
Abstract
Bilateral Tessier no. 7 clefts are rarely reported in the literature. Here, we describe the presence of accessory maxilla with supernumerary teeth in a patient who exhibited bilateral Tessier no. 7 clefts; the diagnosis was established based on the patient’s history, clinical presentation, and computed tomography images. A review of the available literature revealed 24 patients with Tessier no. 7 clefts from 2000 to 2020, including our patient. The most common clinical manifestation in patients with Tessier no. 7 clefts comprises bilateral facial clefts. Additionally, Tessier no. 7 clefts are more frequently found in boys or men, rather than in girls or women. The presence of an accessory maxilla with supernumerary teeth in a patient with bilateral Tessier no. 7 clefts is extremely rare. Early detection of craniofacial abnormalities is important, because it may influence patient prognosis and management.
Keywords
Introduction
Craniofacial clefts are uncommon congenital deformities. The etiology of craniofacial clefts is unknown; they presumably occur as a result of genetic predisposition and environmental factors (e.g., infection, medication, and radiation). 1 The exact incidence is unclear, although craniofacial clefts are estimated to be present in 1.4 to 4.9 of 100,000 births.1–3 Currently, there is no universal classification for orofacial and craniofacial clefts. The Tessier clefting system is a commonly used classification approach, based on anatomic and descriptive features. This classification assigns numbers (1–30) to various sites of clefting, depending on their anatomic relationship with the sagittal midline. 4 , 5 Tessier no. 0 (59.5%) is the most common type of craniofacial cleft, whereas Tessier no. 8, 13, and 30 are the rarest types of clefts. 1 , 6
Tessier no. 7 clefts are uncommon, comprising 5.5% to 13.9% of all clefts. 6 They are characterized by macrostomia, facial muscular diastasis, and abnormalities of the maxilla and zygomatic bone. 6 The exact etiology of these clefts has not yet been determined; they may arise from failed fusion of the embryonic mandibular and maxillary process at the first pharyngeal arch. 7 Tessier no. 7 clefts might be associated with other anomalies, such as an accessory maxilla or mandible. The terms “accessory maxilla” and “maxillary duplication” refer to a rare clinical entity that is characterized by the presence of extra bone, lying posterior to the maxillary tuberosity. 8 The accessory maxilla is presumably caused by abnormal growth of the zygomatic arch and is often associated with facial clefts, including Tessier no. 7 clefts. However, the presence of an accessory maxilla in a patient with a Tessier no. 7 cleft is extremely rare. To the best of our knowledge, there have been four reported cases in the literature.7–10 Here, we describe the presence of an accessory maxilla in a 25-year-old man with bilateral Tessier no. 7 clefts.
Case report
In March 2018, a 25-year-old man with a history of bilateral Tessier no. 7 clefts was referred to the First Affiliated Hospital of Anhui Medical University for evaluation and treatment of an enlarged asymptomatic mass involving supernumerary teeth on the right posterior maxilla, which he had noticed 10 years prior to referral. The patient’s medical history included surgical repair of bilateral Tessier no. 7 clefts when he was 15 years old. He did not take any regular medications and supplements; additionally, he did not smoke and rarely drank alcohol. He reported no family history of facial deformities or inherited diseases.
Extraoral examination revealed no regional lymphadenopathy or swollen salivary glands. The patient’s right zygomatic bone was more prominent than his left zygomatic bone. Although surgical scars were noted at both commissures, the patient’s mouth opening was not limited by the presence of scar tissue (Figure 1). He exhibited no abnormalities in the external and middle ears. Intraoral examination revealed an outgrowth of bone with supernumerary teeth on the right posterior maxilla (Figure 2). With the exception of two narrow mucosal grooves on the right posterior maxilla, no alveolar cleft was observed. Teeth 13 and 24 were absent. The remaining oral structures were normal.

Clinical photo showing facial asymmetry.

