
Abstract
The efficacy of sequential adjuvant chemotherapy after concurrent chemoradiotherapy in older patients with glioblastoma multiforme is limited. Previous studies have reported that controlling tumor recurrence by increasing the electric field intensity in the tumor region can extend the survival of older patients with glioblastoma multiforme. This report describes the case of a woman with glioblastoma multiforme in her early 60s from China who was initially admitted to Shenzhen People’s Hospital with impaired consciousness and limb weakness. Based on her medical history and magnetic resonance imaging findings, she was diagnosed with glioblastoma multiforme with subfalcine herniation. After undergoing decompressive craniectomy in addition to receiving concurrent radiotherapy and chemotherapy, she achieved long-term survival benefits by maintaining tumor electric field therapy.
Background
Glioblastoma multiforme (GBM) is a primary malignancy of the central nervous system, with an annual incidence of 3.2 per 100,000 people. 1 As the incidence of GBM increases with aging, it is more commonly observed in the older population. 2 The standard treatment regimen for GBM consists of maximally safe resection, followed by concurrent chemoradiotherapy (CCRT), and then sequential adjuvant chemotherapy. 3 Despite using multiple comprehensive treatment regimens for patients with GBM in clinical practice, early recurrence often occurs due to its highly aggressive and treatment-resistant nature. Consequently, patients with GBM typically have a median survival of only 14–16 months and a 5-year survival rate of ∼6.8%.1–4 Therefore, there is a pressing need to explore novel effective treatment options for this disease to improve patient outcome. Tumor-treating fields (TTFields) is a novel cancer therapeutic modality that mainly comprises electric field generators and noninvasive transducer arrays. The underlying principle is that the electric field generator can generate a specific alternating electric field. These low-intensity (1–3 V/cm) and intermediate frequency (100–300 kHz) electric fields are delivered through noninvasive transducer arrays and placed locoregionally around the anatomical region of the tumor.5,6 TTFields is designed to interfere with tumor cell mitosis, leading to cancer cell apoptosis and the inhibition of tumor growth. In addition, the TTFields array placement is adjusted according to the optimal anatomical characteristics for opposing tumor growth.5,6 A previous phase I clinical trial reported a skull reconstruction (SR) surgery technique for GBM, which involves creating burr holes and performing minor craniectomies above the tumor region to artificially induce partial skull loss. Moreover, this technique focuses a cancer suppression current onto the tumor while increasing the treatment dose. 7 As this technique has not been documented to cause any additional serious side effects, it has been proposed to be a viable method for controlling local tumor progression and prolonging patient survival.7,8 This report describes the case of a Chinese patient with GBM who underwent bone flap removal surgery, resulting in a loss of a 6 × 6-cm section in the right skull. This resulted in a closer connection between the scalp and brain tissue, reducing the shielding effect of the skull during the TTFields current delivery process, which had a similar effect to SR surgery. Both were designed to increase the current delivered to the local tumor area with the aim of improving the local tumor control rate. Therefore, the ultimate effects of this treatment method warrant further future research.
Case presentation
This case report is in accordance with the Case Report (CARE) guidelines. 9 Written informed consent was obtained from the patient’s family for the publication of case information and images. All patient details have been de-identified. In June 2020, a woman in her early 60s was admitted to Shenzhen People’s Hospital due to impaired consciousness and left lower extremity weakness. Magnetic resonance imaging (MRI) revealed multiple occupying lesions in the right frontotemporal lobe (Figure 1). The diagnosis was cerebral malignancy accompanied with subalpine herniation. The patient had no medical history of hypertension, diabetes mellitus, or hepatitis. During clinical assessment, the patient presented with a state of somnolence but was capable of responding to external stimuli and could independently execute the action of opening eyes. The pupils were of equal size on both sides, measuring approximately 2.5 mm in diameter, and they reacted appropriately to light. The patient’s communication was limited to single words, and she was unable to carry out complex command actions. No resistance was detected during the neck examination. All physiological reflexes were normal, and pathological reflexes could not be elicited. The surgeon performed an exploratory resection of the right frontotemporal lobe and decompressive craniotomy to reduce intracranial pressure and prevent life-threatening postoperative intracranial pressure elevation. Postoperative pathological analysis yielded