
Abstract
Objective
To investigate the effects of femoral tunnel widening and tibial tunnel widening on the clinical and functional outcomes of a patient after anterior cruciate ligament reconstruction.
Methods
This study evaluated patients using the International Knee Documentation Committee score, Lysholm Knee Score, and Tegner Activity Scale score. Quadriceps and hamstring strength measurements on both operated and contralateral sides were recorded using an isokinetic dynamometer. Anterior laxity was assessed using a KT-1000 arthrometer. Tunnel widening rates were calculated as percentages using three-dimensional computed tomography. Statistical analysis included paired t-tests to assess tunnel widening effects.
Results
A total of 120 patients were included, with a mean age of 28.76 ± 6.65 years and a mean follow-up duration of 21.97 ± 8.64 months. No significant differences were found in femoral tunnel widening and tibial tunnel widening values between patients with significant (≥3 mm) and nonsignificant (<3 mm) KT-1000 measurements (p > 0.05). Femoral tunnel widening and tibial tunnel widening showed no significant correlation with Lysholm Knee Score, International Knee Documentation Committee score, or Tegner Activity Scale score (p > 0.05). Femoral tunnel widening was negatively correlated with extension and flexion strength at 60°/s and 180°/s (p < 0.05), whereas tibial tunnel widening showed no such correlation (p > 0.05).
Conclusions
These findings suggest that three-dimensional computed tomography-based femoral tunnel widening measurement and isokinetic dynamometer may help identify functional deficits in symptomatic patients following anterior cruciate ligament reconstruction.
Keywords
Introduction
Anterior cruciate ligament (ACL) reconstruction (ACLR) is currently the surgical treatment of choice for ACL injuries. 1 It is an effective method to restore knee joint function and reduce the risk of joint degeneration. It is common knowledge that the integration of the ACL tendon graft into the bone tunnels may be a key element in the success of the procedure. 2
Despite the development of surgical techniques in ACLR, the tendon–bone healing process remains inadequate. 3 Moreover, tunnel widening (TW) after ACLR is still a commonly reported phenomenon.4,5 Little is known about the mechanisms involved in TW. Synovial fluid, graft, and some cytokines are the main biological factors.6–8 In addition, mechanical factors such as micro-motion between the tunnel and graft, fixation, and position of the bone tunnel may be critical. 9 Although TW does not affect short-term clinical outcomes, graft healing in the tunnel may be affected after reconstruction surgery. At 6 months postoperatively, TW may indicate poor healing from the graft to the bone tunnel, resulting in increased laxity and ultimately affecting knee joint function.10,11
Although it has been reported that TW does not affect clinical outcomes after ACLR, large tunnels may compromise graft fixation in revision ACLR, even necessitating a two-stage procedure.12,13 Data from previous studies have suggested that TW has no effect on the clinical and functional outcomes of patients after ACLR. 14
Considering the important role of ACL in anterior and posterior stabilization of the knee, we hypothesized that TW, which affects the biomechanical relationship between the graft and bone tunnel, has a negative effect on functional and clinical outcomes.
This study aimed to investigate the effect of femoral tunnel widening (FTW) and tibial tunnel widening (TTW) on the clinical and functional outcomes of a patient after ACLR.
Methods
Our study was planned in a retrospective manner. The present study has been approved by the Institutional Review Board with the number 17073117-050.06. Informed consent was obtained from the patients for participation in the current study. The current study was performed in accordance with the Declaration of Helsinki.
A power analysis was conducted to determine the appropriate sample size based on an expected effect size of 0.5 (Cohen’s d), a significance level of α = 0.05, and a power of 80%. The final sample size of 120 patients was determined to achieve sufficient statistical power. Post-hoc power analysis was also performed to assess whether the sample size was adequate for detecting clinically meaningful differences between the groups.
