
Abstract
Cryptococcal meningitis has been reported to be primarily associated with human immunodeficiency virus infection. Herein, we report the case of a male patient in China with recurrent acute stroke as the first clinical manifestation, followed by several symptoms of intracranial infection, such as headache, a stiff neck, disturbance of consciousness, and high fever. The patient tested negative for human immunodeficiency virus and was diagnosed with cryptococcal meningitis after lung computed tomography, cranial computed tomography, cranial magnetic resonance imaging, and cerebrospinal fluid examination. The combination of conventional amphotericin B and flucytosine tablets progressively worsened the patient’s condition. This was accompanied by a series of complications, such as respiratory failure, hepatic and renal insufficiency, and infectious shock, leading to the patient’s death. To date, only a few cases of non-acquired immunodeficiency syndrome-related cryptococcal meningitis with recurrent acute stroke have been reported. This case report suggests that clinicians should be alert to the possibility of cryptococcal meningitis in patients with imaging manifestations of meningitis and promptly perform cryptococcal capsular antigen testing, a highly sensitive screening method. Therefore, this case study could lead to new insights into the clinical diagnosis and treatment of non-acquired immunodeficiency syndrome-related cryptococcal meningitis with recurrent acute stroke.
Introduction
Cryptococcal meningitis (CM) is the primary cause of death from infectious diseases of the central nervous system worldwide. Furthermore, the disease causes approximately 500,000 deaths every year, and the mortality rate is estimated to reach 25%–50%, even after treatment. 1 CM is characterized by diverse and often nonspecific clinical manifestations, which increase the difficulty of diagnosis. The disease is more prevalent in people with immunodeficiency, such as patients infected with human immunodeficiency virus (HIV), those receiving immunosuppressive therapy, those with malignant tumors, and those suffering from congenital immunodeficiency. Among people with normal immune functions, the incidence rate of Cryptococcus infection is estimated to be 1 case per 100,000 people. 2 Herein, the case of a patient with non-acquired immunodeficiency syndrome (AIDS)-related CM with recurrent acute stroke is reported, with evaluation of the clinical features, laboratory examination, treatment, and disease evolution. Therefore, by presenting this case, we expect to improve the clinical diagnosis and treatment of this disease in the future.
Case presentation
Summary of medical history
The patient, a man in his early 60s, was admitted to the hospital after a complaint of repeated weakness of the left upper and lower limb for more than 4 months. More than 4 months ago (24 July 2022), the patient experienced weakness in the left upper and lower limbs. The left upper limb could be lifted; however, he failed to hold things stably with his left upper limb. Additionally, he walked with dragging of the left lower limb. He exhibited no fever, no dry cough, no weight loss, no rash, and no joint pain. He was admitted to Taizhou Hospital in Zhejiang Province on 24 July 2022. Head computed tomography (CT) showed multiple lacunar foci in the bilateral basal ganglia, radiative crown, and hemioval center, along with white matter degeneration (Figure 1). On 25 July 2022, head magnetic resonance imaging (MRI) and diffusion-weighted imaging (DWI) revealed recent occurrence of cerebral infarction in both cerebellar hemispheres (Figure 2). On 28 July 2022, magnetic resonance angiography (MRA) of the head revealed that the bilateral internal carotid arteries and anterior, middle, and posterior cerebral arteries showed clear, natural, rough edges; mild segmental stenosis of lumen; and no cystic dilatation. No abnormal vascular mass shadow was found in the skull (Figure 3). After being diagnosed with cerebral infarction, the patient was treated with enteric-coated aspirin tablets (200 mg qd) and atorvastatin tablets (40 mg qn) for 1 week. After discharge, the patient stopped using aspirin and atorvastatin tablets on his own. Four weeks after discharge (19 August 2022), the muscle strength of the patient’s left upper and lower limbs returned to normal. One month ago (28 October 2022), the patient developed left upper and lower limb weakness again, and the symptoms were the same as before. On 29 October 2022, he was admitted to Zhejiang Provincial People’s Hospital and diagnosed with cerebral infarction, but the specific treatment remained unknown. On 14 November 2022 (during hospitalization), the patient experienced increased weakness in the left upper and lower limbs. He could lift the left upper limb but could not hold anything stably; moreover, he could lift the left lower limb but could not walk. He continued to be hospitalized in Zhejiang Provincial People’s Hospital; after treatment, his left upper limb could hold things stably, but the left lower limb showed claudication. However, during hospitalization, 40 h before admission (26 November 2022), the patient once again experienced increased weakness in the left upper and lower limbs. He could not move his left upper and lower limbs on the bed surface, his left limb was numb, his speech was vague, and he choked while eating. He developed cough and expectoration as well as breathing phlegm sounds. He was transferred to our hospital (Tiantai County People’s Hospital) on 28 November 2022. According to the previous medical records, the patient had a history of hypertension for 12 years, and the highest pressure recorded was 185/95 mmHg. Therefore, the patient was treated with valsartan hydrochlorothiazide tablets (80 mg qd), but his blood pressure was not monitored as usual. In addition, as the patient had type 2 diabetes for 12 years, he was treated with gliclazide sustained-release tablets (30 mg qd) and acarbose tablets (50 mg tid); however, his blood glucose level could not be stabilized. The patient denied any medical history of AIDS, syphilis, tuberculosis, coronary heart disease, or cancer. He also denied any history of poultry or pigeon ownership, exposure to bird droppings and poison, smoking and drinking, and recent vaccination.

