
Abstract
Endometriosis is an uncommon condition, and its occurrence in the urachus is exceptionally rare. This case report highlights the extreme rarity of bladder endometriosis involving the urachal area. To the best of our knowledge, no such cases have been previously reported in the literature. The clinical presentation and imaging findings of this condition are extremely similar to those of urachal carcinoma, which makes the differential diagnosis particularly challenging. In this case, a 34-year-old woman presented with significant bladder irritative symptoms during menstruation. Imaging revealed a mass in the urachal region, but its characteristics remained uncertain. Cystoscopy showed only bladder compression, and the patient ultimately underwent robot-assisted laparoscopic partial cystectomy. Postoperative pathology confirmed the diagnosis of bladder endometriosis. This case underscores the importance of considering bladder endometriosis in the differential diagnosis of masses in the urachal area, particularly when they resemble urachal cancer. Early surgical intervention and histopathological confirmation are essential to prevent disease progression.
Background
Endometriosis is defined as the growth, infiltration, and recurrent bleeding of endometrial tissue (including glands and stroma) outside the uterine lining and myometrium, forming nodules and masses that can cause pain and infertility. 1 The involvement of the urinary system in endometriosis is rare, accounting for approximately 1%–2% of the cases, with 85% of these occurring in the bladder. 2 A review of the literature revealed no reported cases of bladder endometriosis (BE) involving the urachus. Therefore, owing to the low incidence of BE, differential diagnosis with urachal cancer is particularly challenging.
Herein, we present a case of BE in a middle-aged woman to provide further insights into this rare condition.
Case presentation
A 34-year-old woman presented with significant bladder irritative symptoms during menstruation without visible hematuria or notable abdominal or flank pain. Abdominal computed tomography (CT) at a local hospital indicated a mass at the urachal site, with a possible urachal malignancy. She was referred to our hospital for further evaluation and treatment. Since the onset of symptoms, her mental state and appetite were optimal, bowel movements were normal, and there was no recent weight loss. She had a history of two cesarean sections. Her menstrual cycle and characteristics were normal; her last period started on 3 September 2024. Family history revealed that her mother had ovarian cancer with metastasis to the colon. The patient’s remaining medical history was unremarkable. The reporting of this study conforms to the Case Report (CARE) guidelines. 3
Upon admission, a series of investigations were conducted to clarify the nature of the mass. Pelvic plain and contrast-enhanced scans indicated a mass in the anterior bladder wall and left rectus abdominis, along with an enhancing nodule in the right rectus abdominis. Based on these findings, endometriosis was considered (Figure 1). Cystoscopy showed bladder dome compression, suggesting an abdominal mass. Urinary tract ultrasound detected a solid nodule above the bladder, measuring approximately 28 × 22 mm, raising suspicion of endometriosis, urachal mass, or other pathology; this mass needed to be correlated clinically. Another solid nodule above the bladder was likely an endometriotic lesion (Figure 2). Transvaginal ultrasound revealed a small solid nodule in the uterine wall, and the level of the tumor marker CA123 was elevated at 26.2 U/mL. Based on her clinical presentation and imaging findings, a preliminary diagnosis of urachal mass, likely endometriosis, was made, and robot-assisted laparoscopic partial cystectomy under general anesthesia was planned. Final pathological assessment confirmed endometriosis (Figure 3). The patient was followed up for 6 months postoperatively, with no lower urinary tract symptoms (LUTS) observed and no recurrence of the mass detected on examination.

Pelvic plain plus contrast-enhanced CT. (a) Plain CT; (b) CT arterial phase; (c) CT venous phase and (d) CT delayed phase. CT: computed tomography.

Urinary system ultrasound.