Between January and December 2022, 143 patients who underwent anatomical ACLR with quadruple hamstring autograft using endobutton on the femoral side and bioabsorbable fixation screw on the tibial side in a single center by the same surgeon and underwent the same postoperative rehabilitation program were retrospectively analyzed. The inclusion criteria were as follows: (a) age between 18 and 50 years; (b) primary ACLR using hamstring autograft; (c) available preoperative and postoperative imaging; and (d) completion of isokinetic strength testing at the time of follow-up. The exclusion criteria were patients with multiple ligament injuries, revision surgery, history of contralateral knee ligament injury, Kellgren–Lawrence grade >2 arthroses on pre-op knee X-ray, cartilage lesion on intraoperative arthroscopy, and incomplete data. A consecutive sampling method was used to include all eligible patients who met these criteria during the specified timeframe. A total of 120 patients who met the inclusion criteria were included in the study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15
Rehabilitation protocol
Postoperative rehabilitation followed a standardized protocol progressing over approximately 6 months. Initial goals (weeks 0–2) included pain control, swelling reduction, and restoration of full knee extension with partial weight-bearing. By weeks 2–6, the patients advanced to full weight-bearing and initiated range of motion and strengthening exercises. From week 6 onward, progressive strength training, balance exercises, and functional activities were introduced, with sport-specific drills added after week 12. Return to full activity was typically allowed around 6–9 months, based on strength, stability, and functional assessments.
Clinical evaluation
A KT-1000 arthrometer (MEDmetric, San Diego, CA) was used for objective clinical examinations. To perform the KT-1000 side-to-side test, we followed the manufacturer’s protocol. 16 Briefly, tibial translation was calculated in millimeters at an anterior pulling force of 134 N, with the knee in the flexion position at 30°. The side-to-side difference between the ACLR-treated knee and contralateral healthy knee was calculated. A difference of ≥3 mm between both knees was recorded as significant.
The International Knee Documentation Committee (IKDC) score, 17 Lysholm Knee Score (LKS), 18 and Tegner Activity Scale (TAS) 19 score were recorded.
Quadriceps and hamstring strength measurements on the operated and intact sides were recorded using an isokinetic dynamometer (ID) (Cybex II). During the measurements, peak torque values in flexion and extension positions were determined at frequencies of 60°/s and 180°/s.
Radiologic evaluation