Head computed tomography showing multiple lacunar foci in the basal ganglia, radiative crown, and hemioval center.
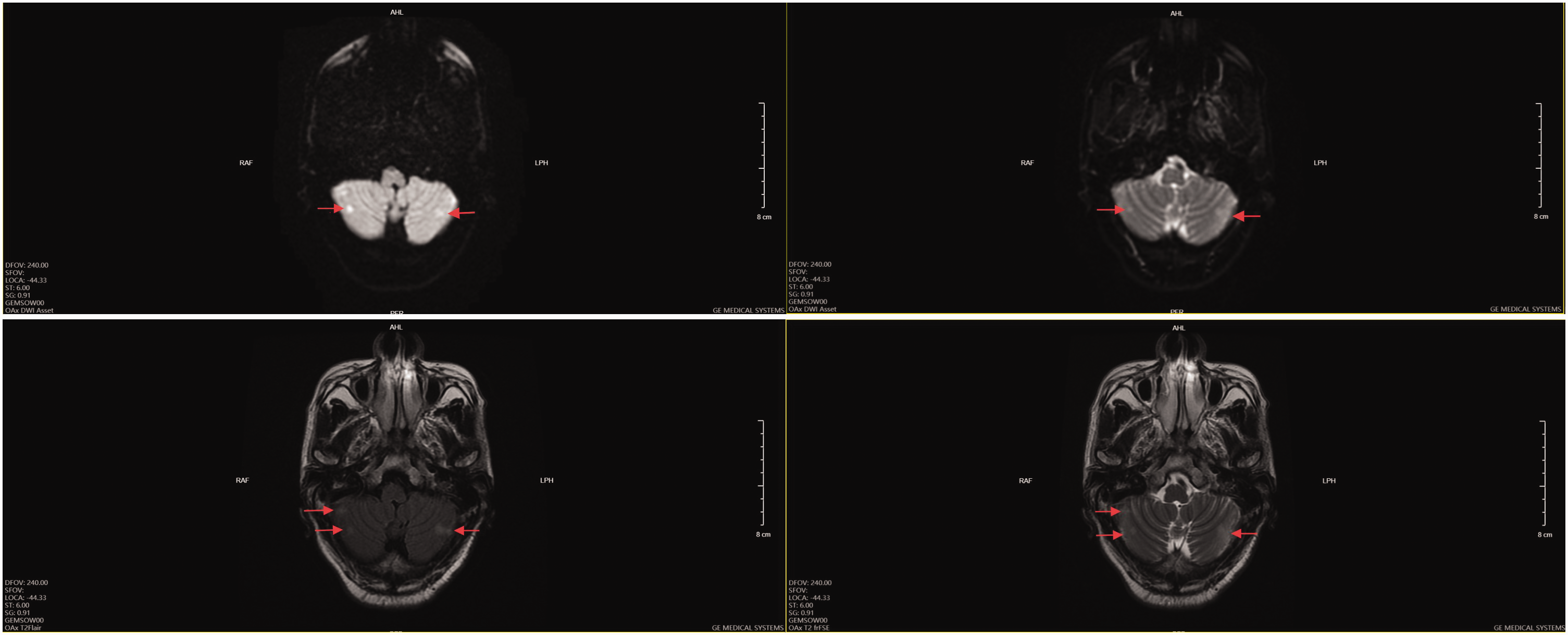
Head magnetic resonance imaging and diffusion-weighted imaging revealing recent cerebral infarction in both cerebellar hemispheres.
