
Abstract
Objective
To evaluate the effectiveness and safety of flexible ureteroscopy in the treatment of kidney and upper ureteral calculi under double-J stent free mode.
Methods
Data from patients who underwent flexible ureteroscopy and laser lithotripsy between February 2018 and September 2021 were retrospectively and analysed. Cases were grouped according to pre- or postoperative use of the double-J stent (6 Fr): Post-F group (preoperative double-J stent but no postoperative double-J stent); Pre-F group (no preoperative stenting but with postoperative double-J stent); and Routine group (preoperative and postoperative double-J stenting).
Results
A total of 554 patients (390 male and 164 female) were included. The mean operation time was similar between the three groups, with no statistically significant difference. Incidence of grade 0–1 ureteral injury was significantly higher in the Pre-F group versus other groups, but there were no significant between-group differences in other operation-related complications. During follow-up, stent-associated complications were observed in the Pre-F and Routine groups, but not in the Post-F group. Stone clearance rates were similar between all groups at 1, 3 and 6 months following surgery.
Conclusions
Flexible ureteroscopy using double-J stent free mode was found to be safe, feasible and effective in treating renal and upper ureteral calculi.
Keywords
Introduction
At present, minimally invasive techniques are the main surgical treatment for urinary calculi, including retrograde ureteroscopic lithotripsy, percutaneous nephrolithotomy and laparoscopic techniques. Based on high efficacy and low complication rates, the European Association of Urology (EAU) guidelines recommend flexible ureteroscopy (fURS) as one of the main methods for treating kidney and upper ureteral stones of less than 20 mm. 1
Routine preoperative stenting before fURS for passive dilation of the ureter is no longer part of the standardized technology,2,3 however, EAU guidelines still recommended pre-stenting to improve the outcome. 1 Because preoperative stenting before fURS may improve stone clearance rate and reduce the rate of complications, such as ureteric injury,3–7 many surgeons still adopt this approach before fURS. Generally speaking, the routine operating procedure for fURS and laser lithotripsy consists of three steps. First, under cystoscopy, a double-J stent is placed in the ureter of the stone side prior to ureteroscopy. A few days later, fURS is performed, simultaneously replacing the previous double-J stent with a new one. Finally, the double-J stent is removed by cystoscopy after an appropriate time interval following surgery. Some patients may experience stent-associated complications, such as fever, haematuria, pain, frequent urination, urgency, and dysuria while the double-J stent is in place. 8 With the practice of pre and post stenting, patients may experience such complications both before and after fURS. In order to reduce the duration of stent-associated symptoms, is it possible to adopt a stent free mode after surgery? Multicentre studies investigating a stent free mode following fURS are currently rare. Thus, the aim of the present study was to conduct a retrospective preliminary analysis of data from patients who had undergone fURS with varying double J stent-free modes (pre or postsurgical) at The Second Affiliated Hospital of Soochow University.