Owing to the advantages of three-dimensional analysis, a reliable imaging method, and more precise imaging for the assessment of bone tunnel boundaries, some authors recommend CT for the postoperative evaluation of ACLR. 20 The software technique for tunnel measurements and the methodology for measuring the tunnels were performed in accordance with the literature 21 (Figures 1 and 2).
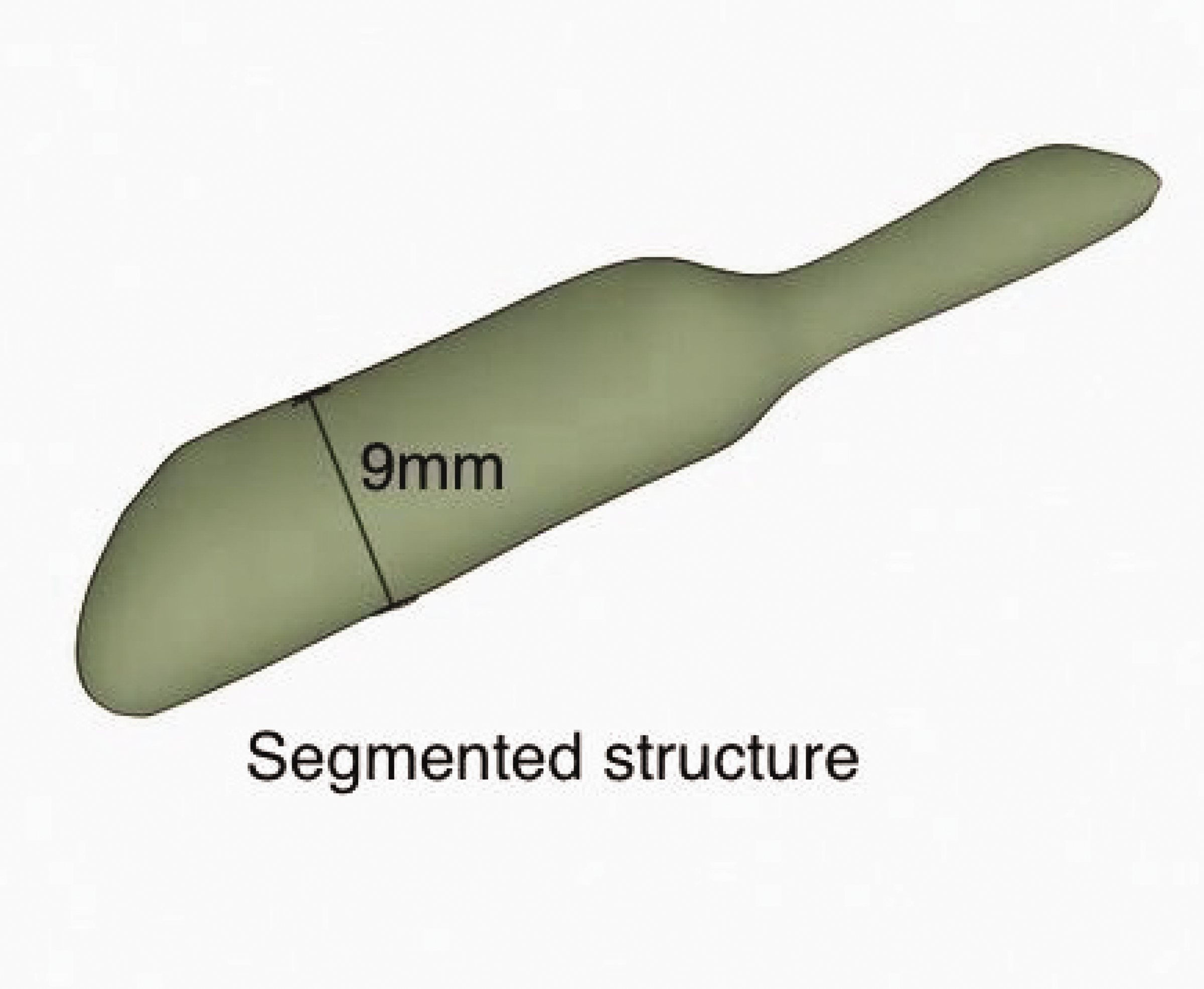
3D reconstruction of the femoral tunnel (green cylinder model) with maximal diameter quantification (9.0 mm). 3D: three-dimensional.

Coronal view of the tunnel within the distal femur, as visualized through 3D computed tomography reconstruction. 3D: three-dimensional.
The scan consisted of a minimum of 50 image slices with the following parameters: slice thickness, 1.5 mm; resolution, 512 × 512; voltage, 120 kVp; current, 250 mA.
The 3D-Slicer 5.6.2 program was used to measure tunnel sections in the CT images obtained from the patient. The measurement was performed by scanning each section where the tunnel was visible over all sections. The tunnel scanned in the 3D-Slicer 5.6.2 program was also displayed in three dimensions. The diameter of the cylindrical tunnel created on the 3D slicer 5.6.2 program was measured. The tunnel diameter obtained during surgery was recorded as a percentage compared with the tunnel diameter obtained during CT. FTW and TTW values were recorded and statistically analyzed. To assess the effect of TW on clinical and functional outcomes, we performed Pearson/Spearman correlation analyses to evaluate associations of FTW and TTW with functional scores (LKS, IKDC, and TAS) and ID measurements, followed by linear regression models adjusted for covariates (e.g. age, follow-up duration) to quantify independent effects, with statistical significance set at p < 0.05.
Intra- and interobserver reliabilities were evaluated using the intraclass correlation coefficient (ICC). For intraobserver reliability (test–retest), the same observer repeated measurements after a 1-week washout period using a two-way random-effects model for absolute agreement. For interobserver reliability, two independent observers analyzed the same dataset using a blinded approach, two-way random-effects model for average agreement. The washout period minimized memory bias between measurements. ICC values were interpreted as follows: <0.50 = poor, 0.50–0.75 = moderate, 0.75–0.90 = good, >0.90 = excellent.
Statistical analysis
Data were digitally recorded and analyzed using IBM SPSS Statistics (Version 22.0, Armonk, NY). Categorical variables were presented as frequencies (percentages) and continuous variables as mean ± standard deviation (SD). Normality of data distribution was assessed through Shapiro–Wilk tests, analysis of skewness/kurtosis, and visual inspection of histograms.