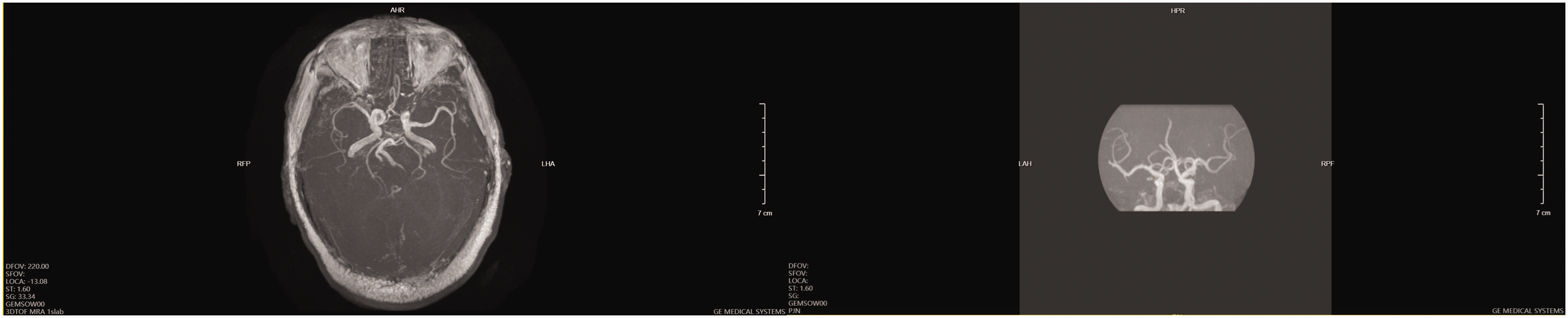
Head magnetic resonance angiography showing mild cerebral atherosclerosis.
Physical examination
The patient’s body temperature was 37°C, pulse rate 109 times/min, respiratory rate 17 times/min, and blood pressure 177/106 mmHg. Breathing sounds were coarse and wet rales were heard in both lungs. No concrete evidence of heart or abdominal ailment was noted after examination. Neurologic physical examination showed clear mind, slurred speech, uncooperative mental examination, soft neck, and negative meningeal irritation. The diameter of the two pupils was 0.3 cm; they were equal in size, round, and sensitive to light reflection. Eye movement was free, nystagmus was negative, visual field was not defective, coarse hearing was normal, and the corneal reflex was present. Moreover, the left nasolabial groove was shallow, the tongue was extended to the left, and the pharyngeal reflex was normal. In addition, muscle strength test was uncooperative, left muscle strength coarse test level 0, while the right limb could be lifted autonomously. Furthermore, the muscle tension of the left limb was low. However, the muscle tension of the right limb was normal, and the patient’s ataxic gait was uncontrollable. Pain and temperature sensation was decreased on the left side, while on the right side, superficial sensation was normal. On examination of the tendon reflex (++), the left Babinski sign was present, whereas the right Babinski sign was absent. Auxiliary examination revealed that all indices in the routine urine test and complete set of biochemical tests were within the normal ranges, with negative results for blood HIV, syphilis antibody, novel coronavirus antibody, and novel coronavirus nucleic acid test.
