
Abstract
This case details a male patient in his late 50s weighing 90 kg who traveled to Burkina Faso, Africa, for approximately 1 month. He developed fever, headache, and generalized myalgia 3 days after returning to Chongqing, China. The interval from the emergence of the patient’s symptoms to the diagnosis of severe falciparum malaria and the commencement of artesunate treatment was 9 days. Despite effective anti-Plasmodium falciparum treatment, the patient ultimately succumbed to multiple organ failure caused by P. falciparum infection complicated by an acute subdural hematoma.
Introduction
Local transmission has been absent in China since the World Health Organization (WHO) declared the country malaria-free on 30 June 2021. 1 However, 2000–4000 imported malaria cases are reported annually, including occasional fatalities. 2 Among malaria-related deaths caused by Plasmodium falciparum, cerebral malaria is one of the most fatal factors, while acute subdural hematoma represents an uncommon clinical manifestation of cerebral malaria. 3 The WHO guidelines for malaria clearly state that untreated severe malaria is almost 100% fatal, and rapid and effective antimalarial treatment is key to reducing mortality rates. 4 This case report describes a patient whose diagnosis was delayed, leading to rapid progression to severe malaria during hospital treatment and the rare complication of subdural hemorrhage. Despite receiving effective antimalarial treatment targeting the parasite, the patient ultimately died.
Case
This case describes a male patient in his late 50s, weighing 90 kg, who traveled to Burkina Faso, Africa, for approximately 1 month and returned to Chongqing, China, in September 2024. He self-administered nonsteroidal anti-inflammatory drugs 3 days after his return for fever, headache, and widespread myalgia. A private community clinic identified and treated him for acute upper respiratory infection 7 days after his return. Nine days after his return, the patient sought treatment at Chongqing General Hospital, Chongqing, after community clinic care proved ineffective. An outpatient throat swab test showed the presence of influenza B antigen; therefore, he was prescribed oral Arbidol. He was hospitalized on the evening of the 10th day after his return due to recurrent chills and fever.
The patient was attentive and light-responsive at the time of admission, with bilateral pupils equal in size and round, approximately 3 mm in diameter. Head computed tomography (CT) indicated lacunar cerebral infarction (Figure 1(a)). The blood test showed no anemia, with a red blood cell count of 5.41 × 1012/L (normal: 4.3–5.8 × 1012/L) and hemoglobin level of 173 g/L (normal: 130–175 g/L). He exhibited a decrease in platelet count (36 × 109/L, normal: 125–350 × 109/L) and a slightly higher creatinine level (107.3 µmol/L, normal: 57–97 µmol/L). Following admission, the patient received treatment with Arbidol, cefuroxime, recombinant human thrombopoietin, electrolyte imbalance correction, and crystalloid fluid resuscitation. He was later screened for malaria and dengue fever. Platelet transfusion was requested from the central blood bank.

Head CT scans. (a) First day of admission. (b) Two days after admission and (c) four days after admission. CT: computed tomography.
On the second day postadmission, the patient showed a Glasgow Coma Scale score of 9 and developed anisocoria (left pupil, 5 mm; right pupil, 2.5 mm) and hypotension (systolic blood pressure <80 mmHg). The patient displayed indications of anemia, with a red blood cell count of 3.92 × 1012/L and hemoglobin level of 125 g/L. The platelet count decreased to 12 × 109/L. Prothrombin time (18.6 s, normal: 9–14 s) and activated partial thromboplastin time (53.6 s, normal: 20–40 s) suggested hypocoagulability. Renal impairment worsened, with a serum creatinine level of 185.9 µmol/L and blood urea level of 21.2 mmol/L (normal: 3.1–8 mmol/L). Hyperlactatemia occurred, with a plasma lactate level of 13.2 mmol/L (normal: 0.5–1.7 mmol/L). A peripheral blood smear showed 15% P. falciparum parasitemia (Figure 2(a)). The patient received intensive care unit mechanical ventilation. Norepinephrine and fluids were provided to maintain circulatory stability. Mannitol, synthetic glucocorticoids, and ice were used to reduce intracranial pressure and protect cerebral function. The antibiotic regimen was altered to broad-spectrum antibiotics. Platelets and fresh frozen plasma were administered to improve coagulation function. The patient received intravenous artesunate (120 mg, supplied by the Chinese Center for Disease Control and Prevention (CDC)) within 4 h of malaria diagnosis.