Patients and methods
Study population and study design
The clinical data of consecutive patients with upper ureteral calculi and renal calculi, who were treated by retrograde fURS and holmium laser lithotripsy at The Second Affiliated Hospital of Soochow University, between February 2018 and September 2021, were retrospectively analysed. Included patients were those with non-incarcerated upper ureteral calculi, 9 or renal calculi, who were successfully treated with unilateral, single fURS and holmium laser lithotripsy and in whose cases, the cumulative calculi maximum length diameter (CMD), measured by computed tomography (CT), was 10–20 mm. The CMD was calculated by measuring the maximum length diameter of the stone according to the CT 3D reconstruction images. The following cases were excluded from the study: patients with calculi complicated by ipsilateral ureteral stenosis, or pyonephrosis, or severe infection; patients with anatomical abnormalities of the kidney, including horseshoe kidney, medullary sponge kidney, duplex kidney, transplanted kidney, or ectopic kidney; and patients who had received radiotherapy for abdominal and pelvic tumours. Data regarding preoperative physical examination, urinalysis, urine culture, abdominal CT scan and urinary ultrasonography were extracted from medical records within the hospital database. The degree of hydronephrosis was judged by the results of ultrasonography. Hydronephrosis was classified into four types: no hydronephrosis, mild hydronephrosis, moderate hydronephrosis and severe hydronephrosis. Data regarding demographic characteristics and preoperative parameters were also extracted. Stones characteristics, such as the CMD and CT value of the calculi were also extracted for analysis. The mean CT values for calculi were calculated as the mean of three different areas of the largest cross-section of the calculi in the CT scan. Complications, including surgical complications and stent-associated complications, were graded retrospectively according to the modified Clavien-Dindo classification. 10
The reporting of this study conforms to STROBE guidelines. 11 All procedures were in accordance with ethical standards of The Second Affiliated Hospital of Soochow University Ethics Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards, and all patients provided written informed consent to treatment. The study was approved by the Ethics Committee of The Second Affiliated Hospital of Soochow University (JD-HG-2022-23), and the committee waived the requirement for informed consent to study inclusion because of the retrospective study design.
The grouping principle was as follows. Patients were informed of the operation process and whether the double-J stents were retained in the ureter before and/or after the operation. The postoperative double-J stent free (Post-F) group comprised patients with preoperative indwelling double-J stent (6 Fr) and no postoperative double-J stent. The routine group comprised patients with both preoperative double-J stenting (6 Fr) and postoperative double-J stenting (6 Fr). The duration of pre stenting with double-J stents in the Post-F and Routine groups was 2 weeks. The preoperative double-J stent free (Pre-F) group comprised patients without preoperative stenting and with indwelling postoperative double-J stent (6 Fr).
Surgical procedures
All procedures were performed by a deputy chief physician (BXX) with extensive experience in fURS. Patients were treated under general anaesthesia and in the pendulum lithotomy position. Under direct vision, a 9.5 Fr rigid ureteroscope was inserted from the external urethral orifice to the bladder. If the double-J stent was placed preoperatively, it was removed. Using a guide wire, a rigid ureteroscope was inserted into the ureter to the renal pelvis for routine examination. The fURS delivery sheath was inserted under guidance of the wire and a constant pressure perfusion pump was connected, or a hand-push syringe may have been used for perfusion. The Olympus URF-V2 electronic flexible ureteroscope was inserted into the renal pelvis through the fURS sheath, and the renal pelvis and all renal calyces were examined for calculi. The calculi were crushed to a diameter <4 mm using a 200-μm holmium laser fibre with laser energy and frequency set as follows: fragmentation mode, 1.2–1.5 J/15 Hz and pulverization mode, 0.8–1.0 J/20–25 Hz. During the operation, larger calculi fragments were removed with a stone retrieval basket. In the Post-F group, a 5 Fr ureteral catheter was temporarily placed in the ureter at the end of the operation and removed at 48–72 h after the operation. In the Pre-F group and the Routine group, a new 6 Fr double-J stent was placed in the ureter at the end of the operation and removed under cystoscopy at 1 month after the operation.
Postoperative procedures and follow-up
All patients were followed-up for 6 months. Abdominal CT scan, ultrasonography, or kidneys, ureters and bladder (KUB) radiography were performed at the end of 1, 3 and 6 months following the operation. All imaging data were compared with preoperative data. The absence of stone, or presence of stone fragments ≤2 mm in diameter, was regarded as complete stone clearance. Differences in demographic characteristics, preoperative parameters, stone characteristics, operative time, operative complications, double-J stent-associated complications, and stone free rate between the three treatment groups were compared.
Statistical analyses
Continuous data are presented as mean ± SD and were compared by one-way analysis of variance. Categorical variables are presented as n (%) prevalence and were compared using χ2-test or Fisher’s exact test. Data were analysed with IBM SPSS software, version 19.0 (IBM Corp, Armonk, NY, USA), and a P value <0.05 was considered to be statistically significant.