Treatment course
After admission, the patient was treated with clopidogrel hydrochloride tablets (75 mg qd) and atorvastatin tablets (40 mg qd) for symptomatic treatment. In addition, various tests were completed. Syphilis, HIV, blood routine, comprehensive immune examination, and outpatient antinuclear antibody tests showed normal results. On 29 November 2022, lung CT showed inflammation in both lungs (Figure 4). Cryptococcus was not detected in sputum culture. Cardiac ultrasound examination (29 November 2022) revealed decreased left ventricular diastolic function and mild tricuspid regurgitation. Dynamic electrocardiogram showed normal sinus rhythm. No basis for cardiac embolism was found. On 2 December 2022, anti-neutrophil cytoplasmic antibody test was negative. On 2 December 2022, head CT showed an increase in the density of the right temporal frontal lobe and disappearance of the sulcus. Moreover, cerebral infarction was observed in the brainstem, right basal ganglia, and paraventricular lacuna (Figure 5). On 3 December 2022, enhanced cranial MRI showed multiple recent infarcts in the brainstem and bilateral cerebral hemisphere. The meninges of the right frontotemporal parietal lobe were enhanced, indicating the possibility of meningitis. These findings were combined with the clinical manifestations (Figure 6). On 2 December 2022, neck MRA showed that the common carotid artery was well-filled, with natural flow, smooth wall, and no abnormal stenosis or local dilation. The internal carotid arteries on both sides displayed multiple wall calcifications of intracranial sections; each section and its branches were well-filled, with smooth tube wall and no abnormal stenosis or local dilation. The main trunk and branches of the external carotid artery were well-filled, with natural flow, smooth wall, and no abnormal stenosis or local dilation. Both sides of the vertebral arteries were well-filled, with natural flow, smooth tube walls, and no abnormal stenosis or local dilation. There was no vascular string of beads sign change. These findings did not conform to the imaging manifestations of cerebrovascular inflammation. Dynamic electrocardiogram showed normal sinus rhythm.
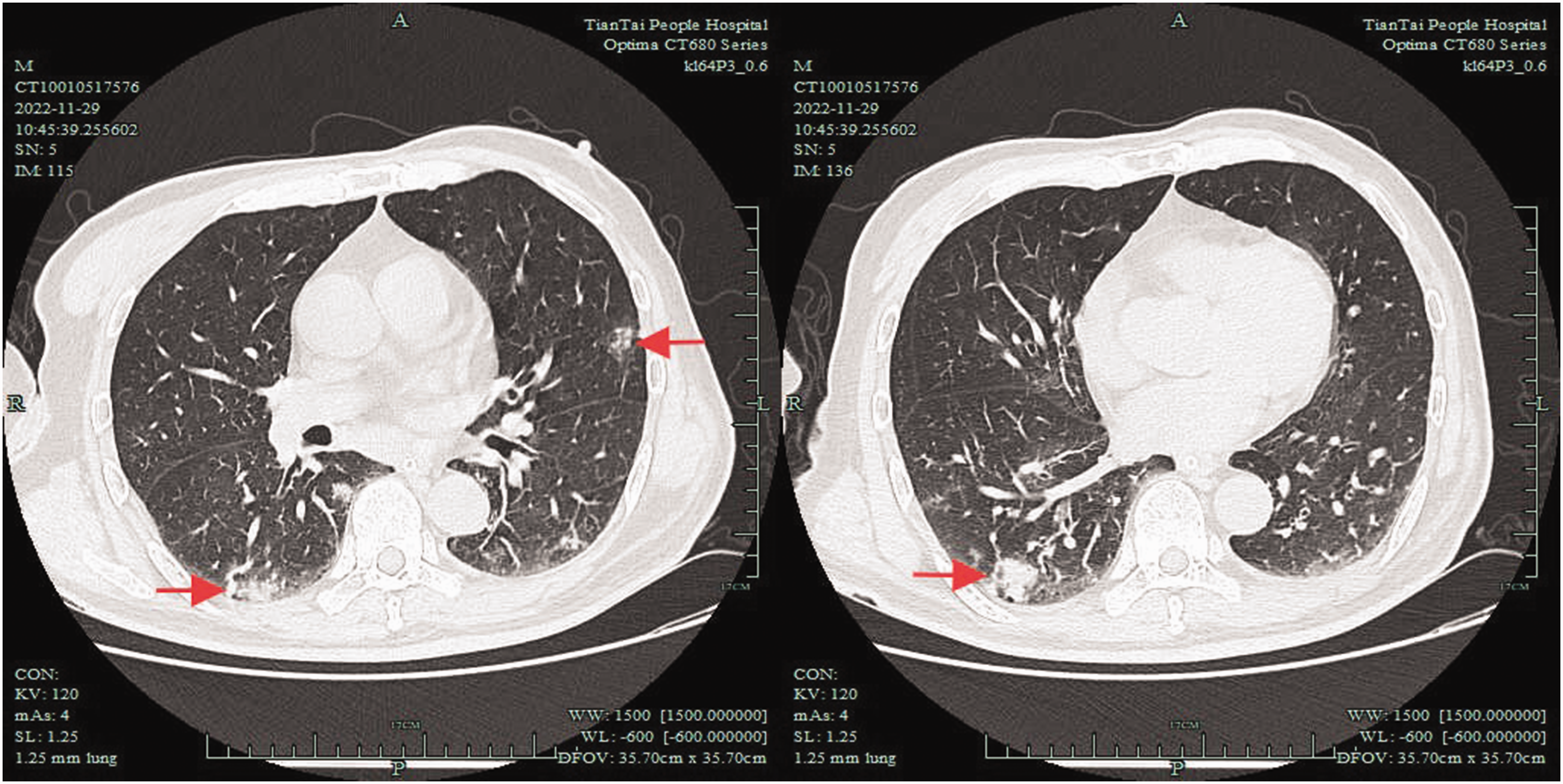
Lung computed tomography revealing patchy high-density shadows in both lungs.