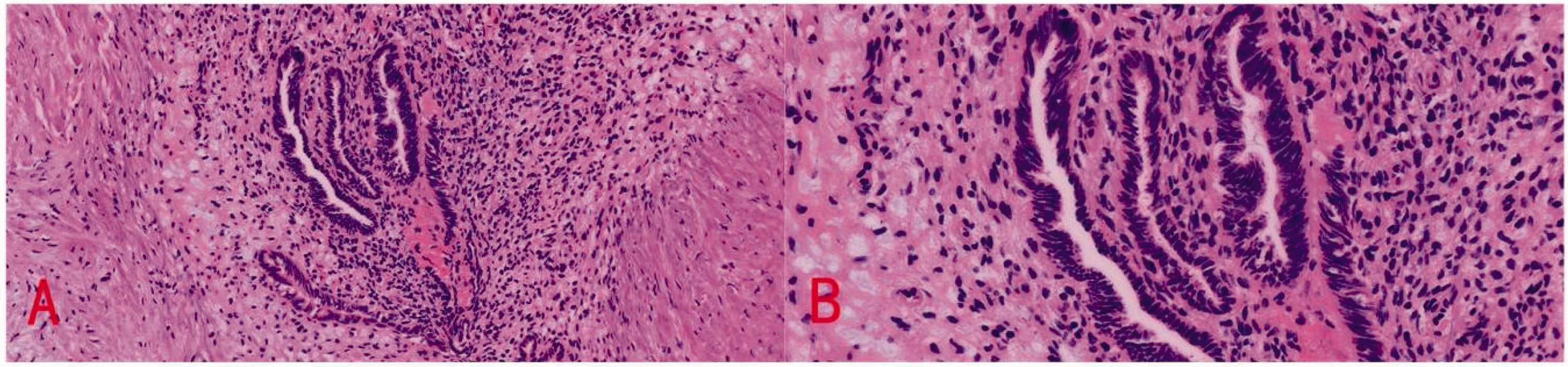
Postoperative pathology of the urachal mass showing endometrial glands and stroma. (a) H&E (20×) and (b) H&E (40×). H&E: Hematoxylin and eosin.
Discussion
Endometriosis is defined as the presence of functional endometrial glands and stroma outside the uterine cavity. It affects approximately 10% of women of reproductive age. The most common sites of endometriosis include the ovaries, ovarian fossa, uterosacral ligaments, rectovaginal space, and rectouterine space. Urinary tract involvement is rare, accounting for approximately 1% of all endometriosis cases. BE is the most common form of urinary tract endometriosis, occurring in 70%–85% of cases. 4 Endometriosis located at the urachus has not been reported in the existing literature, making it even rarer. Because of the striking similarity of BE to the similarly rare urachal carcinoma (UrC) in both clinical symptoms and auxiliary examination findings, BE poses significant diagnostic challenges.
BE is characterized by the ectopic presence of endometrial tissue, glands, and stroma that invade the bladder wall at various depths. The dome and posterior aspects of the bladder are the most frequently affected areas. In women without a history of gynecological surgery, it can present as a primary lesion. However, it may also occur secondarily following pelvic surgery, primarily after cesarean deliveries and is rarely observed after total hysterectomy. 4 Endometriosis can also occur in relatively rare anatomical sites. For instance, Liu Kai et al. reported a case of hepatic endometriosis in a primiparous woman, 5 while Yohannes documented a case of ureteral endometriosis. 6 These reports highlight the unusual locations where ectopic endometrial tissue can be found. In most cases, BE is associated with LUTS such as dysuria, urinary frequency, and visible hematuria, which typically occur during menstruation, as well as less common symptoms such as urinary urgency, bladder pain, and even acute urinary retention. 7 These symptoms may worsen during menstruation and can present in a noncyclical manner. Urine cultures and cytology tests are generally negative.
BE occurring at the urachus is associated with the following theories: (a) retrograde menstruation theory, which suggests that endometrial tissue flows backward through the fallopian tubes into the abdominal cavity during menstruation and is implanted at this site; (b) coelomic metaplasia theory, which proposes that under certain stimuli, peritoneal epithelium can transform into endometrial-like tissue; (c) lymphatic or hematogenous dissemination theory, which posits that endometrial tissue can be transferred to distant sites through blood or lymphatic circulation; and (d) embryonic remnant theory, which suggests that residual embryonic tissue during development may differentiate into endometrial tissue under specific conditions. These mechanisms may act individually or synergistically to contribute to the presence of ectopic endometrial tissue in atypical sites, such as the urachus.8–9
UrC is an extremely rare malignant tumor, accounting for approximately 0.35%–0.70% of bladder tumors. It is more commonly found in men. In the early stages, patients with UrC present with no specific clinical symptoms. As the disease progresses, hematuria may develop. Furthermore, in later stages, abdominal pain or mucus in the urine may occur. 10
Both BE and UrC affect the urinary tract and present with varying degrees of urinary symptoms. However, UrC is primarily characterized by hematuria, while BE symptoms are often associated with the menstrual cycle. In the present case, the patient had a history of two cesarean sections and exhibited typical symptoms of urinary frequency, urinary urgency, and dysuria during menstruation. These medical histories suggest that the patient was more likely to have BE.