the diagnosis of right temporal lobe glioblastoma (WHO grade 4; isocitrate dehydrogenase (IDH) wild-type) (Figure 1). Immunohistochemical analysis reported the following: methylguanine methyltransferase (MGMT; foci +) and Ki-67+ (∼50%). Genetic testing revealed the following: IDH1 R132 wild-type; IDH2 R172 wild-type; 1p/19q not missing; and MGMT promoter methylation (+) (Figure 2). Physical examination 20 days after surgery found the following: (a) the patient was conscious; (b) Karnofsky Performance Status (KPS) score of <60; and (c) right frontal lobe soft tissue bulging at the bone window. The neurological features were as follows: (a) the patient could not pronounce words clearly; (b) muscle strength in the left limb was grade III; (c) muscle tone in the upper limb decreased, whereas the muscle tone in the lower limb increased; (d) other neurological examinations did not reveal any other relevant symptoms; and (e) no abnormalities were detected following examinations of other organs. After the patient’s condition was stabilized, our team was allowed to offer her a comprehensive treatment plan. She started receiving CCRT in July 2020. Radiotherapy was delivered using volumetric modulated arc therapy using 6-MV X-rays. The gross tumor volume (GTV) included the T1 enhancement area and the surgical cavity, whereas the clinical target volume (CTV) was a 2-cm enlargement of the GTV, and the planned target volume (PTV) was defined as a 0.3-cm enlargement of the CTV. From day 1 of radiotherapy, concomitant chemotherapy with temozolomide (TMZ, 75 mg/m2/day) combined with bevacizumab (BEV, 10 mg/kg q2w) was administered to suppress angiogenesis and reduce intracranial edema. Due to the patient’s poor postoperative condition and the unclear efficacy of TTFields after craniectomy, simultaneous electric field therapy was not performed at the time. In August 2020, 1 month after CCRT, sequential adjuvant chemotherapy based on TMZ (6 cycles, 150–200 mg/m2/day for 1–5 days, every 28 days) was initiated. A follow-up brain MRI at 7 months after the end of CCRT showed stable tumor control (Figure 3). In addition, at the request of the patient’s family, in pursuit of superior treatment outcomes and based on the previous findings from a phase I study on the effects of SR + TTFields, 7 the patient was deemed eligible for TTFields therapy; subsequently, treatment was initiated in March 2021, with an average daily adherence rate of 88%.

Magnetic resonance imaging of the lesion. (a,b) Coronary T1-weighted post-gadolinium. (c,d) Coronary fluid-attenuated inversion recovery (FLAIR) image. (e) Hematoxylin–eosin stain, 4× magnification and (f) Hematoxylin–eosin stain, 20× magnification (f). Many heterologous cells, palisade-like necrosis, and prominent mitotic figures exist.

MGMT gene methylation was positively detected in gliomas using the pyrophosphate sequencing method (a), and DNA sequencing method was used to detect IDH1 R132 wild-type and IDH2 R172 wild-type (b,c).

Magnetic resonance imaging of the brain at 7 months after concurrent chemoradiotherapy (March 2021). (a,b) Coronary T1-weighted post-gadolinium image. (b,d) Coronary fluid-attenuated inversion recovery (FLAIR) image and (e,f) the patient underwent long-term tumor-treating fields (TTFields) therapy.
Since that time, the patient has undergone MRI follow-ups every 3 months and has also been subjected to routine blood tests, encompassing assessments of liver function, kidney function, and electrolyte levels. According to the response assessment in neuro-oncology criteria, 10 MRI efficacy evaluation during treatment showed stable disease, and no systemic severe toxicity was found. The patient did not require hormonal maintenance therapy, had an improved KPS score of 60, and was clinically stable.
Until August 2023, MRI revealed a new lesion in the right occipital lobe, suggesting tumor recurrence (Figure 4). The patient subsequently received 6 cycles of TMZ chemotherapy (150–200 mg/m2/day for 1–5 days, every 28 days). Although the MRI that followed indicated a reduction in the size of the lesion located in the right occipital lobe, regrettably, the MRI conducted in April 2024, revealed the presence of multiple small enhancing nodules within the brain, suggesting that the disease was advancing (Figure 4). Therefore the patient underwent secondary radiation therapy for these new lesions (5 Gy × 5 fractions), concurrently with BEV (10 mg/kg q2w). Over the entire duration of treatment, TTFields therapy has been administered consistently, and the patient has shown good tolerance and compliance with the treatment. The latest MRI, performed in October 2024, revealed a decrease in the enhancement of the lesions (Figure 4). To date, the patient has undergone TTFields therapy for over 43 months, with an overall survival (OS) of >52 months (Figure 5).

Follow-up magnetic resonance imaging of the brain. (a,b) Coronary and sagittal T1-weighted post-gadolinium image (August 2023). (c,d) Coronary T1-weighted post-gadolinium image (April 2024). (e,f) Radiotherapy plan of re-irradiation and (g,h) Coronary T1-weighted post-gadolinium image (October 2024).
