
Abstract
Objective
Stone disease is one of the most common afflictions in modern society. Complications following retrograde intrarenal surgery (RIRS) vary considerably, and small-diameter ureteral access sheaths are reportedly significantly associated with rates of infectious complications following RIRS. This study aimed to explore additional risk factors for infectious complications after RIRS.
Methods
This study retrospectively analyzed 602 patients who underwent RIRS between December 2016 and October 2019 at the First Affiliated Hospital of Fujian Medical University. All flexible ureteroscopic lithotripsy processes were conducted with patients under general anesthesia in the low lithotomy position. Postoperative systemic inflammatory response syndrome (SIRS) was diagnosed; statistical analyses comprised two-way analysis of variance (ANOVA) and one-way multivariate ANOVA.
Results
The incidence of infectious complications after RIRS was 7.14%. Operative time was an independent risk factor that increased the risk of infection. Stone size >2 cm was observed in 153 (27.37%) patients in the SIRS group and 29 patients (67.44%) in the non-SIRS group.
Conclusions
Findings in the literature suggest that early antibiotic treatment and active fluid therapy might lower the rate of infectious complications after RIRS. Our results indicate that extended operative time and increased stone size may be risk factors for infectious complications after RIRS.
Keywords
Introduction
Stone disease is among the most common afflictions in modern society. The lifetime prevalence of kidney stone disease is estimated to range from 1% to 15%, with variations according to age, sex, race, and geographic location. 1 A popular approach for the management of small or mid-sized renal stones is retrograde intrarenal surgery (RIRS), which is regarded as a first-line alternate surgery for percutaneous nephrolithotomy; this method was first introduced by Marshall in 1964 and has become the primary treatment option for renal stones up to 20 mm in size. 2 Using an 8-Fr (1 Fr = 0.33 mm) soft mirror to complete ureteral and renal examination, Takagi et al. 3 initiated the clinical application of RIRS. In the context of continuous equipment updates, increasing flexibility, and smaller-diameter ureteral access sheaths, digital ureteroscopy has become the standard treatment approach for ureteral and renal stones. 4
Flexible ureteroscopy has been gradually implemented in various types of hospitals worldwide. However, a variety of complications have been reported following RIRS, including hematuria, pain, fever, infection, sepsis, kidney loss, and mortality. 3 Notably, the incidence of systemic inflammatory response syndrome (SIRS) during percutaneous nephrolithotomy ranges from 16.7% to 23.4%; 5 SIRS risk factors after percutaneous nephrolithotomy have been well-characterized in previous investigations. 6 , 7 To the best of our knowledge, SIRS risk factors after RIRS have not been fully elucidated, although infection remains a serious postoperative complication after RIRS, with a reported incidence approaching 25%. 5 The risk factors for infectious complications after RIRS remain controversial. Previous investigations have demonstrated that large stone burden, small-diameter ureteral access sheath (UAS), and irrigation with a high flow rate are significantly associated with increasing rates of infectious complications following RIRS. 8 Although preoperative antibiotic therapy and the use of UAS can reduce the likelihood of pyelolymphatic or pyelovenous backflow, patients may exhibit unpredictable postoperative systemic infection after RIRS; this may become catastrophic in some instances. This retrospective study aimed to explore additional risk factors for infectious complications after RIRS.
Materials and methods
Patients
This retrospective study included patients who underwent RIRS between December 2016 and October 2019 at the First Affiliated Hospital of Fujian Medical University, Fujian, China. The exclusion criteria were: (1) severe cardiac insufficiency; (2) late-stage kidney disease; (3) refusal to undergo surgery. The Ethics Committee of the First Affiliated Hospital of Fujian Medical University (Fujian, China) approved this study (approval no. IEC-FOM-013-1.0s). All patient details were de-identified and all patients provided written informed consent to participate in the study.
