
Abstract
Neurofibromatosis type 1 is an autosomal dominant disorder. The vasculopathy of neurofibromatosis type 1 may rarely comprise stenosis, occlusion, aneurysm, pseudoaneurysm, and arteriovenous deformity, and it often presents as rupture of an undiagnosed lesion, which highly increases mortality in young patients with neurofibromatosis type 1. A female patient in her early 30s who had neurofibromatosis type 1 presented to our hospital with extensive and progressive bleeding of a ruptured renal artery pseudoaneurysm caused by trauma. Complete total embolization of the renal artery was performed using several microcoils and a mixture of n-butyl cyanoacrylate and iodized oil. Despite combined endovascular and surgical management tailored to the patient’s condition, she died from uncontrolled bleeding. Endovascular treatment is widely regarded as a safe and less invasive option for managing vascular complications in neurofibromatosis type 1. However, it may be insufficient in rapidly progressive cases. Considering the vascular fragility and recurrence of hemorrhagic shock, earlier surgical intervention, including nephrectomy, should have been more strongly considered. This case highlights the limitations of repeated endovascular management alone and suggests that prompt surgical exploration is warranted when pseudoaneurysm rupture is suspected, even in seemingly stable patients. Ultimately, this case underscores the need for heightened clinical vigilance and early surgical decision-making in the treatment of neurofibromatosis type 1 and rapidly evolving vascular injuries.
Introduction
Neurofibromatosis type 1 (NF1), also known as von Recklinghausen disease, is a common autosomal dominant disorder characterized mainly by multiple café au lait macules, benign neurofibromas, and iris hamartomas. 1 Patients with NF1 rarely develop cardiovascular disease, including vascular stenosis, occlusion, aneurysm, pseudoaneurysm, rupture, and fistula formation, and most of them remain asymptomatic. However, vascular disease often presents as rupture of undiagnosed lesions, which significantly increases mortality in young patients with NF1.2–4
Most cases involve the renal arteries, which tend to be stenotic rather than aneurysmal. 2 Renal artery aneurysms are usually asymptomatic, but their rupture can be fatal. 5 There have been a few reports of spontaneous rupture of a renal artery aneurysm in patients with NF1,6–8 and endovascular management has been reported as a safe and effective treatment for aneurysm in NF1.7,8
To the best of our knowledge, there has been no report of traumatic renal arterial injury in a patient with NF1 to date, and the direction of treatment and prognosis have rarely been investigated. Herein, we report our experience with a case of extensive, progressive lethal bleeding from a ruptured renal artery pseudoaneurysm caused by traumatic injury in a patient with NF1. We also discussed optimal treatment strategies for this condition.
Case presentation
In May 2019, a female patient in her early 30s who had NF1 presented to Chungbuk National University Hospital (Cheongju, Chungbuk, South Korea) with worsening back pain after bumping the left side of her body on a desk 3 days earlier. In the emergency department, she had a blood pressure level of 90/50 mmHg, pulse rate of 120/min, and hemoglobin level of 11.8 g/dL. Computed tomography (CT) on admission revealed a renal laceration with a massive hematoma in the perirenal space (Figure 1(a)). As there was no definite active bleeding on CT and the patient stabilized after fluid resuscitation, diagnostic angiography was performed instead of immediate surgery. Considering the patient’s underlying NF1, angiography was also preferred due to the possibility of vascular fragility and anomalies. A right renal artery angiography showed an abnormally tortuous and irregular main renal artery (Figure 1(b)); however, embolization was not performed because there was no evidence of active bleeding on angiography, and she had improved vital signs after initial fluid resuscitation. On the sixth day after angiography, the patient’s systolic blood pressure level dropped to 60 mmHg, and her hemoglobin level decreased to 6.5 g/dL. A follow-up CT revealed a tortuous and bulging vascular structure of the right renal artery with multiple pseudoaneurysms (Figure 2(a)). Considering the patient’s rapid stabilization following fluid resuscitation, after consultation with the trauma surgery team, repeat angiography was selected over immediate surgical exploration. Upon the second angiography, markedly aggravated hypertrophied changes of the renal artery with multiple pseudoaneurysms were revealed (Figure 2(b)), and complete total embolization of the renal artery was performed using several microcoils and a mixture of n-butyl cyanoacrylate and iodized oil (Figure 2(c)). Subsequent angiography confirmed complete exclusion of the right renal artery, collateral vessels, and incomplete opacification of the right kidney (Figure 2(d)). However, 2 days after embolization, the patient experienced shock again. Despite massive transfusion, the bleeding could not be stopped, and sufficient blood pressure could not be established. The patient finally died without recovering.