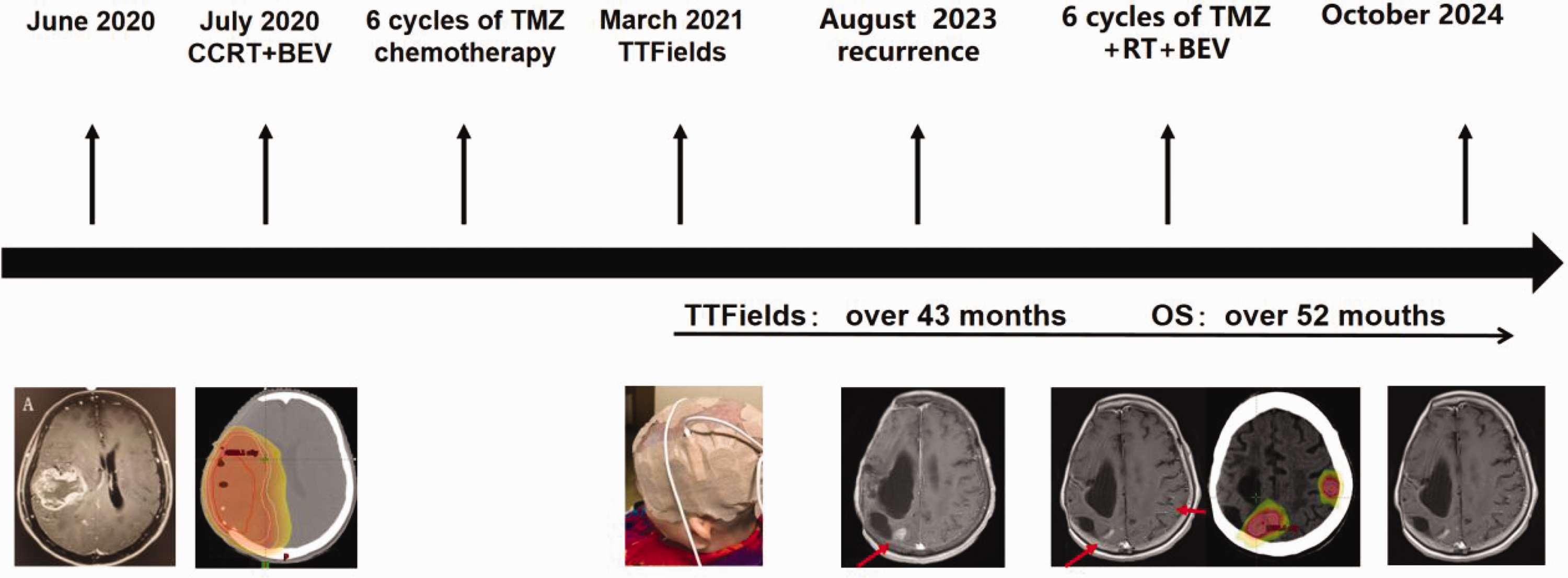
Patient treatment timeline.
Discussion
TTFields is currently used in numerous medical institutions across China as an adjunct to the standard treatment protocols for GBM, including surgery, radiotherapy, chemotherapy, and targeted therapy. 11 Its efficacy has been previously validated in two phase III randomized controlled trials, namely EF-11 and EF-14.12,13 Notably, EF-14 trial used tumor electric field therapy in conjunction with TMZ. This combined therapeutic approach for newly diagnosed glioblastoma prolonged patient OS from 16 to 20.9 months and the 5-year OS rate improved from 5% to 13%. 13 This clinical trial study also revealed that patients with good compliance experienced a significantly prolonged median survival time. When patients adhered to wearing the device for over 22 hours daily, the 5-year survival rate was observed to increase to 29.3%. 14 Regarding side effects, TTFields did not result in any notable systemic or severe toxicity. However, the most common adverse event was mild-to-moderate dermatitis at the site of transducer array placement, such as ulcers and skin infections. Treatment strategies for these events typically included topical corticosteroid and antibiotic therapy. 15 Further research on TTFields is underway to exploit the advantages of this noninvasive treatment technique.