Medical history, serum electrolytes, midstream urine culture, urinalysis, serum creatinine, complete blood count, and coagulation assessments were performed preoperatively. Plain abdominal film and ultrasonography examinations were also performed. Intravenous urography was performed if a patient’s serum creatinine level was in the normal range. Patients underwent non-contrast helical computed tomography scans to evaluate stone characteristics. Patients with preoperative positive urine culture results received a complete course of culture-specific antibiotics, prior to RIRS procedures. Prophylactic antibiotic treatment with ciprofloxacin (cephalosporin for patients with abnormal renal function) was administered to all patients prior to surgery.
Flexible ureteroscopic lithotripsy procedure
Flexible ureteroscopic lithotripsy procedures were performed with patients under general anesthesia in the low lithotomy position. Ureteroscopy was performed using a semi-rigid 8/9.8-Fr ureteroscope (Richard Wolf, Knittlingen, Germany), with a flexible 0.035-inch guide wire inserted into the renal collecting system. A UAS (Cook Medical, Bloomington, IN, USA) was then inserted into the proximal ureter along the guide wire under fluoroscopy guidance. A flexible ureteroscope (Olympus, Tokyo, Japan) was then advanced through the UAS. Stones were identified and fragmented by holmium:yttrium-aluminum garnet laser lithotripsy. Stone fragments were removed using a 2.2-Fr Nitinol stone basket. A 6-Fr double-J ureteral stent was placed at the completion of surgery.
SIRS vs. non-SIRS groups
The primary endpoint of the study was the incidence of postoperative SIRS, defined as onset within 2 weeks after RIRS. Patients were diagnosed with SIRS if they exhibited at least two of the following four criteria: 9 (1) body temperature >38°C or <36°C; (2) respiratory rate >20 breaths/minute or partial pressure of carbon dioxide <32 mmHg (<4.3 kPa), at least 12 hours after surgery; (3) heart rate >90 beats/minute, at least 12 hours after surgery; (4) leukocyte count >12,000 cells/mm3 or <4,000 cells/mm3. Patients who did not meet these criteria were included in the non-SIRS group.
Statistical analysis
Univariable analysis (two-way analysis of variance) and multivariable analysis (one-way multivariate analysis of variance) were performed using IBM SPSS Statistics, version 25 (IBM Corp., Armonk, NY, USA). The SIRS and non-SIRS groups were compared to comprehensively assess risk factors for SIRS. p values <0.05 were considered to indicate statistical significance.
Results
Patient characteristics
This study included 602 patients who underwent RIRS at our hospital. Forty-three patients (7.14%.) underwent SIRS (Figure 1, Table 1). The rate of infectious complications was higher among male patients (7.55%) than among female patients (6.69%), although this difference was not statistically significant. The rate of infectious complications after RIRS was 10.58%. There was no statistically significant difference in the proportion of patients with stone location in the left or right kidney between the two groups (Table 1). Preoperative urine cultures results exhibited 50% sensitivity and 63% specificity in this study.

Computed tomography scans of a patient with medullary sponge kidney. (a) A high preoperative stone burden was observed, and the operative time was 81 minutes. (b) The patient developed systemic inflammatory response syndrome postoperatively.
Patient characteristics, clinical findings, and prognostic analyses (numbers in brackets are percentile).

Data are shown as mean ± standard deviation or number of patients (%).
*: Bold values indicate p < 0.05 for association with SIRS.
BMI, body mass index; SIRS, systemic inflammatory response syndrome.
Associations with onset of SIRS
The non-SIRS and SIRS groups did not significantly differ in terms of age, body mass index, history of urinary calculi in the affected side, or preoperative creatinine abnormality (Table 1). However, preoperative positive urine culture results, operative time, and stone size >20 mm were significantly associated with the onset of SIRS (p = 0.040, p = 0.009, and p = 0.001, respectively).
Logistic regression analysis revealed that patients with longer operative time (Figure 2) and stone size >20 mm were more likely to have SIRS (p = 0.009 and p < 0.001, respectively; Table 2). Multivariate analyses confirmed that operative time and stone size >20 mm were independent risk factors for increased risk of infection (p = 0.014 and p < 0.001, respectively).