Intraoral photo showing right posterior accessory maxilla with supernumerary teeth (black arrows: two mucosal grooves; red arrow: supernumerary teeth).
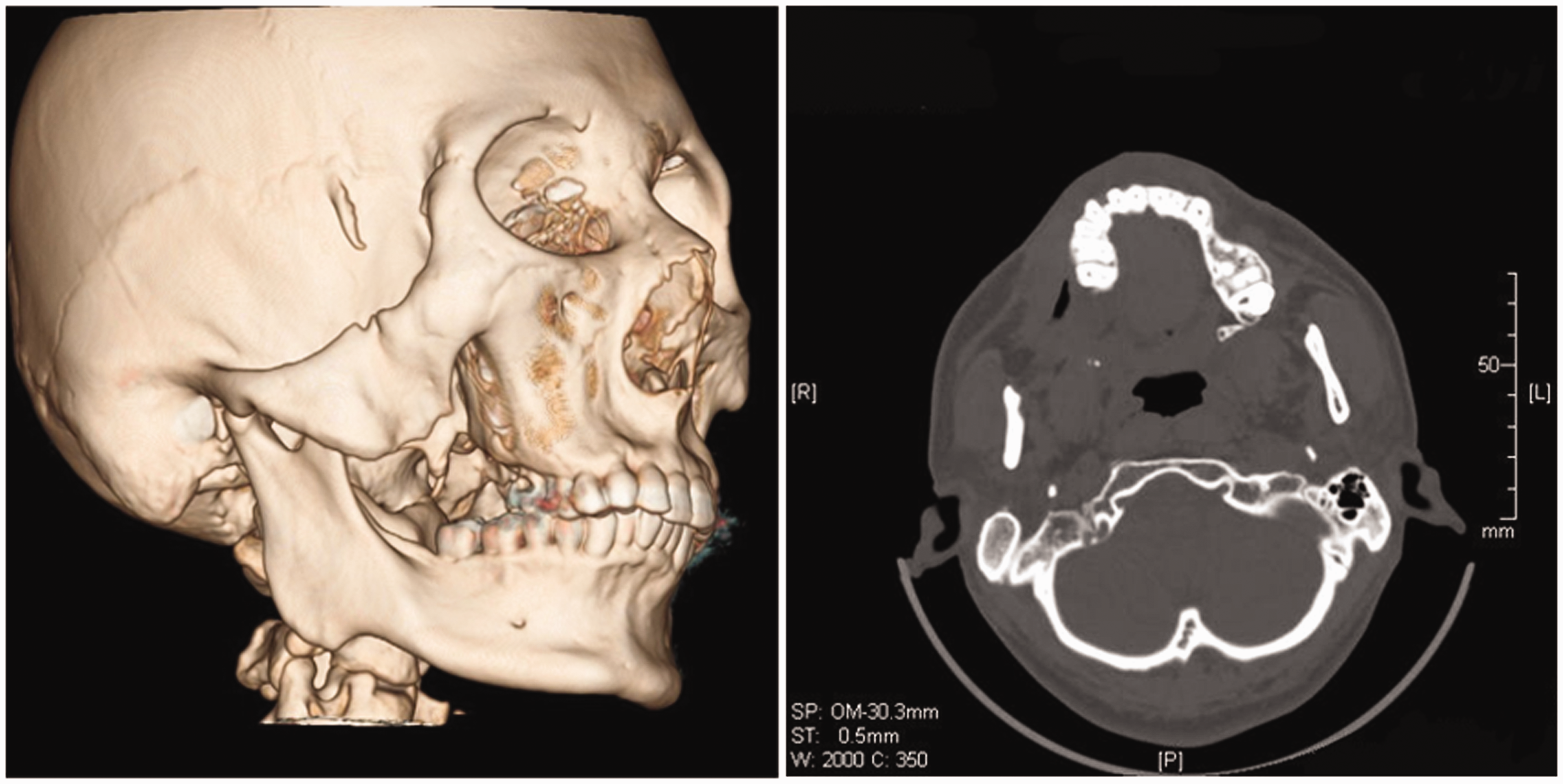
Panoramic radiography and computed tomography scans of the patient’s craniomaxillofacial skeleton also revealed an outgrowth of bone with supernumerary teeth, which appeared to arise from the right posterior maxilla; this outgrowth extended from the inferior border of the right zygomatic bone to the maxillary tuberosity. In addition, a gap was observed between the normal maxilla and the outgrowth of bone on the right side (Figure 3). Based upon the patient’s history, clinical findings, and computed tomography findings, a diagnosis of accessory maxilla with bilateral Tessier no. 7 clefts was made.

Preoperative computed tomography images. (a) Three-dimensional reconstruction computed tomography scan (black arrow: bony segments extending from inferior borders of right zygomatic bone to maxillary tuberosity; red arrow: bony gap between normal maxilla and teeth-bearing bony segments on right side). (b) Axial view of computed tomography scan (red arrow: high-density mass at right posterior maxillary region).
Surgical reconstruction was performed with the patient under general anesthesia. An angular incision was made and a mucoperiosteal flap was raised. Massive sclerotic bone was found between the posterior maxilla and the zygomatic bone. The accessory maxilla with supernumerary teeth was surgically removed; the excised specimen measured 4.5 cm × 3.0 cm × 2.0 cm (Figure 4). No bone graft was required, and the maxillary sinus remained intact during the surgery. Subsequent histopathological analysis revealed tooth-like structures, osseous tissue, and fibrous connective tissue in the excised specimen (Figure 5); no abnormal cells were found. By the 3-month follow-up examination, the wound had healed completely (Figure 6). The patient did not report any postoperative complications. Both postoperative computed tomography and panoramic radiography scans showed no signs of local recurrence (Figure 7).

Measurement of excised specimen showing size of 4.5 × 3.0 × 2.0 cm.

Histopathological assessment of excised specimen (hematoxylin and eosin stain) showing tooth-like structures, osseous tissue, and fibrous connective tissue.