Korshoej et al. 16 proposed that the conductivity of the brain tissue structure can affect the local field strength distribution. By changing the skull structure, the shielding effect of the skull can be effectively reduced, creating a low-resistance current path for TTFields. This in turn renders it easier for TTFields to deliver electric fields into the cerebrospinal fluid, which is more conductive than other original head tissues, such as the skin and bone, and can increase the electric field strength in the superficial tumor region by 60%–70%, significantly increasing the tumor suppression effect.16,17 A previous phase I clinical trial in which patients were treated with recurrent GBM with SR + TTFields found that the median progression-free survival (PFS) and OS of 11 patients were 4.6 and 15.5 months, respectively, with a 12-month survival rate of 55% and an overall response rate of 9.1%. In addition, the treatment-related toxicities observed were found to be within acceptable limits. 7 These survival results suggest promising safety and efficacy of SR + TTFields for GBM.5,17 Another previous phase II study of SR + TTFields for GBM is ongoing to clarify its efficacy and potential impact. 18 In summary, craniotomy is similar to SR surgery, which is in turn comparable to decompressive craniectomy. All three techniques are designed to alter the local electric field strength by altering the cranial structure to achieve optimal tumor suppression.
It has been frequently reported that individualized multimodal therapy can meet the therapeutic expectations of patients more adequately. Previous studies have shown that a number of patients with GBM can tolerate higher doses of hypofractionated radiotherapy, which reduces the risk of advanced radionecrosis and improves their quality of life.19,20 Furthermore, re-irradiation emerges as a viable treatment option for patients experiencing recurrent diffuse lesions. Techniques such as stereotactic radiosurgery or stereotactic radiotherapy are used for individuals with small lesions. 21 In addition, assessment of the qualitative status of MGMT promoter methylation has been previously reported to be one of the indicators of a good prognosis from high-grade GBM by several studies. 22 Based on these abovementioned findings, Perry et al. 23 used short-course macrofractionated radiotherapy combined with TMZ and compared it with standard concurrent radiotherapy, which found that the median OS in the experimental group could be extended to 13.5 months, which is 5.8 months longer compared with that in the standard concurrent radiotherapy group. Therefore, Perry et al. 23 suggested that the use of short-course radiation combined with TMZ is expected to prolong the survival of patients with poorly tolerated glioblastoma who exhibit methylated MGMT promoters. In addition, previous studies have shown that angiogenesis plays a crucial role in the growth, invasion, and metastasis of GBM. 24 Specifically, BEV blocks vascular endothelial growth factor activation. It has been shown to reduce vascular permeability and edema, thereby alleviating radiotherapy and chemotherapy symptoms. Although it can be used to support patients as a supplement to radiotherapy and improve PFS, it is not known to significantly improve OS.24–26
A small proportion of patients with GBM have achieved long-term survival, where favorable prognostic factors include younger age, good physical condition, complete tumor resection, MGMT promoter methylation, and standard Stupp treatment. In the current case, the tumor lesion was situated near the midline, and its complete excision could potentially compromise structures within critical functional regions of the brain. Furthermore, a previous study indicated that individuals younger than 70 years are advised to receive conventional fractionated radiotherapy. 27 However, the KPS score of the current case before radiotherapy was <60, suggesting she would be unlikely to endure high-dose radiotherapy. To ensure the patient’s safety, short-course and large-fractionated radiotherapy were used during the first and second courses of treatment. Overall, the present case has exhibited characteristics of long-term survival, with her OS reaching over 52 months since diagnosis, significantly surpassing the reported median survival time of 15 months. This may be attributed to the combined effect of TTFields following craniectomy, which enhances the electric field intensity within the localized tumor region and thereby boosts the antitumor efficacy of TTFields. Although generalizability is inherently limited by a single case, this case highlights the potential of combining TTFields with SR surgery.
Conclusions
To the best of our knowledge, this case report documents the first instance in China of an older patient diagnosed with GBM who underwent decompressive craniectomy in combination with TTFields therapy, resulting in a favorable outcome. Unfortunately, the surgery caused significant damage to the patient’s neurological function. According to the current case, patients with GBM and a poor prognosis may benefit from personalized combination therapy, including TTFields combined with craniectomy, short-course macrofractionated radiotherapy, chemotherapy, and targeted therapy. Therefore, further studies are required to improve and assess the efficacy of TTFields.
Footnotes
Acknowledgements
We would like to express our gratitude to the Deepseek team. During the preparation of this work, we used Deepseek to enhance the language. After using this tool, we reviewed and edited the content as necessary and take full responsibility for the content of the publication. Moreover, we did not use AI tools in our research methods. We also acknowledge the patient and her family for agreeing to the publication of the case.
Authors’ contributions
LZH, YHL, WLJ, SMQ, and ZJZ treated the patient. YHL and WLJ wrote the paper. All authors contributed to the article and approved the submitted version.
Availability of data and materials
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declare that this study was conducted without any business or financial relationships that could be perceived as a potential conflict of interest.
Ethics approval and consent for publication
Ethical review and approval were not required for this study on a human participant in accordance with the local legislation and institutional requirements. Written informed consent was obtained from the patient’s family for the publication of case information and images. We have de-identified all patient details.
Funding
No funding was received.