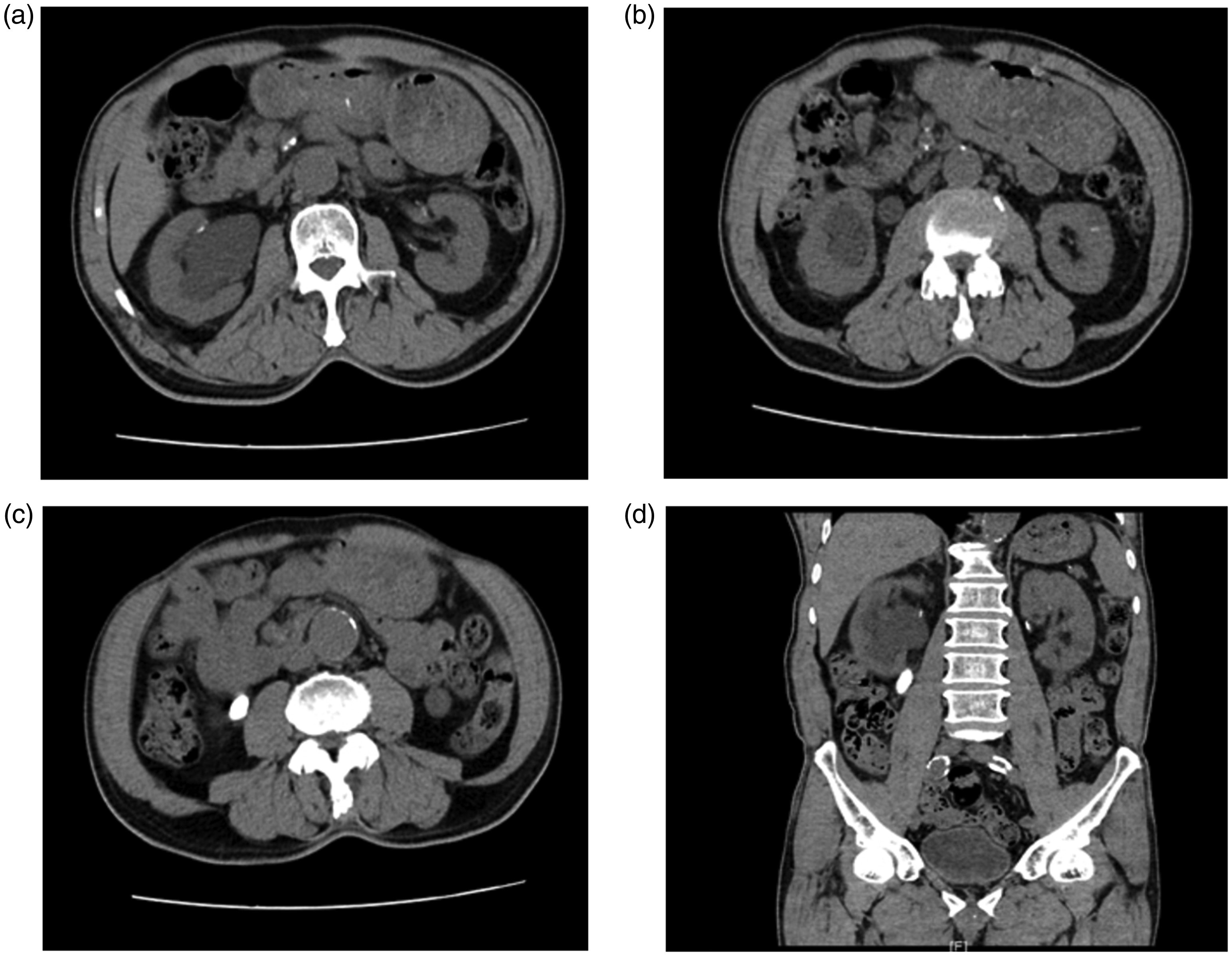
Computed tomography scans of a patient with a history of right low back pain with fever for 2 days. Preoperative urine culture results were positive, and the patient developed systemic inflammatory response syndrome postoperatively.
Logistic regression analysis of infectious complications after retrograde intrarenal surgery.
