively in response to the curvature of the flexible ureteroscope, allowing for more efficient access to the target calyces during the procedure, particularly for stones in the lower calyces.16–18
The significantly higher early SFR at 1 week postoperatively in the negative pressure group than in the conventional group (84.1% vs. 68.7%) is the most notable finding of our study, which can be attributed to several technical advantages of the negative pressure system. First, the active suction mechanism facilitates the immediate removal of stone fragments during lithotripsy, which reduces the likelihood of residual fragments migrating to less accessible locations within the collecting system. Second, the bendable nature of the sheath enables better access to various calyceal angles, potentially allowing for comprehensive stone clearance. However, it is noteworthy that this advantage diminished when both groups exhibited comparable SFRs (87.0% vs. 84.3%) after the 1-month follow-up. This convergence suggests that although the negative pressure system accelerates stone clearance, it may not significantly influence the ultimate treatment outcome.
It should be noted that the SFR in our study may appear lower than those reported in some published series, which can be explained by several factors. First, we used a strict definition of stone-free status, as confirmed using CT, where residual fragments >4 mm were considered as a treatment failure; on the contrary, some studies used less stringent criteria. Second, our study included stones in challenging locations, particularly lower pole calyces, which are known to have lower clearance rates. Therefore, these methodological differences should be considered when comparing our results with those of other studies.
The longer operative time observed in the negative pressure group (119.8 ± 10.4 vs. 93.2 ± 9.8 min) warrants careful consideration, which may be attributed to several factors. First, the manipulation of the bendable sheath and coordination with the suction system requires additional technical expertise and time. Second, the need to frequently adjust the position of the sheath for optimal suction effect may contribute to the extended operative duration. Although the longer operative time might be viewed as a disadvantage, it should be weighed against the benefit of improved early stone clearance and potentially reduced need for secondary procedures.
The slightly higher postoperative hemoglobin drop in the negative pressure group (5.3 ± 2.2 vs. 4.7 ± 1.2 g/L) suggested a marginally increased risk of bleeding, which may be attributed to several mechanisms. The negative pressure system might cause more trauma to the urothelium because of the suction effect, and the frequent repositioning of the bendable sheath could cause more mucosal injury. However, it is important to note that the difference, although statistically significant, may not be clinically meaningful as neither group showed severe bleeding complications.
We also observed that the hospitalization cost was lower in the negative pressure group (¥28,273 ± 5389 vs. ¥30,786.1 ± 4055). The price of the bendable sheath was comparable to that of a conventional ureteral access sheath, with no additional cost. The intraoperative need for the sheath basket only in specific situations reduces its frequency of use, thereby reducing hospitalization costs.
When comparing our technique with mini percutaneous nephrolithotripsy (PCNL), it is important to consider several key factors. Mini PCNL typically offers higher SFRs for larger stones (>2 cm), although with potentially higher morbidity. Studies have reported transfusion rates of 2%–7% for mini PCNL, with longer hospital stays compared with those required for FURL.19,20 Our negative pressure technology offers advantages in terms of reduced invasiveness, using the natural urinary tract without percutaneous access. Although mini PCNL may have shorter operative times for larger stone burdens, the choice between modalities should be individualized based on stone characteristics, patient factors, and available expertise.21,22 Direct comparative studies of these approaches are needed to clearly define the optimal treatment algorithm.
The comparable postoperative hospital stay (4.3 vs. 4.4 days) and complication rates between the two groups suggested that the negative pressure system does not compromise the safety or recovery time of the patient. This information is crucial for clinical decision-making, as it suggests that the potential benefits of the system are not associated with increased patient morbidity.
Several technical considerations emerge from our findings. The successful implementation of the negative pressure system requires specific surgical expertise, as suggested by the longer operative time. This indicates a learning curve that should be considered when adopting this technology. The recommendation for experienced operators to perform these procedures is particularly pertinent, given the technical demands of coordinating the bendable sheath with the suction system while maintaining optimal visualization.