When evaluating BE, transabdominal and transvaginal ultrasound are considered first-line imaging methods owing to their accuracy, safety, and cost-effectiveness. 11
Pelvic CT and magnetic resonance imaging (MRI) can serve as second-line imaging modalities for assessing BE. In cases where malignancy is suspected, CT and MRI are regarded as more reliable, offering higher contrast and resolution compared with ultrasound, thus better visualizing the bladder layers and tissue characteristics and possessing superior multiplanar capabilities. 12 Cystoscopy is a diagnostic procedure widely used to accurately localize BE; it can estimate the distance between the ureteric orifice and the margin of BE to plan the most appropriate surgical approach. It can also be used to mark the margins of BE for easier visualization during subsequent laparoscopic excision. 13 Postoperative histopathological results can confirm the diagnosis by demonstrating the presence of endometrial glands in the bladder wall.
Imaging plays a crucial role in the diagnosis of UrC. Ultrasound is a screening tool, with typical findings including an irregular hypoechoic mass in the anterior bladder wall, frequently accompanied with patchy blood flow signals. CT and MRI are useful in assessing local infiltration and lymph node involvement as well as detecting distant metastases. Cystoscopy typically shows polypoid or ulcerative lesions on the dome or anterior wall of the bladder in UrC cases. 14 Urine cytology and tumor marker levels can also support the diagnosis of UrC.
In this case, cystoscopy results were atypical, showing only signs of pressure on the dome. Pelvic CT with contrast indicated a mass in the left rectus abdominis and an enhancing nodule in the right rectus abdominis, with the nature of the mass yet to be determined. The atypical imaging findings contributed to the uncertainty in the diagnosis of this case as they closely resembled the imaging characteristics of urachal cancer, making the differential diagnosis challenging. Ultimately, intraoperative pathology of the mass confirmed the diagnosis of BE.
Once the diagnosis of BE is established, treatment needs to be individualized based on the patient’s age, severity of symptoms, extent of the disease, number of pregnancies, and associated pelvic conditions. Clinical management may involve conservative measures, hormonal therapy, and surgical intervention. 4 The primary goal of surgery is the complete excision of bladder lesions. Current surgical approaches for treating BE primarily include transurethral resection of bladder tumors, open/laparoscopic (robot-assisted or nonrobot-assisted) partial cystectomy, and cystoscopic combined open/laparoscopic/robotic approaches. Partial cystectomy is a method that preserves bladder function while completely eliminating the extent of BE, including full-thickness resection of the lesion and surrounding bladder wall. 15 There is currently no standardized treatment protocol for UrC. Treatment options including surgery, chemotherapy, radiotherapy, targeted therapy, and immunotherapy have been explored. Among these, surgical resection remains the primary treatment approach, including partial cystectomy or radical cystectomy. In this case report, surgical treatment was ultimately chosen, with the procedure being robot-assisted laparoscopic partial cystectomy. Follow-up imaging at 6 months postoperatively revealed no signs of tumor recurrence.
The preoperative differential diagnosis between BE and malignant tumors requires a comprehensive approach, including medical history, clinical symptoms, imaging studies, and serum biomarker testing. Endometriosis is often associated with menstrual irregularities, pelvic pain, and infertility, whereas malignancies may present with persistent abdominal pain, weight loss, and systemic symptoms. Imaging modalities such as ultrasound and MRI are helpful in identifying typical endometriotic lesions (e.g. endometriomas), whereas malignant tumors usually appear with irregular margins and invasive growth patterns. The levels of serum markers such as CA-125 are frequently elevated in endometriosis, but they lack specificity; thus, these marker levels should be interpreted in conjunction with other clinical findings. BE is extremely rare among patients with endometriosis and is prone to misdiagnosis and missed diagnosis. In this case, the lesions occurred at the urachus, closely resembling the characteristics of urachal cancer. Distinguishing between these two conditions is particularly difficult based solely on clinical presentation, imaging findings, and laboratory tests. This case report suggests that when it is challenging to differentiate these two diseases preoperatively based on disease characteristics, intraoperative excision of the lesion with frozen section pathology may help confirm the diagnosis, guiding whether further resection of additional tissue or structures is necessary. This is because both diseases primarily require partial cystectomy as a treatment method. However, more clinical cases are needed to support this conclusion.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
Jiale Deng was primarily responsible for literature search and organization as well as drafting of the manuscript. Guanqun Wang participated in patient management, assisted in surgeries, and followed up with the patients. Yu Yang was responsible for editing the manuscript and organizing the case data. Mengying Liao performed the pathological examination of the tumor in this case. Liangkuan Bi assisted in editing the case presentation section of the article. Benlin Wei conducted a literature review and provided guidance and revisions for the manuscript. All authors have read and approved the final manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Clinical trial number
Not applicable.
Consent for publication
The patient’s written informed consent was obtained before preparing the case report.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
Not applicable.
Funding
Not applicable.