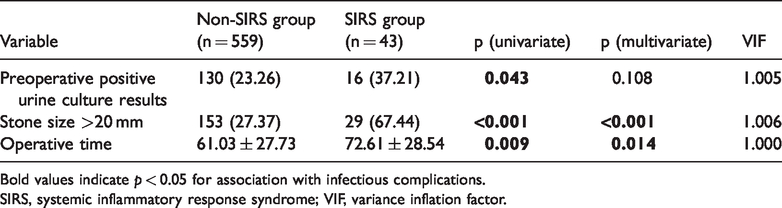
Bold values indicate p < 0.05 for association with infectious complications.
SIRS, systemic inflammatory response syndrome; VIF, variance inflation factor.
Discussion
Complications after RIRS are common, with infectious complications being the most serious problem among patients undergoing stone removal treatment. The incidence of infectious complications after RIRS is reportedly 1.7% to 18.8%; 10 in the current analysis, this rate was 10.58%. As reported by Fan et al., 11 because RIRS is an endourologic procedure with some similarities to percutaneous nephrolithotomy, RIRS has comparable risk factors for postoperative SIRS. Zhong et al. 8 reported that large stone burden, presence of infectious stones, small-diameter UAS, and irrigation with a high flow rate were independent risk factors for SIRS after RIRS. Moreover, Orsan Demir et al. 12 reported that operative time was an independent risk factor for postoperative urinary tract infection in patients who underwent RIRS. A recent study 13 demonstrated that the extent of intraoperative pyuria was associated with the rate of infectious complications following RIRS.
In the present study, we found that the rate of infectious complications was lower than that of the study by Orsan Demir et al. 12 We presume that this difference was observed because patients who underwent rigid ureteroscopy were also included in the CROES study, 14 which might have reduced the rate of infection. Furthermore, our findings showed a lower incidence of infection than in the study by Baboudjian et al., which involved flexible ureteroscopy. 15 Notably, the incidence of SIRS occurred at a rate of 8.1% in another study of flexible ureteroscopic lithotripsy. 8 A recent systematic review showed that the use of single-dose prophylactic antibiotics was able to reduce the incidences of postoperative pyuria and bacteriuria, although this approach did not significantly reduce the incidence of postoperative urinary tract infections. 16 The findings in the literature suggest that early antibiotic treatment and active fluid therapy might lower the rate of infectious complications after RIRS.
A previous study revealed that operative time was an important risk factor for postoperative fever in patients undergoing stone removal. 17 In addition, stone size has been associated with postoperative infection after RIRS; greater stone size had the strongest influence on the extension of operative time. 18 Prolonged operative time is a reported risk factor for postoperative fever. In previous studies of RIRS, the operative time was reported to be 60 to 120 minutes, although it is commonly accepted that the duration of the intervention should not exceed 1 hour. 17 The operative time in our study was similar to the operative time in previous investigations; moreover, operative time was an independent risk factor that increased the risk of infection. In a study of 266 patients performed by Sorokin et al., 18 more infections were observed with operative time >70 minutes, which was similar to the operative time for patients with SIRS in the present study. However, our study included a larger number of patients, so the results may be more generalizable to other patient populations. Although a safe operative time has not been determined thus far, the current findings and prior research indicate that extended duration of RIRS is a risk factor for postoperative fever/infection.
Stone size has been reported to influence postoperative septic shock in patients undergoing stone removal. 10 , 19 In our study, larger stone size was a significant risk factor for SIRS. Larger stone size is often presumed to be associated with greater likelihood of infectious stones, thereby resulting in bacteriuria; these large stones may also carry a greater endotoxin load. 6 Concurrent large stone burden and long operative time may cause exposure to large amounts of endotoxin. The operative time should be strictly controlled for patients with high risk of SIRS, which requires the use of staging procedures. In our experience, shorter operative time is associated with lower renal pelvic pressure and lower incidence of postoperative inflammation.