Results
The clinical data of 554 patients (390 male and 164 female) were included in this retrospective study, according to the inclusion and exclusion criteria. Patient age ranged from 23 to 78 years (mean, 48.7 ± 15.9 years) and body mass index ranged from 18.6 to 28.6 kg/m2 (mean, 24.0 ± 2.0 kg/m2). There were 73 cases of upper ureteral calculi and 481 cases of renal calculi. The cumulative calculi maximum length diameter (CMD) was 10–20 mm (15.9 ± 2.9 mm). The calculi CT value ranged from 476 to 1560 HU (mean, 1031.8 ± 595.6 HU).
As per the inclusion and exclusion criteria, 177 patients were included in the Pre-F group, of whom, 23 patients (13.0%) failed to have the fURS delivery sheath successfully placed during the operation, due to a small ureteral diameter. With informed patient consent, six cases were assigned to the Post-F group and 17 cases to the Routine group. There were no statistically significant differences in demographic or stone characteristics between the three groups (P > 0.05; Table 1).
Demographic and clinical characteristics of patients who underwent flexible ureteroscopy and laser lithotripsy, classified into three treatment groups.
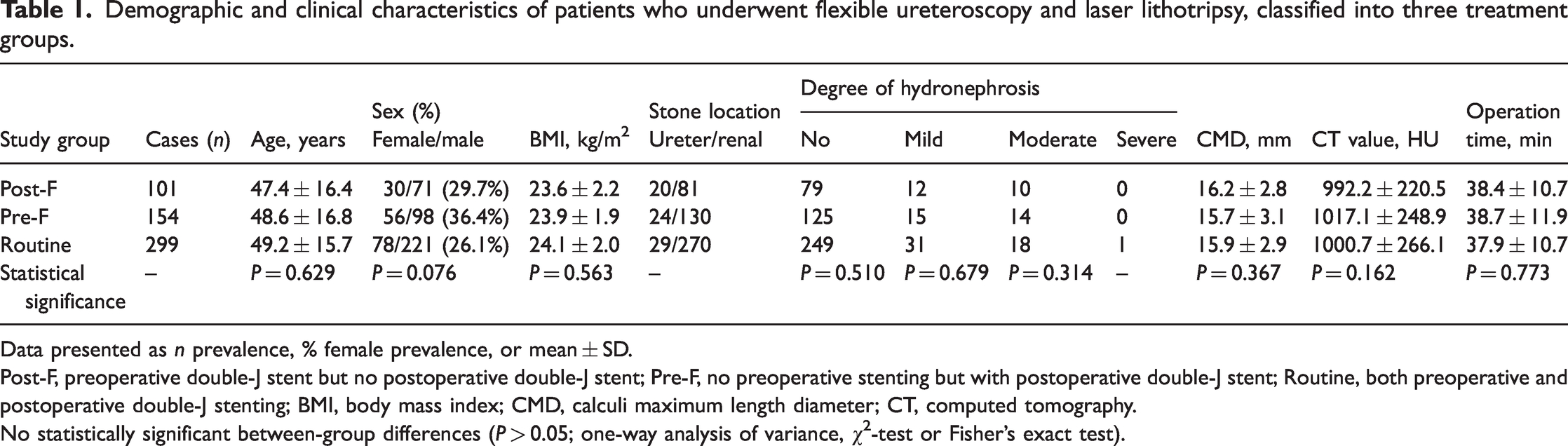
Data presented as n prevalence, % female prevalence, or mean ± SD.
Post-F, preoperative double-J stent but no postoperative double-J stent; Pre-F, no preoperative stenting but with postoperative double-J stent; Routine, both preoperative and postoperative double-J stenting; BMI, body mass index; CMD, calculi maximum length diameter; CT, computed tomography.
No statistically significant between-group differences (P > 0.05; one-way analysis of variance, χ2-test or Fisher’s exact test).