For categorical data comparisons, Pearson’s chi-square, Fisher’s exact test (for small sample sizes), or Spearman’s correlation were applied as appropriate. Continuous variables with normal distribution were compared using independent t-tests, whereas non-normally distributed variables were analyzed using the Mann–Whitney U test. For repeated within-group measurements of nonparametric data, the dependent Wilcoxon signed-rank test was utilized. A two-tailed p-value of <0.05 was considered to indicate statistical significance.
Results
A total of 120 patients were included in the study, with a mean age of 28.76 ± 6.65 years and a mean follow-up duration of 21.97 ± 8.64 months. Among them, 67 patients underwent right-sided and 53 underwent left-sided ACLR. The mean FTW value was 1.59 ± 0.55 mm, corresponding to an FTW rate of 15% ± 8%, whereas the mean TTW value was 1.23 ± 0.40 mm, with a TTW rate of 16% ± 6%. The mean LKS was 93.95 ± 7.60, mean TAS score was 7.69 ± 1.26, and mean IKDC score was 81.49 ± 11.69 (Table 1).
Demographic and clinical outcomes.

FTW: femoral tunnel widening; TTW: tibial tunnel widening; IKDC: International Knee Documentation Committee.
Muscle strength measurements using ID showed that the operated knee’s extension strength was 183.34 ± 50.36 N·m at 60°/s and 85.81 ± 25.28 N·m at 180°/s, compared with 214.14 ± 44.58 and 98.04 ± 25.43 N·m, respectively, in the intact knee. Flexion strength in the operated knee was 128.83 ± 34.38 N·m at 60°/s and 74.29 ± 21.57 N·m at 180°/s, whereas the intact knee recorded strength measurements of 141.97 ± 34.14 and 82.18 ± 24.44 N·m at the respective speeds (Table 1). KT-1000 arthrometer evaluation revealed that 35.8% of the patients had a side-to-side difference of 3–4 mm.
Statistical analysis revealed no significant correlation between FTW or TTW and clinical outcome scores, including LKS, IKDC score, and TAS score (p > 0.05; Table 2). However, patients with moderate-to-poor LKS scores had significantly greater FTW than those with good–to-very good LKS scores (p < 0.05; Table 3). FTW was negatively correlated with both extension and flexion strength at 60°/s and 180°/s (p < 0.05), whereas TTW showed no such relationship (p > 0.05; Tables 4 and 5). No significant difference was observed in FTW or TTW between patients with significant (≥3 mm) and nonsignificant (<3 mm) KT-1000 values (p > 0.05; Table 6). Additionally, there was no significant difference in isokinetic muscle strength between patients with and without KT-1000-detected side-to-side laxity (p > 0.05; Table 7).
Correlation between tunnel widening and functional scores.

FTW: femoral tunnel widening; TTW: tibial tunnel widening; IKDC: International Knee Documentation Committee.
Relationship between tunnel widening and Lysholm Knee Score.
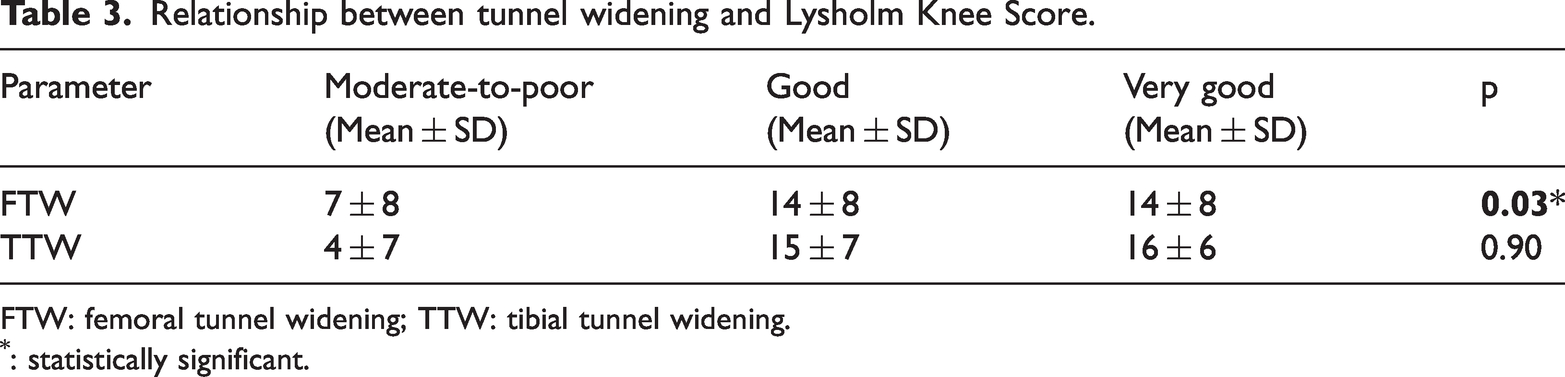
FTW: femoral tunnel widening; TTW: tibial tunnel widening.