The study’s findings must be interpreted within the context of certain limitations. First, the retrospective nature of the analysis may introduce selection bias, particularly given our exclusion of patients with significant coagulation disorders. This exclusion was primarily related to institutional protocol during the study period and the need to ensure patient safety when introducing a new technology. However, we acknowledge that FURS is indeed advantageous for patients with coagulopathies compared with percutaneous procedures, and this exclusion may have resulted in selection bias that limits the generalizability of our findings. Therefore, future studies should include patients with coagulopathies to better demonstrate the advantages of this minimally invasive approach. Second, the single-center design might limit the generalizability of our findings to other clinical settings with different patient populations or surgical expertise levels. Our results may not be applicable to all clinical environments, highlighting the need for multicenter validation. Third, our sample size of 152 patients (69 in the negative pressure group and 83 in the conventional group) represents an initial experience with this technology. Although our complication rates were comparable between the two groups, these findings require validation in larger cohorts to ensure adequate power for detecting differences in safety outcomes. Fourth, our follow-up protocol using CT at 1 week and 1 month postoperatively raises concerns about radiation exposure. Although low-dose CT protocols were used when available, alternative imaging modalities such as ultrasound combined with plain radiography could be considered to reduce radiation exposure. Future studies should explore radiation-reducing imaging protocols while maintaining accurate assessment of stone clearance. Finally, the follow-up period of 1 month, while sufficient for immediate outcomes, may not capture long-term complications or stone recurrence rates. The reporting of this study conforms to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 23
Conclusions
Our findings suggest that the bendable negative pressure suction sheath combined with a disposable ureteroscope represents a promising advancement in the treatment of upper urinary tract stones. Although the procedure demands a greater technical expertise and longer operative times, the benefits of improved early stone clearance and potential cost-effectiveness make it an attractive option for appropriately selected cases. However, the importance of operator experience and proper patient selection cannot be overstated. Given the limitations of our single-center retrospective study with a relatively small sample size, we recommend larger multicenter prospective studies to validate these findings and establish the true efficacy and safety profile of this technology. Future research should also include direct comparative studies with other modalities such as mini PCNL to better define the optimal treatment algorithm for different stone characteristics and locations. Additionally, studies incorporating patients with coagulopathies and using radiation-reducing imaging protocols would provide more comprehensive evidence for the role of this technology in contemporary stone management. These findings contribute to the evolving body of evidence supporting technological innovations in endourological surgery while highlighting the need for careful consideration of both technical and economic factors in their implementation.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251386570 - Supplemental material for A novel bendable suction sheath in flexible ureteroscopy for renal calculi
Supplemental material, sj-pdf-1-imr-10.1177_03000605251386570 for A novel bendable suction sheath in flexible ureteroscopy for renal calculi by Jiyu Zhao, Jiajing Wang, Sheng Yang, Jia Liu, Junzhe Xia, Xianen Gu and Jianhua Long in Journal of International Medical Research
Footnotes
Acknowledgments
No acknowledgments.
Author contributions
Conceptualization, Jiyu Zhao; methodology, Jiyu Zhao; formal analysis, Jianhua Long; investigation, Jiajing Wang, Sheng Yang, Jia Liu, Junzhe Xia; resources, Xianen Gu; data curation, Jiyu Zhao; writing—original draft preparation, Jiyu Zhao; writing—review and editing, Jiyu Zhao; visualization, Jiyu Zhao; supervision, Jianhua Long. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The datasets used or analyzed during the current study will be available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Institutional review board statement
All data included in this study are retrospective, and all patient privacy data involved in the study have been anonymized, thus involving no ethical review and approval.
Funding
This research received no external funding
Informed consent statement
Patient consent was waived for this study due to the fact that all data used were retrospective and that all patient privacy data involved were anonymized, ensuring the protection of individual privacy.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.