Head computed tomography revealing low density in the right brainstem, increased density in the right temporal frontal lobe, and disappearance of the cerebral sulcus.

Enhanced brain magnetic resonance imaging revealing multiple patchy abnormal signals in the brainstem and bilateral cerebral hemispheres and enhanced meninges in the right frontotemporal parietal lobe.
On the 5th day of admission (2 December 2022), the patient developed headache and a stiff neck. Considering the presence of moist rales in both lungs, lung CT was performed, which showed inflammation in both lungs. Enhanced head MRI revealed meningeal enhancement in the right frontotemporal parietal lobe in addition to multiple recent infarcts in the brainstem and bilateral cerebral hemispheres, further indicating the possibility of meningitis concurrent with complicated infectious diseases in the central nervous system. Eventually, after obtaining validated informed consent from both the patient and his family members, a lumbar puncture was performed, which demonstrated an initial pressure of 150 mmH2O. Furthermore, in a Cryptococcus neoformans smear test, no Mycobacterium tuberculosis or other bacteria were found, but Indian ink staining detected Cryptococcus. Cerebral spinal fluid (CSF) was cultured on sandcastle agar medium; M. tuberculosis and other bacteria were negative, but C. neoformans was positive. His CSF biochemistry revealed a total protein level of 134 mg/dL. Routine CSF test revealed a white blood cell (WBC) count of 5.0 × 106/L (reference value: 0–8 × 106/L) and a chlorine level of 118.5 mmol/L. WBC count was within the normal range. The CSF glucose level was 2.77 mmol/L, which was within the normal range (reference: 2.22–3.89 mmol/L). The CSF protein level was 134 mg/dL (reference range: 8–43 mg/dL), indicating an increase. Simultaneous blood glucose measurement was 10.0 mmol/L. Blood Cryptococcus capsular test (lateral flow immunoassay) was positive.