: statistically significant.
Correlation between tunnel widening and Cybex II extension peak torque.
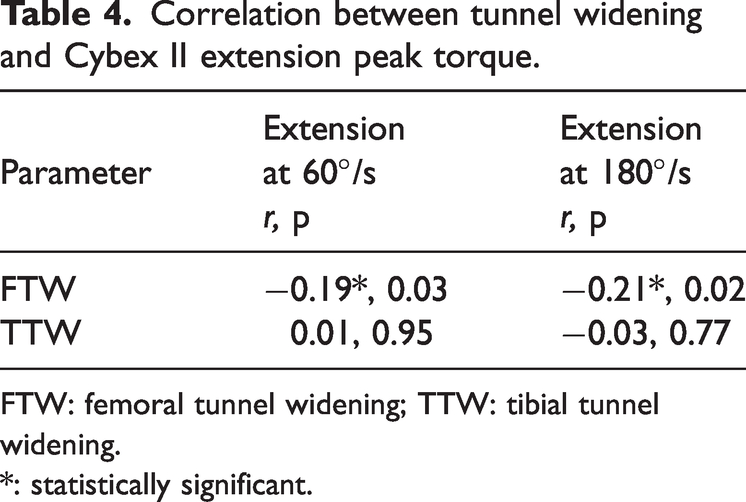
FTW: femoral tunnel widening; TTW: tibial tunnel widening.
*: statistically significant.
Correlation between tunnel widening and Cybex II flexion peak torque.
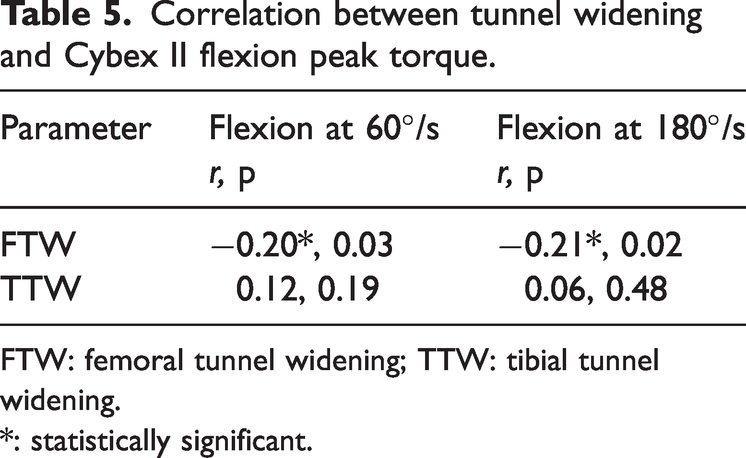
FTW: femoral tunnel widening; TTW: tibial tunnel widening.
*: statistically significant.
KT-1000 arthrometer measurements and tunnel widening.
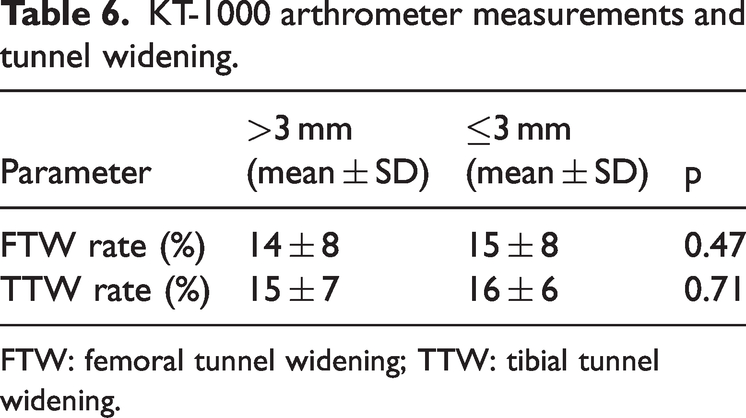
FTW: femoral tunnel widening; TTW: tibial tunnel widening.
