
Abstract
An esophageal fistula can be caused by an esophageal tumor as well as the surgery, radiotherapy (RT), or chemoradiotherapy used to treat the tumor. The most dangerous complications are massive hemoptysis and asphyxia. This report describes a 58-year-old man with a >1-month history of dysphagia and hemoptysis. Contrast-enhanced computed tomography revealed a tumor in the upper esophagus and a tracheoesophageal fistula. Esophagography revealed a large lesion measuring approximately 8 cm in length. Esophagogastroduodenoscopy showed an ulcerated tumor with raised margins originating 22 cm from the incisors, and histologic examination of a biopsy specimen indicated squamous cell carcinoma. The tumor was finally classified as stage IVA (T4bN0M0) esophageal squamous cell carcinoma. Massive hemoptysis occurred after the patient was admitted to the hospital. Therefore, we applied staged dose-escalated RT in three stages (6.0 Gy in 5 fractions, 7.5 Gy in 5 fractions, and 46.8 Gy in 26 fractions) to decrease the rate of tumor shrinkage brought on by RT and give the normal tissue enough time to close the fistula. Finally, the hemoptysis resolved and the patient’s symptoms were significantly improved. Contrast-enhanced chest computed tomography revealed shrinkage of the tumor. In conclusion, staged dose-escalated RT can be applied for esophageal fistula closure.
Keywords
Introduction
China has a high incidence of esophageal carcinoma, and approximately 90% of esophageal carcinoma is esophageal squamous cell carcinoma (ESCC). 1
The thoracic esophagus is adjacent to large vessels, the pericardium, the trachea, bronchi, vertebrae, and other tissues. Advanced esophageal carcinoma can easily invade the normal tissue and lead to an esophageal fistula (EF), which may further cause hemoptysis, pneumonia, lung abscesses, and death.
Prior research has shown that the T4 stage and maximum tumor thickness are risk factors for EF formation.2,3 Dose-escalated radiation may improve the local disease control rate and survival in patients who have ESCC with large tumor volumes. 4 However, there is no unified regimen for ESCC complicated with an EF. Conventional fractionated and dose-escalated radiotherapy (RT) may be inappropriate because such treatments can damage the esophageal wall and cause an imbalance between tumor shrinkage and normal tissue repair, leading to or aggravating an EF. This report presents a patient who developed ESCC with a tracheoesophageal fistula and severe hemoptysis. Hemostasis and an individualized RT mode were conducted because of the patient’s critical condition. The patient was successfully treated with staged dose-escalated RT. We herein share our clinical experience to help other clinicians who encounter similar patients.
Case presentation
A 58-year-old Chinese man was hospitalized because of a >1-month history of dysphagia and hemoptysis without cough, sputum, chest pain, or fever. The patient had a 15-year history of stage 2 hypertension, a long-term history of smoking and drinking, and no family history of cancer. He was 173 cm in height and 68 kg in weight on admission. His hemoglobin level was 108.4 g/L, and all other blood test results were normal. Contrast-enhanced computed tomography (CT) revealed a large solid tumor in the upper esophagus and a tracheoesophageal fistula (Figure 1(a)) without distant lymph node or organ metastases. Esophagography revealed a large lesion with esophageal stenosis measuring approximately 8 cm in length (Figure 1(a)). Esophagogastroduodenoscopy showed an ulcerated tumor with raised margins that originated 22 cm from the incisors (Figure 2(a)), and histologic examination of a biopsy specimen revealed structured invasion of atypical squamous epithelium-like cells in the normal esophageal epithelium, consistent with invasive, poorly differentiated squamous cell carcinoma (Figure 2(b)). Therefore, the tumor was classified as stage IVA (T4bN0M0) ESCC.