Postoperative intraoral photo of right maxillary region showing complete wound healing.
Postoperative three-dimensional reconstruction and axial view computed tomography images showing no signs of local recurrence.
Ethical approval was obtained from the local ethics committee (approval no. 20190127) for treatment and publication of this report. Written consent was obtained from the patient for treatment and publication of this report.
Discussion
It is important to examine fetal craniofacial structure during prenatal examinations because abnormalities involving these structures may suggest the presence of syndromes, chromosomal abnormalities, infectious diseases, or metabolic disorders. 11 Prenatal ultrasounds (e.g., two-dimensional, three-dimensional, or four-dimensional ultrasound) are accurate, reliable, and non-invasive examination tools that can be used for detection of craniofacial abnormalities. Current international guidelines recommend routine mid-trimester ultrasound scans for evaluation of the fetal face including the upper lip, median facial profile, orbits, nose, and nostrils. 12
This report described a man with bilateral Tessier no. 7 clefts who presented for treatment of a right accessory maxilla. Thus far, the etiology of Tessier no. 7 clefts is unclear; it may involve amniotic membrane syndrome, failed maxillary fusion of the first branchial arch, or failed mesodermal migration. 8 , 9 , 13 Hard and soft tissue deformities are present in patients with Tessier no. 7 facial clefts. 6 , 13 The hard tissue abnormalities are characterized by deformation of the cranial base, glenoid fossa, sphenoid, condyle, coronoid process, mandibular ramus, posterior maxilla, alveolar process, and alveolar process, as well as the absence of zygomatic arch and maxillary cleft in the molar region; deformation of the maxillary tuberosity and pterygoid process are also observed. The soft tissue abnormalities are characterized by macrostomia, external and middle ear abnormalities, and temporalis abnormality, as well as sporadic abnormalities of the parotid gland and cranial nerves 5 and 7.
In the available literature, 24 patients with Tessier no. 7 clefts have been described from 2000 to 2020, including our patient. The clinical findings of these patients are presented in Table 1. 7 , 9 ,13–32 Among the 24 patients, 12 were male patients and eight were female patients; sex could not be identified in four patients. The most common clinical manifestation of Tessier no. 7 clefts was bilateral facial clefts, which was present in 66.7% of the patients. Syndromes (i.e., Goldenhar Syndrome, Dandy-Walker Syndrome, Amniotic band syndrome, and posterior fossa brain malformations, hemangioma, arterial lesions, cardiac abnormalities, and eye abnormalities [PHACE] syndrome) were present in five patients. Three patients exhibited a unilateral accessory maxilla, two exhibited bilateral accessory maxillae, and one exhibited a right accessory mandible. Supernumerary teeth were present in five patients with jaw duplication; alveolar cleft and mandibular dysplasia were present in seven patients. All patients were described in case reports. Most patients had a prenatal diagnosis and had undergone reconstructive surgical treatment.
Tessier no. 7 clefts cases from 2000 to 2020.

Abbreviations: F, female; M, male; N/A, information not available; PHACE, posterior fossa brain malformations, hemangioma, arterial lesions, cardiac abnormalities, and eye abnormalities.
Duplication of jaws with supernumerary teeth can occur in maxilla or mandible, either as an accessory outgrowth or a complete jaw. 7 The exact incidence of jaw duplication is unclear; it is estimated that 1 in 80,000 births in the general population may be affected, with a higher incidence in boys than in girls 9 and a higher incidence in the maxilla than in the mandible. 8 , 33 The majority of published reports described unilateral involvement; fewer than 20% of patients exhibited bilateral involvement. Maxillary duplication is a rare congenital condition that is often accompanied by cleft lip, palate, or other craniofacial clefts. 7 , 8 , 13 , 34 To the best of our knowledge, only a few instances of maxillary duplication have been described in the literature.34–37 Accessory maxilla as a type of maxillary duplication has often been reported with facial clefts; isolated maxillary duplication with no other anomalies has also been described. 30 ,38–41
Early detection of jaw duplication is important because it could influence the growth of the craniomaxillofacial region (e.g., tooth eruption and facial growth). Thus, we recommend early referral to tertiary centers and regular follow-up of affected patients to rule out the presence of other craniofacial anomalies and syndromes.
Conclusion
The most common clinical manifestation in patients with Tessier no. 7 clefts comprises bilateral facial clefts. Additionally, Tessier no. 7 clefts are more frequently found in boys or men, rather than in girls or women. The presence of an accessory maxilla with supernumerary teeth in a patient with bilateral Tessier no. 7 clefts is rare. This report emphasizes that early detection of craniofacial abnormalities is important, because it may influence patient prognosis and management.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
We thank Anhui Provincial Higher Education Talent Project, gxyq 2018010 and Natural Science Research Project of Anhui Higher Education Institutions, KJ2018A0193, for the support of the publication cost.