The mean operation times were not significantly different between the Post-F, Pre-F and Routine groups (38.4 ± 10.7 min, 38.7 ± 11.9 min and 37.9 ± 10.7 min, respectively; P > 0.05). Surgical and stent-associated complications are summarised in Table 2. In terms of surgical complications, the incidence of grade 0 and 1 ureteral mucosa injury was significantly higher in the Pre-F group than in the other two groups (P < 0.01), but there was no significant difference between the Post-F and Routine group (P > 0.05). Bleeding, renal subcapsular effusion and fever were the other most common Clavien-Dindo grade I/II complications, with no statistically significant differences between the three treatment groups (Table 2). There was also no significant difference in postoperative ureteral stenosis between the three groups (P > 0.05). None of the included patients developed urosepsis during or after surgery. In the Pre-F group, one patient was found with hydronephrosis at 3 months after the operation, and showed progressive aggravation. A membranous stricture of the upper ureter was found by ureteroscopy and cured by balloon dilatation.
Surgical and double-J stent-associated complications in 554 patients who had undergone flexible ureteroscopy and laser lithotripsy, classified into three treatment groups.

Data presented as n (%) incidence.
Post-F, preoperative double-J stent but no postoperative double-J stent; Pre-F, no preoperative stenting but with postoperative double-J stent; Routine, both preoperative and postoperative double-J stenting; UTI, urinary tract infection.
Statistically significant between-group differences (P < 0.05; χ2-test or Fisher’s exact test).
Regarding double-J stent-associated complications, the common Clavien-Dindo grade I/II complications were haematuria, bladder irritation symptoms, fever, pain and urinary tract infection. While there were no stent-associated complications in the Post-F group, the above complications frequently occurred in the other two groups, with no statistically significant between-group differences in incidence rates (P > 0.05; Table 2). All 554 patients were followed up for 1 month after the operation. At the 3-month time-point, 50 patients had been lost to follow-up, and data were obtained for 504 patients (91%). A total of 489 patients (88%) were assessed at the 6-month time-point. Stone free rates in the Post-F, Pre-F and Routine groups, respectively, were 88.1% versus 87.7% versus 89.6% at 1 month, 91.5% versus 91.9% versus 93.8% at 3 months, and 93.1% versus 93.0% versus 94.9% at 6 months (all P > 0.05; Table 3).
Follow-up stone free rate in 554 patients who had undergone flexible ureteroscopy and laser lithotripsy, classified into three treatment groups.

Data presented as n (%) incidence.
Post-F, preoperative double-J stent but no postoperative double-J stent; Pre-F, no preoperative stenting but with postoperative double-J stent; Routine, both preoperative and postoperative double-J stenting.
No statistically significant between-group differences (P > 0.05; χ2-test or Fisher’s exact test).
Discussion
Retrograde fURS is one of the main minimally invasive methods for treating upper urinary tract calculi. The safe, noninvasive and ease of manipulation characteristics of the fURS technique are favoured by surgeons and patients, and it may even be performed as day or outpatient surgery.12,13 With popularization of the electronic flexible ureteroscope, and application of the disposable electronic flexible ureteroscope,14–16 the clarity of surgical imaging has been improved, the learning curve has been shortened, and the cost has been reduced.
Preoperative stenting before fURS for passive dilatation of the ureter remains under debate, however, the results of published meta-analyses may strengthen the notion of preoperative stenting. In a review and analysis of 20 studies into the treatment of upper urinary tract urolithiasis using fURS, including 5 852 patients, 3 clinical outcomes displayed a high stone free rate and tendency for lower complications with pre-stenting. In a separate review of seven studies, including 3 145 patients (pre-stenting, 1 408; no pre-stenting, 1 737) who had undergone fURS for large upper urinary tract stones (≥10 mm), 16 pre-stenting was shown to improve initial success rate and provide better stone free rates. The ureteral access sheath may facilitate insertion and movement of the flexible ureteroscope inside the ureter, and may reduce intrarenal pressure and provide clearer vision. 17 Urosepsis-associated mortality is reported to be approximately 2.5-fold higher in patients with urinary obstruction, which may largely be due to urolithiasis.18,19 Use of a ureteral access sheath may help to reduce the risk of this complication,19,20 however, without pre-stenting, the failure rate of ureteral access sheath utilization may reach about 9.8–22.0%. 21 In the present study, the ureteral access sheath was used in all patients. The failure rate was 13.0% in the Pre-F group, which was close to previously reported values. Compared with the Post-F and Routine groups, the higher incidence of ureteral injury (Grade 0–1) complications observed in the Pre-F group may have been related to active intraoperative dilatation by the ureteral access sheath.