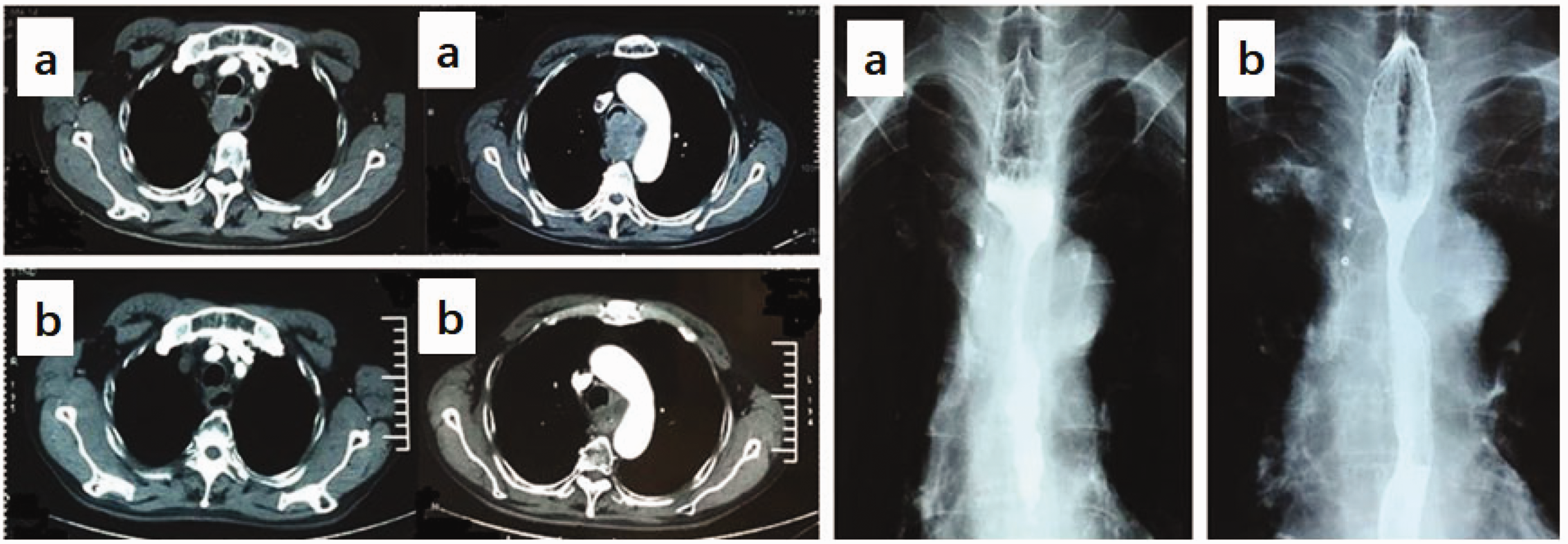
Computed tomography and esophagography. (a) Images before radiotherapy. Contrast-enhanced chest computed tomography revealed a large solid tumor in the upper esophagus and a tracheoesophageal fistula. Esophagography revealed a large lesion with esophageal stenosis measuring approximately 8 cm in length and (b) Images after radiotherapy. Contrast-enhanced computed tomography and esophagography revealed tumor shrinkage and fistula repair.