Cybex II torque values stratified by KT-1000 measurements.

During the follow-up period, no cases of graft failure or revision surgery were recorded among the study participants. Therefore, no statistical analysis regarding the correlation between TW and clinical failure could be performed.
Inter-rater reliability for tunnel measurements was high, with an ICC of 0.829 (95% confidence interval (CI): 0.732–0.897), and intrarater reliability was excellent, with an ICC of 0.963 (95% CI: 0.855–0.988).
Discussion
The main result of our study is that there is a statistically significant decrease in quadriceps and hamstring peak torque values in the ID test after FTW. Another important result is that LKS is negatively affected in patients with FTW.
ACLR remains pivotal for restoring knee stability and function; however, TW—a frequently observed radiographic phenomenon—continues to challenge clinicians due to its ambiguous clinical implications.4,5,22 Although existing literature largely dismisses the association between TW and functional outcomes, our findings revealed a paradoxical relationship: although general TTW or FTW did not directly correlate with subjective functional limitations, FTW emerged as a critical determinant of adverse clinical outcomes. Specifically, patients with moderate-to-poor LKS scores exhibited significantly greater FTW (p < 0.05), suggesting that FTW can impair subjective knee stability and patient-reported function. Furthermore, our study is the first to objectively associate FTW with diminished quadriceps and hamstring strength using ID, a finding with profound implications for postoperative rehabilitation strategies.
We hypothesize that FTW disrupts graft–bone integration, exacerbating biomechanical instability and compromising neuromuscular recovery. This instability may manifest as reduced quadriceps activation and hamstring co-contraction, perpetuating a cycle of weakness and functional impairment. Notably, the extended follow-up period (median: 21.97 ± 8.64 months) and robust sample size (n = 120) in our study enhance the generalizability of these findings, addressing limitations of prior smaller cohorts with shorter observation windows. These results underscore the need to re-evaluate FTW not merely as a radiographic curiosity but as a potential biomarker for suboptimal recovery, warranting closer surveillance in high-risk patients.
It is critical to perform ACLR for successful clinical and functional outcomes with low complication rates. Despite various surgical techniques and the development of surgical instruments, ACLR is associated with many problems. 22 The occurrence of TW following ACLR is a common phenomenon and has been widely reported.4,5 TW affects graft maturation and bone–tendon healing and may cause difficulties in ACLR revision.23,24 Although enlargement is a common imaging finding, its clinical significance remains unclear. 25 A study reported that ACL reconstruction appeared to result in mild osteoarthritis in the long term in most of the patients, and only <33.2% patients developed a moderate-to-severe degree of knee osteoarthritis according to the IKDC radiographic score. 26 Our study revealed that TW had no effect on functional outcomes, in line with the literature. However, when assessing the clinical results, we found that FTW had a negative effect on quadriceps and hamstring strength. In the literature, we did not come across a study evaluating the relationship between FTW and ID results, which is an objective evaluation. At the same time, we believe that FTW can adversely affect the susceptibility to laxity and quadriceps strength, leading to low LKS scores. In terms of the follow-up period and sample size, our study offers stronger results than other studies in the literature.
The causes of TW after ACLR are multifactorial. The use of hamstring autografts or allografts is associated with graft–tunnel movement, accelerated rehabilitation, and improper graft placement. 27 After arthroscopic ACLR, TW is mostly observed in the hamstring graft and femoral tunnel compared with that in the tibia. 28 While opening the tibial bone tunnel, it has been shown that the use of angled (55°–65°) drill guides, which were previously determined in the literature and found to have the least stress in the tibial plateau, and opening them at a fixed angle minimize the stress created. 29 The tibial adhesion site of the ACL is more consistent than the femoral adhesion site. 30 We applied our study to patients who underwent reconstruction with hamstring tendon autograft. Femoral tunnel malposition is more surgeon-dependent than tibial tunnel malposition. We believe that the variability in FTW in our study occurred since the femoral tunnel was opened with the free hand technique during anatomical ACLR application to the patients, and the ACL footprint varies in the population.