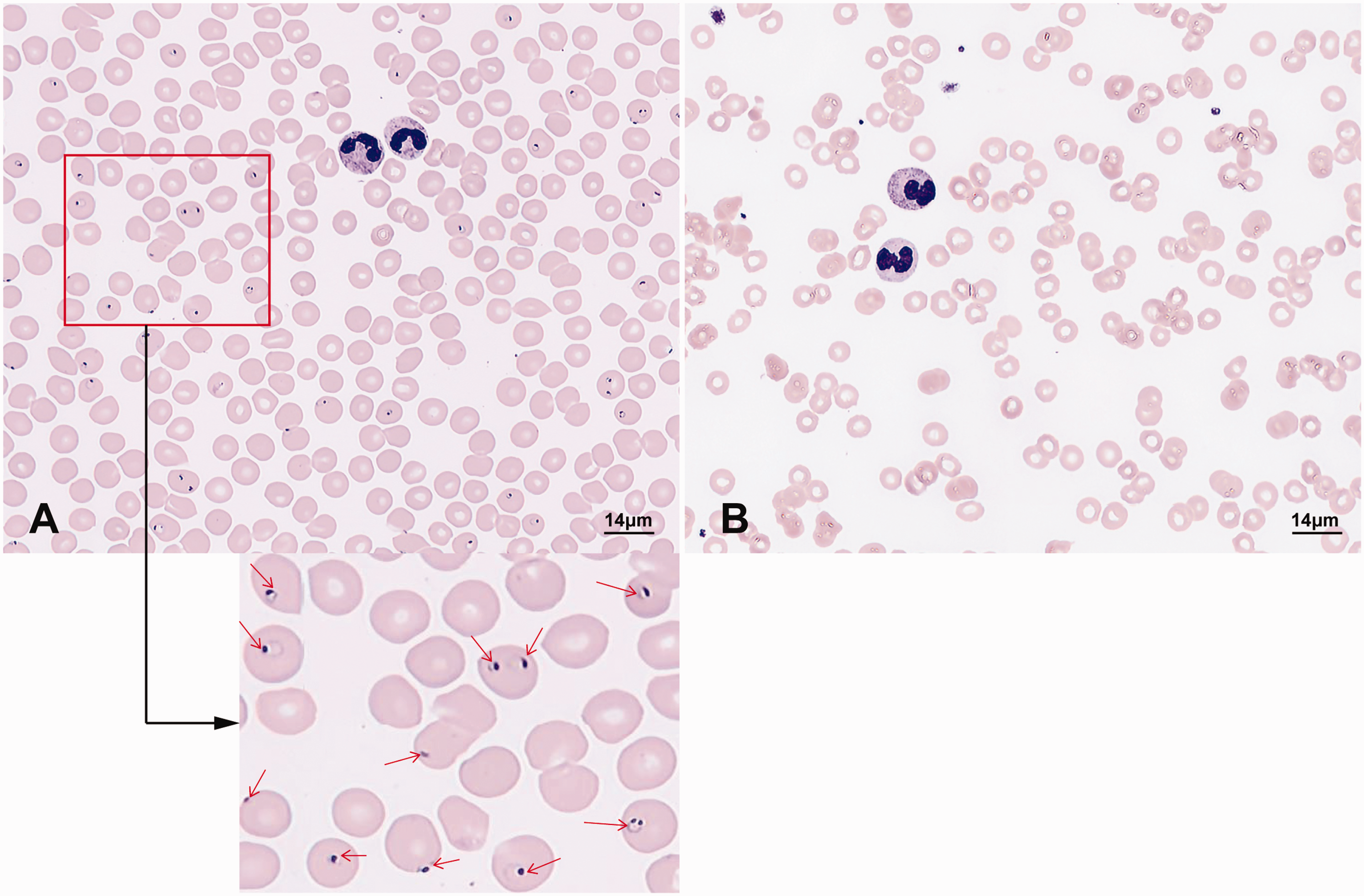
Peripheral blood smears. (a) First day after admission and (b) five days after admission. The red arrow in (a) indicates the Plasmodium falciparum ring-stage.
On the third day after admission, a follow-up head CT revealed a subdural hematoma in the left fronto-temporo-parieto-occipital area and the right frontal region, accompanied by a considerable midline shift to the right, suggesting herniation (Figure 1(b)). Before intracranial hematoma evacuation and decompressive craniectomy, the patient received cryoprecipitate, fresh frozen plasma, and platelets. Despite the administration of synthetic glucocorticoids and other drugs to lower intracranial pressure following surgery, cerebral edema persisted until the patient’s death (Figure 1(c)).