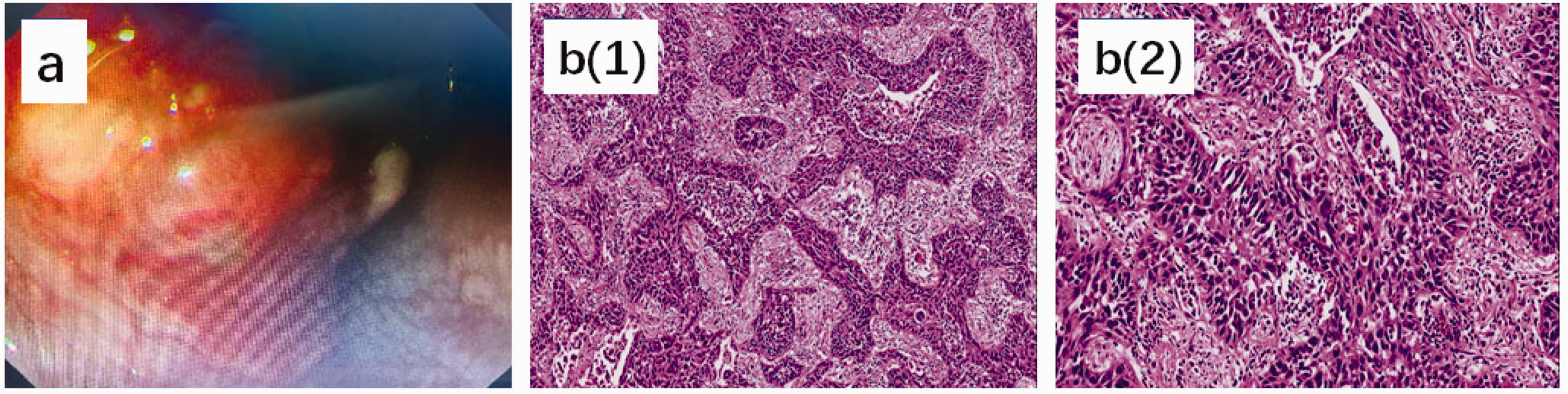
Esophagogastroduodenoscopy and histopathologic examination. (a) Esophagogastroduodenoscopy revealed an ulcerated tumor with raised margins originating 22 cm from the incisors and (b) Histopathologic examination of a biopsy specimen (hematoxylin–eosin stain) revealed squamous cell carcinoma. (1) Magnified view (100×) exhibiting invasion of the normal esophageal epithelium by deeply stained abnormal cells. (2) Magnified view (200×) exhibiting structured invasion of atypical squamous epithelium-like cells with irregularly shaped nuclei, anisonucleosis, and polychromasia.
The patient developed massive hemoptysis after admission. Even after receiving bilateral bronchial and intercostal artery embolization, he still developed massive hemoptysis twice in 4 days, with a blood volume of more than 400 mL each time. The bleeding temporarily ceased after intravenous administration of 10 U of pituitrin. We applicated staged dose-escalated RT as follows: intensity-modulated RT, 6-MV X-ray, 5 days per week. The gross tumor volume was determined by contrast-enhanced CT. The clinical target volume was defined as the gross tumor volume plus a margin of 0.8 cm on each side and 1.5 cm above and below the tumor mass. The planning target volume was defined as the clinical target volume plus a margin of 0.5 cm in all directions. Three treatment stages were used: 6.0 Gy in 5 fractions for the first, 7.5 Gy in 5 fractions for the second, and 46.8 Gy in 26 fractions for the third.
The hemoptysis stopped during the first stage of treatment, and the dysphagia was relieved throughout the second stage. Contrast-enhanced CT and esophagography after RT revealed tumor shrinkage and fistula repair (Figure 1(b)). The patient was able to swallow semi-solid and soft foods, and his weight increased by 3 kg. He developed no acute toxicities during the RT. The patient’s treatment course is shown in Figure 3.

Treatment course from admission to the end of dose-escalated radiotherapy.
Six courses of chemotherapy with 5-fluorouracil and cisplatin were administered 2 weeks after RT. We treated the patient with RT at 50.4 Gy in 28 fractions for recurrence in the middle esophagus and cervical lymph nodes 11 months after he was diagnosed with ESCC. We then conducted RT at 30 Gy in 10 fractions for ilium bone metastasis 13 months after the diagnosis. The patient developed another tracheoesophageal fistula 18 months after the diagnosis, and he died of respiratory insufficiency 20 months after being diagnosed with ESCC.
The patient’s wife provided written informed consent for publication of the patient’s anonymized information in this case report. The reporting of this case conforms to the CARE (CAse REport) guidelines. The Ethics Office of the Fourth Hospital of Hebei Medical University provided ethics approval for the publication of this report.