Prior studies have shown that a history of stone surgery and the presence of lower pole stones are both risk factors for infective complications. 9 However, a prior study demonstrated that a history of previous surgery was not a risk factor for infectious complications after stone removal. 11 Notably, our analysis revealed that the presence of lower pole stones and a history of previous surgery were not risk factors for infective complications. The higher incidence of infectious complications in our patients, compared with patients in the study by Fan et al., 11 may be related to differences in inclusion criteria (e.g., characteristics of the patients, use of antibiotics, or definitions of infectious complications). Most patients in the present study received antipyretics, without changes in antibiotic treatment. This treatment approach is consistent with the methodology in a prior study concerning operative complications after RIRS. 18 Importantly, postoperative fever may occur despite the presence of sterile preoperative urine and appropriate antibiotic prophylaxis. The European Association of Urology guidelines suggests that short-term antibiotic prophylaxis be administered to patients with RIRS who exhibit sterile urine. For patients with positive urine culture results, antibiotic therapy should be administered before the stone removal procedure, then continued for at least 4 days postoperatively. 18 Preoperative urine culture results have been used to predict the onset of postoperative infectious complications; positive preoperative urine culture results are associated with increased risk of postoperative fever. 18 In the current study, multivariate analysis showed that the preoperative urine culture rate did not significantly differ between the two groups. Preoperative urine cultures have only 50% sensitivity and 63% specificity (as demonstrated in the present study). These characteristics of the test method may explain why the urine culture results did not constitute an independent risk factor for infectious complications in this study.
RIRS is more effective than percutaneous nephroscopy in the treatment of stones through natural channels (i.e., from the urethra through the bladder, then into the ureter and kidney). 20 It is minimally invasive, and equally safe and effective, compared with percutaneous nephroscopy. Antibiotics are often needed before patients undergo RIRS. However, in some instances, the kidney collection system may be in a high-pressure state for an extended period, such that the infected urine may flow backwards or leak into the perirenal tissue space, leading to the spread of infection and the occurrence of sepsis. Situations that may cause these outcomes include:20,21 1) ureteral stricture and distortion, such that the flexible ureteroscope sheath cannot enter the renal pelvis; 2) ureteral injury and urine extravasation; 3) serious stone obstruction, with infection of the upper portion of the obstruction, which cannot be detected by a routine urine test and therefore cannot be completely controlled by preoperative antibiotic treatment; 4) intraoperative hemorrhage, unclear vision, and/or artificial enhancement of perfusion pressure and flow; 21 5) treatment of stones with diameter >2.5 cm and/or long operative time. The retention of a double-J tube for more than 1 week before surgery is conducive to the placement of a ureteroscopic sheath into the renal pelvis during the operation; 22 for larger stones, pretreatment of micro fistulas in the renal collecting system is also helpful for lowering intraoperative pressure in the renal pelvis and reducing the incidence of infection. 23 During postoperative recovery, vigilance is necessary to identify early symptoms and signs of infection, thus allowing early diagnosis and treatment.
Because renal calculi constitute a common urological disease, there is increasing technology available to aid in minimally invasive surgery. RIRS plays an increasingly important role in the treatment of renal calculi. In the future, equipment renewal should be focused on improving the operation efficiency and reducing damage to the body. The following aspects should be considered: the patient's situation, the hospital equipment situation, the doctor's experience with a particular treatment approach, and the use of evidence-based medicine. With respect to infectious complications, prevention efforts should be prioritized; early treatment may prevent further progression of the infection. 22 Urologists should understand the advantages and disadvantages of various surgical instruments; they should also seek to improve their theoretical knowledge and surgical expertise, which may reduce the likelihood of complications and improve the stone clearance rate. 23 There were some limitations in our study. A notable limitation was the small proportion of patients who experienced SIRS, which may have led to some bias and restricted the generalizability of the findings.
Conclusions
Large stone size, positive urine culture results, and long operative time were significantly associated with the risk of SIRS after RIRS for kidney stones. These findings could assist clinicians in evaluating the risk of infectious complications after RIRS.
Footnotes
Author contributions
HM conceived the study. HZ, TJ, RG, QC, WC, CL, and HM performed the analysis and wrote the manuscript.
Acknowledgements
The authors would like to thank the editor and anonymous reviewers who provided insights and valuable suggestions that helped to improve this work.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
“This work was supported by the Qihang Fund of Fujian Medical University (2019QH1078).