The patient received 120 mg artesunate intravenously every 12 h for 10 days, followed by a 1-week course of nasogastric artesunate–amodiaquine. From 5 days after admission, peripheral blood smears were negative for P. falciparum (Figure 2(b)).
The patient’s subsequent treatments primarily comprised hemofiltration, somatostatin, omeprazole, broad-spectrum antibiotics, and various blood products; norepinephrine and vasopressin were administered for circulatory stability; and continuous mechanical ventilation was performed for respiratory support. The patient eventually died of hemorrhagic shock resulting from uncontrollable massive gastrointestinal hemorrhage 29 days after admission. We have deidentified all patient details. The reporting of this study conforms to the Case Report (CARE) guidelines. 5
Discussion
This imported case of malaria was reported because the patient presented late to the hospital, which led to a rapid deterioration of his condition. Malaria had progressed to severe falciparum malaria when diagnosed. 4 In addition to cerebral malaria symptoms, the patient developed the rarely reported complication of acute subdural hematoma. The poor therapeutic outcome ultimately led to his death.
Following the elimination of malaria in China after 2021, the malaria antibody levels of interior county people (those who live far away from the border of China) have declined. 6 The patient lived in Chongqing, far from China’s borders, and did not receive antimalarial prophylaxis before or during his trip to Africa. After returning to Chongqing, artesunate was given 9 days after the illness began. Despite the efficacy of the anti-P. falciparum medication, multiple organ failure induced by P. falciparum in his body ultimately resulted in his death.
Previous research indicates that thrombocytopenia in malaria patients results from multiple factors and is closely associated with the severity of falciparum malaria.7,8 Due to the patient’s thrombocytopenia and coagulation dysfunction, subdural hemorrhage occurred, which is an uncommon occurrence in cerebral malaria. In the event of obvious symptoms of intracranial lesions, the doctor used drug intervention measures, such as synthetic glucocorticoids, to treat cerebral malaria. Nevertheless, the pharmacological treatment failed to significantly improve the patient’s cerebral malaria symptoms, consistent with previous research demonstrating that synthetic glucocorticoid administration does not decrease the mortality rate in patients with cerebral malaria. 9 After confirmation of a subdural hematoma, the patient underwent intracranial hematoma evacuation and decompressive craniectomy. However, the patient’s intracranial condition did not improve substantially. Intracranial surgery was unlikely to provide substantial therapeutic benefits for this patient with cerebral malaria complicated by subdural hematoma, as evidenced by the patient’s surgical outcome. The therapeutic method may not be equivalent to that for subdural hematomas caused by other reasons; thus, additional research is required.
Individuals lacking sufficient malaria antibodies should seek professional advice from specialized institutions or infectious disease control experts before traveling to malaria-endemic areas. Preventive measures, such as prophylactic medications, should be proactively implemented. If initial symptoms develop, individuals should, as soon as possible, seek prompt diagnosis and effective treatment at specialized medical institutions with expertise in infectious disease control, rather than self-medicating or visiting private community clinics. Healthcare providers must carefully evaluate the patients’ medical and travel histories and perform immediate parasitological testing for those who are suspected of malaria exposure. Additionally, the most important aspect of malaria treatment is the early delivery of appropriate antimalarials, especially artemisinin-based combination therapies. Ultimately, prevention is more effective than treating late-stage severe malaria.
Footnotes
Acknowledgments
We appreciate Dr Meng Zhang’s assistance in collecting the patient’s medical records.
Author contributions
NX and XJ conceived and drafted the study. HY and XJ revised the manuscript. All authors read, edited, and approved the final manuscript.
Data availability statement
Data are available from the authors upon request.
Declaration of AI
AI tools were solely employed as a translation aid to assist with language refinement. We independently developed the core content and discussion of the paper without using AI-generated text.
Declaration of conflicting interests
The authors declare that they have no potential conflicts of interest to disclose.
Ethical considerations
All relevant treatments were performed with informed consent obtained from either the patient or his legal guardians, supported by signed consent documentation. Informed consent for permission to publish was obtained from the patient’s son.
Funding
This work was supported by the Health Commission of Chongqing and The Science and Technology Bureau of Chongqing (2024MSXM162).