The revised diagnosis of the patient confirmed CM, cerebral infarction, pulmonary infection, hypertension, and diabetes. Therefore, the patient was administered amphotericin B (25 mg qd) and fluorocytosine tablets (1000 mg 4 times a day). On the 6th day of admission, the patient was in a coma. The patient’s family refused to undergo lumbar puncture again and refused to have the cryptococcal antigen re-examined. Re-examination of the head CT showed that the lesion had not changed, but the density of the right temporal frontal lobe increased compared with that on the previous scan. A joint consultation with the infectious disease department was conducted, considering the progression of the disease itself and not the toxicity of the treatment or a systemic inflammatory response syndrome-like manifestation. On the 9th day, he suffered from respiratory failure (oxygen partial pressure in blood gas analysis was 58 mmHg) and developed hyperpyrexia. On the 10th day, he suffered from hepatic insufficiency and renal failure (alanine aminotransferase: 78 U/L (reference value: 9–50 U/L), aspartate aminotransferase: 81 U/L (reference value: 15–40 U/L), total bilirubin: 8.3 μmol/L (reference value: 0–26 μmol/L), direct bilirubin: 5.7 μmol/L (reference value: 0–8 μmol/L), indirect bilirubin: 2.6 μmol/L (reference value: 0–18.5 μmol/L), albumin: 27.80 g/L, globulin: 45.30 g/L, albumin/globulin ratio: 0.6, urea nitrogen: 19.02 mmol/L, creatinine: 218 μmol/L, and glomerular filtration rate: 218 μmol/L), along with the infectious shock. On 8 December 2022, the patient’s blood oxygen saturation dropped by 74%–78%, and his condition deteriorated rapidly. The patient was treated with 120 mg of methylprednisolone by intravenous drip, but his condition did not improve and he eventually died. The reporting of this study conforms to the Case Report (CARE) guidelines. 3
Discussion
CM is an infectious disease of the central nervous system caused by Cryptococcus and is the most common fungal infection in the central nervous system. This disease is frequently observed in immunocompromised patients, especially AIDS patients. 4 In China, most cases of CM are non-HIV-related (HIV-negative: 91.5%), and 50%–70% of patients with CM have normal immune function. 5 The main clinical manifestations are fever, progressive headache, and mental and neurological symptoms (insanity, excitability, disorientation, abnormal behavior, and lethargy). 6 However, the early onset of the disease is more insidious, and the chronic clinical symptoms are not typical, which is also the main reason for the frequent delay in the diagnosis of CM.
Brain MRI results differ between CM patients co-infected with HIV and those not co-infected with HIV. Cerebral infarction, hydrocephalus, and hypomeningeal enhancement are observed more often in non-HIV patients.7,8 The characteristics of lacunar cerebral infarction (lesion diameter ≤20 mm) in CM indicate that the small vessels are the main vessels involved, and large vessels are relatively rarely involved. 9 Chen et al. 10 believed that the lesions are mainly multiple infarcts, and the affected areas can be widely distributed, including the anterior and posterior circulation of cerebrovascular blood supply areas. Head MRI+DWI of this patient on 25 July 2022 showed recent occurrence of cerebral infarction in both cerebellar hemispheres, which is difficult to infer from the brain imaging changes of patients with CM. On 2 December 2022, head CT showed increased density of the right temporofrontal lobe; disappearance of cerebral sulci; and cerebral infarction in the brainstem, right basal ganglia, and paraventricular lacuna; the clinical manifestations were headache and neck stiffness. Enhanced head MRI on 3 December 2022 showed multiple recent infarcts in the brain stem and both cerebral hemispheres and enhanced meninges in the right frontotemporal parietal lobe, suggesting meningitis. Brain imaging clearly indicated intracranial infection. Common neurotropic infections are cryptococcal, tuberculous, and parasitic. Head MRI enhancement of the patient with intracranial parasitic disease showed multiple nodules or annular enhancement and multiple calcification in the brain parenchyma, but the imaging of the patient did not support this disease. CM patients can present with acute hemiplegia, headache, a stiff neck, and intracranial hypertension. The imaging features are mainly multiple infarctions, the affected areas can be widely distributed, and the meninges can be enhanced, accompanied by asymptomatic lung infection. Therefore, it is necessary to consider the possibility of this disease.
The main changes in the CSF of CM patients are increased WBC count, mainly lymphocytes, increased CSF protein level, and decreased CSF glucose level. 11 However, the current patient’s CSF WBC count was not high (5.0 × 106/L), raising the question of whether this finding is a manifestation of the patient’s low immune response and relatively serious disease. The diagnostic criteria for CM are as follows: 12 (a) Cryptococcus was positive in CSF fungal culture or cerebrospinal Indian ink staining; (b) Cryptococcus was found in the pathological examination of the brain tissues; (c) the clinical symptoms supported the diagnosis of meningitis, and a negative result was obtained from the CSF Indian ink smear and culture. However, a positive result was obtained from the Cryptococcus antigen test. The clinical examination of Cryptococcus Indian ink staining using CSF is a rapid and simple test, but the positivity rate and detection rate may be low due to the uneven specimen smear and too small or too few cryptococci, 13 which may affect the early diagnosis. The positivity rate can be increased via multiple tests, or the diagnosis can be confirmed by the culture of Cryptococcus and determination of cryptococcal capsular antigen. The patient underwent a lumbar puncture test, the result of Indian ink staining was positive, the CSF culture was positive, no M. tuberculosis or other bacteria were detected on the smear, and no M. tuberculosis or other bacteria were detected in the culture. Thus, the revised diagnosis was CM.