Despite reports showing that routine post-stenting is unnecessary after ureteroscopy in uncomplicated cases,22,23 in patients with ureteral injury or heavy stone burden, post-stenting remains essential. Short-term post-stenting using ureteral catheterization overnight in uncomplicated cases after fURS for kidney stone is shown to be as effective as conventional long-term post-stenting in reducing postoperative complications. 24 Short-term postoperative ureteral catheter indwelling (<6 h), or even total absence of double-J stent, has been shown to be feasible in retrograde ureteroscopy surgery (including fURS) through phase I and phase II clinical experiments,25,26 which has helped to improve the quality of life of patients and reduce complications. Multicentre studies of no-post-stenting after fURS are lacking. Therefore, clinical decision-making needs to combine the preoperative and intraoperative characteristics of individual cases. For the sake of safety, most surgeons prefer to indwell a double-J stent after the operation. However, the indwelling of a double-J stent often leads to accompanying symptoms, such as lumbar and abdominal pain, pubic pain, frequent urination, urgency of urination, urination pain, haematuria, sexual dysfunction, and even high fever. 8 These accompanying symptoms may seriously hinder the patient's rapid postoperative recovery and affect the patient's life quality by preventing normal social networking and work. Particularly for patients with both pre-stenting and post-stenting, the duration of stent-associated symptoms may be longer than in patients who have received either pre- or post-stenting. In the present study, the rate of surgical complications was not increased in the Post-F group compared with the other two groups, with similar stone clearance rates and no stent-associated complications. From the perspective of the patient’s postoperative life quality, it may be better not to use a ureteral stent after ureteroscopy laser lithotripsy. However, this may lead to other complications, such as acute ureteral obstruction and emergency placement of a ureteral stent. 27
The results of the present study may be limited by several factors. First, the data included in the study were mainly aimed at the postoperative stage without indwelling stent, and was limited by study sample size and follow-up duration. Secondly, because this was a single-centre retrospective study, the level of evidence was limited. A prospective, randomized controlled study is required to further support the present results.
In conclusion, the non-indwelling double-J stent mode after fURS for renal and upper ureteral calculi was feasible, safe and effective, and may avoid stent-associated complications and improve patients’ quality of life. In the present study, patients who were free of a postoperative double-J stent (the Post-F group), were those who had received pre-stenting. Whether this tubeless postoperative management mode may also be adopted in patients without preoperative stenting needs to be further explored.
Research Data
Research Data for The study of double-J stent free mode of flexible ureteroscopy and laser lithotripsy: a single centre experience
Research Data for The study of double-J stent free mode of flexible ureteroscopy and laser lithotripsy: a single centre experience by Ming Xu, Xiaoyun Han, Jin Zhu, Chuanyang Sun, Wei Tao and Boxin Xue in Journal of International Medical Research
Footnotes
Author contributions
Ming Xu: data collection and manuscript writing; Xiaoyun Han: data analysis and manuscript writing; Chuangyang Sun: project development; Jin Zhu: data collection; Wei Tao: data collection; and Boxin Xue: project development. All authors gave final approval of the version to be published.
Data accessibility statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported by the Suzhou Science and Technology Planed Project (grant No. SYS2020139 to Dr Ming Xu).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.