Discussion
We have herein described a 58-year-old man with stage IVA (T4bN0M0) ESCC who underwent staged dose-escalated RT and achieved tracheoesophageal fistula closure. This patient developed a tracheoesophageal fistula after the trachea had been invaded and compressed by the tumor. Contrast-enhanced CT revealed that the entrance of the fistula was covered by the tumor tissue, preventing food and digestive fluids from entering the trachea through the fistula. The airway might have been minimally irritated by esophageal contents, explaining why he did not develop a severe cough. However, the patient’s condition became critical because of massive hemoptysis. The hemoptysis was temporarily stopped with the administration of pituitrin. Nevertheless, we faced the following four issues. First, because the EF and hemoptysis had been caused by the ESCC, the patient’s symptoms required anti-tumor therapy. Second, the hemoptysis could have recurred at any time. Third, after consultation with surgeons and anesthesiologists, surgery was not recommended because of its substantial risk. Fourth, given the patient’s state, RT might have been an efficient and secure option. However, we hoped that the fistula would close as the tumor shrank.
The two known causes of EF are tumors and treatment-related factors. An advanced esophageal tumor can invade the esophageal tissues, disrupt their structures, and cause an EF. Additionally, RT and chemoradiotherapy can damage the esophageal wall and cause malnutrition and an imbalance between tumor shrinkage and normal tissue repair, thereby leading to EF formation.5–7 A tumor-related EF might not heal without anti-tumor therapy; however, anti-tumor therapy might also aggravate a tumor-related EF. Therefore, the treatment of an existing tumor-related EF, especially local treatment such as RT, remains controversial. The efficacy of RT in patients with an EF has been demonstrated in several cases8–10 even though a tumor-related EF was previously thought to be a contraindication.
A prior study showed that ESCC with a large tumor volume was correlated with poor local control and overall survival (OS) rates and that dose-escalated RT could improve local disease control and OS in these patients. 4 Dose-escalated RT is a simultaneous integrated boost strategy in which the tumor is given a high RT dose while minimizing the radiation dose to the surrounding organs, and it has produced promising results with improved tumor control and OS rates.4,11 Although this technology is inspiring, it was unsuitable for our patient’s situation because rapid tumor regression due to a dose increase might have increased the size of the EF or aggravated the bleeding. We modified the dose escalation from simultaneous to staged and implemented the following RT strategy. In the first treatment stage, the patient received 6.0 Gy in 5 fractions (1.2 Gy per fraction). The tumor was smaller at this point; the treatment forced it to gently contract, giving the normal tissue time to repair. The hemoptysis rapidly decreased in volume and eventually stopped during this period. In the second stage, the patient received 7.5 Gy in 5 fractions (1.5 Gy per fraction). The purpose of this stage was to steadily increase the fraction size while increasing the tumor control rate, leading to normal tissue repair. The patient’s dysphagia was relieved during this time, and contrast-enhanced CT following the first two stages of treatment revealed decreased tumor volume and tracheal compression with no signs of the EF. In the third stage, the patient received 46.8 Gy in 26 fractions (1.8 Gy per fraction) because of the decreased risk of the EF and hemorrhage. Chest CT revealed no visible compression or fistula in the tracheal wall after completion of the three treatment phases. The patient’s OS was 20 months. His symptoms eased during radiation, and he remained symptom-free for about 13 months.
Staged dose-escalated RT was used to effectively treat this patient by safely ending the hemoptysis and easing symptoms. The EF closed after staged dose-escalated RT. We have shared this patient’s treatment course in the hope that patients with similar conditions will receive therapeutic benefits.
Conclusion
Staged dose-escalated RT has clinical applications in some situations. We hope that more patients can benefit from this technology. Nevertheless, more studies are needed to examine the efficacy of staged dose-escalated RT and its adverse events.
Footnotes
Author contributions
Zhen CJ and Zhang P contributed to the manuscript writing and editing and the data collection. Song YZ, Bai WW, and Qiao XY contributed to the data analysis. Zhou ZG contributed to the study conceptualization and supervision. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.