Computed tomography (CT) and angiography images on admission. (a) CT scan on admission revealing renal laceration (red arrow) with a large hematoma in the perirenal space and (b) right renal artery angiography showing an abnormally tortuous and irregular main renal artery (red circle).
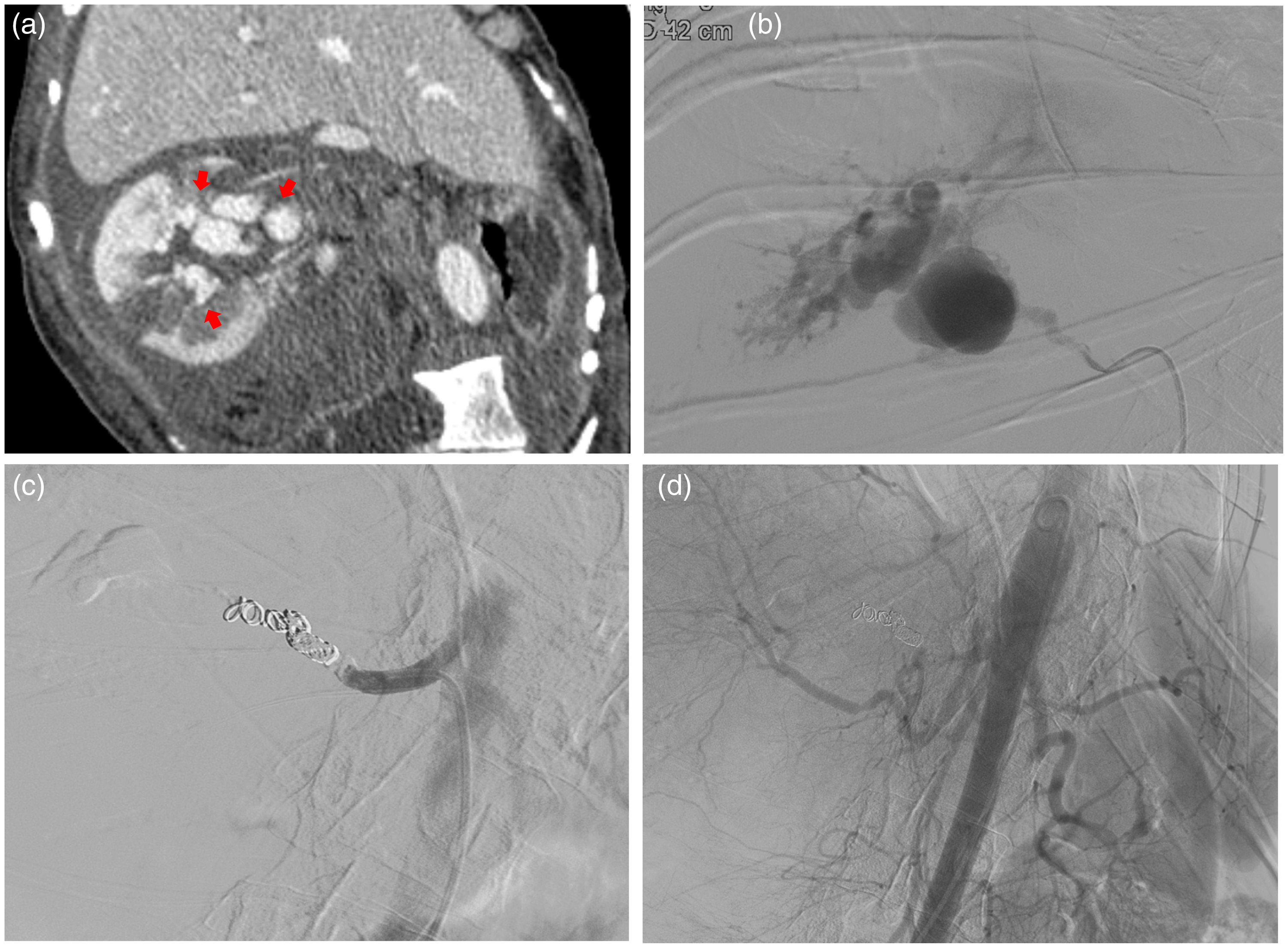
Follow-up computed tomography (CT) and second angiography images 6 days after first angiography. (a) Follow-up CT revealing a tortuous and bulging vascular structure of the right renal artery with multiple pseudoaneurysms (red arrow). (b) Upon the second angiography, multiple pseudoaneurysms arising from the right renal artery were revealed. (c) Complete total embolization of the renal artery was performed using several microcoils and a mixture of n-butyl cyanoacrylate (NBCA) and iodized oil and (d) Subsequent angiography confirming complete exclusion of the right renal artery, collateral vessels, and incomplete opacification of the right kidney.