Regarding the imaging method for bone tunnels, CT is known to be superior in terms of reliability. A study reported that CT measurements, instead of X-rays, were more accurate in TW measurements for correlation with clinical evaluation scales. 27 Another study reported that there were no reliable radiological parameters available that correlate with return to sport after ACLR. 31 Moreover, X-ray is prone to error because of variation caused by the inability to provide the correct AP/lateral position. In our study, we used the 3D reconstruction method, which shows the most appropriate TW measurement previously described in the literature.20,32 Using this software technique and the methodology for measuring tunnels, we aimed to evaluate our work in the most appropriate way. As the most sensitive tunnel measurement method, we used CT with 3D reconstruction and Cybex II device, which evaluates objective muscle strength, in our study. By choosing these examinations, we planned to minimize the margin of error in our study results.
A study reported that FTW had a statistically negative correlation with IKDC and LKS scores.26 We found a negative correlation between FTW and LKS score, but this was not statistically significant. In our study, we examined TW values with a KT-1000 arthrometer. We found that KT-1000 values (≤3 mm) were not related to TW. Although we detected laxity after TW, we found that this did not affect functional outcomes. These findings were consistent with the literature. However, we believe that this situation can have a negative effect on the functional results of the patient, especially because it causes a significant decrease in quadriceps and hamstring strength in patients with FTW.
In our study, TTW was found to have no effect on functional and clinical outcomes. According to our results, the effect of FTW on functional and clinical outcomes was more significant than that of TTW. Based on ID measurement, statistically significant decreases in extension and flexion values at 60°/s–180°/s were observed after FTW. Based on these findings, FTW measurement and ID are important in symptomatic patients who have undergone ACLR with low functional scores. We believe that these evaluations will help in planning the appropriate treatment modality and organizing the rehabilitation program. Although the strength deficits were subclinical and did not translate into inferior outcome scores or increased laxity, reduced thigh muscle strength can delay return-to-sport readiness and increase the risk of reinjury. Strength asymmetry, particularly in the quadriceps, has been shown to affect dynamic knee stability and functional performance, both of which are critical for safe return to high-demand activities. Therefore, the presence of FTW may warrant closer monitoring and more aggressive, individualized rehabilitation—especially emphasizing isokinetic strengthening and neuromuscular control—to ensure patients achieve functional criteria before resuming sports.
The most important limitation of our study is that it is a retrospective study. Second, there were no observed cases of graft failure or revision surgery during the follow-up period. As a result, we were unable to analyze potential correlations between FTW or TTW and clinical failure. This limits our ability to determine whether the observed morphological changes have long-term implications for graft integrity or joint stability. Further studies with larger patient populations and longer-term follow-up are warranted to explore the relationship between TW and postoperative graft failure. The fact that the number of patients included in the study is considerably higher than that in similar studies in the literature emerges as a strong aspect of our study. At the same time, the fact that our mean follow-up period is longer than that of many studies in the literature is important for the evaluation of medium-to-long–term follow-up of TW. Another important strength of our study is the use of ID, which is an objective clinical evaluation method, and an FTW measurement method in which the margin of error is minimized.
Conclusion
Although FTW and TTW were not significantly associated with clinical outcome scores or anterior laxity, an increase in FTW was negatively correlated with quadriceps and hamstring strength at both 60°/s and 180°/s. These results suggest that FTW contributes to subclinical functional deficits in muscle performance, even in the absence of overt instability.
Given these findings, incorporating targeted rehabilitation strategies for patients with FTW may be beneficial. Emphasis should be placed on progressive isokinetic strengthening of the thigh muscles, particularly the quadriceps and hamstrings, along with neuromuscular control and proprioceptive training. Monitoring of tunnel morphology via follow-up imaging and periodic strength testing should be considered to guide individualized rehabilitation and optimize long-term functional outcomes after ACLR.
Footnotes
Acknowledgements
None.
Author contributions
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors have no competing interest related to this study.
Ethics and consent to participate
The present study has been approved by the Institutional Review Board with the number 17073117-050.06. Informed consent was obtained from the patients.
Funding
This study received no funding.