In addition to patients with immunodeficiency diseases, recent data have suggested an increase in the number of cases of Cryptococcus infection in non-HIV-infected people and healthy individuals. 14 Because of the slow disease onset, lack of specificity in clinical manifestations, and delayed treatment due to misdiagnoses, non-HIV patients are more vulnerable to neglect. 15 The current case involves an older, non-HIV-infected patient with a history of hypertension and diabetic arteriosclerosis who had suffered several acute stroke episodes within a short period. Due to the difficulty in communication after stroke, such patients may not be able to describe their symptoms well. The clinician’s thinking may be fixed on cerebrovascular disease, and the possibility of CM infection is not considered. When meningeal irritation is obvious and symptoms worsen, the opportunity for early treatment is lost. Therefore, if a patient has a preexisting lung infection, enhanced head MRI shows meningeal enhancement in the right frontotemporal parietal lobe, and there are possible imaging manifestations of meningitis, even without meningeal irritation, the patient should be screened for infectious diseases of the central nervous system. Although lumbar puncture is inconvenient, it is necessary for cryptococcal capsular antigen testing, ensuring early diagnosis and early treatment and reducing mortality, as strongly recommended by the current treatment guidelines and experts.16–18
This case revealed that in people without AIDS who have normal immune function and have unexplained conditions or deterioration of the original disease, when imaging data suggest meningitis, it is necessary to be alert to the possibility of CM or other central nervous system infectious diseases. Timely lumbar puncture examination or etiological screening (such as cryptococcal capsular antigen testing) should be conducted as soon as possible to achieve early diagnosis, reduce misdiagnosis, and gain valuable treatment time for antifungal therapy. This case report shows that the occurrence of CM in patients with obviously normal immune function is relatively rare and that associated stroke is even rarer. This case is novel and can provide a significant reference contributing to the clinical diagnosis and treatment of similar cases in the future.
Conclusion
In summary, non-HIV-infected individuals with CM, a fungal infection of the central nervous system with complex clinical manifestations, face unique diagnostic and treatment challenges. Deeply understanding the epidemiological characteristics of non-HIV-related CM in China and the characteristics of normal immunocompetence in most patients will help improve clinical vigilance. Typical CM is characterized by fever, headache, and mental symptoms. However, in the current case of an older patient with normal immunocompetence, stroke-like symptoms were the first symptoms, which was highly misleading. Delayed diagnosis caused by clinicians’ fixed thinking often leads to the loss of precious treatment opportunities. This case suggests that clinicians should be alert to the possibility of CM in patients with imaging manifestations of meningitis and promptly perform cryptococcal capsular antigen testing, a highly sensitive screening method. Early diagnosis and timely antifungal treatment are the keys to improving prognosis. The novelty of this case lies in the detailed recording of the clinical characteristics of CM-related stroke-like attacks in a patient with normal immune function, providing references and clinical insights for the diagnosis and treatment of similar complex cases. In the future, it is necessary to further explore the pathogenesis of non-HIV-related CM and optimize the diagnosis and treatment process.
Footnotes
Acknowledgments
We would like to thank Yingjun Chen from the Department of Infectious Diseases of Tiantai County People’s Hospital for the guidance during the revision process of the article.
Author contributions
BJY was the major contributor to the writing and revision of the manuscript. JW revised the drafts of the manuscript. JW and YHQ collected clinical data. WQF analyzed the data. JTX collected references. YPT made substantial contributions to the conception or design of the work. All authors have read and approved the final version of the manuscript, and all authors agree to the publication of this manuscript.
Consent for publication
Not applicable.
Data availability statement
The datasets provided within the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
All experimental protocols were approved by the Ethics Committee Reviews of Applications for Research Studies at Tiantai County People’s Hospital. Approval NO. 2024 Study No. 001. Written informed consent was obtained from the patient and his legal guardian(s). All the stated treatments were agreed upon by the patient and his family.
Funding
This work was financially supported by grants from the Zhejiang Medical and Health Science and Technology Program (2023KY399) and the Taizhou Science and Technology Plan Project (23ywb159).