Institutional review board approval was obtained for this case report. Written informed consent for clinical treatment and publication of relevant case details was obtained from the patient’s legal guardian, as the patient could not provide consent due to her critical condition. All patient information has been fully de-identified to protect privacy. This report has been prepared in accordance with the Case Report (CARE) guidelines as recommended by the EQUATOR Network. 9
Discussion
Aneurysm or pseudoaneurysm formation in NF1 is believed to be a result of friable vasculature in arterial dysplasia. Sayler suggested that intimal thickening accompanying NF1 vasculopathy is the result of Schwann cell proliferation within the arteries. 10 Aneurysms or pseudoaneurysms in patients with NF1 are characterized by fibrous intimal thickening, irregular loss of smooth muscle media, and elastic membrane fragmentation. These features may cause weakening of the supportive connective tissue and adjacent muscle coating in the arterial wall, which could lead to rupture of the arterial wall. 11
Here, we reported a traumatic ruptured pseudoaneurysm of the renal artery in a patient with NF1 who experienced cardiac arrest due to massive bleeding and finally died from uncontrolled hemorrhage, despite complete total occlusion of the renal artery. Until now, a case of traumatic vasculopathy in NF1 with a lethal outcome has not been reported. A patient with bleeding due to a traumatic pseudoaneurysm arising from arteries in the head and neck was successfully treated with surgery or endovascular embolization, according to previous reports.12,13 Unlike other reported cases of vasculopathy in NF1, our patient died of uncontrolled recurrent bleeding. Considering the pathogenesis of vascular abnormalities in NF1 described in the literature, any vessel of the body may be affected by NF1 because of its multisystemic nature, displaying reduced integrity of the vessel wall. 10 Therefore, following trauma, the abnormal vessel architecture can undergo a sequence of changes in which a vessel ruptures and subsequent bleeding increases local pressure on nearby vessels, causing them to rupture. Damage to friable abnormal blood vessels causes additional bleeding through a vicious cycle that is difficult to control, which may have occurred in our case.
Although there is currently no standard management for traumatic vascular injury in patients with NF1, endovascular treatment can be considered the initial treatment approach, as it is a less invasive and effectively accessible technique. 14 Bargiela et al. 15 conducted a systematic review of the endovascular management of NF1-associated aneurysms and showed that endovascular management is safe and effective. However, they also reported that the rates of major and minor complications were 15% and 6%, respectively, with a perioperative mortality rate of 6%. Ruptured aneurysms or pseudoaneurysms of the renal artery in patients with NF1 are rare, with only three case reports published (Table 1).6–8 Among these three cases, angiography revealed a ruptured renal artery aneurysm that was successfully treated with selective coil embolization in two patients.7,8 However, it is difficult to expect complete management with endovascular treatment in all cases; thus, open surgery may occasionally be required. A case report by Abt et al. 6 described a 37-year-old man who experienced retroperitoneal bleeding due to the rupture of a lower pole and main arteries of the right kidney. After undergoing unilateral nephrectomy, the patient recovered. This case also demonstrates the limitations of the endovascular route. In the abovementioned case, angiography showed tortuous and hypertrophied vasculature in the injured area that suddenly and progressively widened; even after complete embolization of the involved renal artery, the patient finally died without recovering. Following trauma, renal artery abnormalities can lead to a cascade of rupture and subsequent bleeding, increasing local pressure on nearby vessels, causing them to rupture. The friability of the renal artery propagates this cycle, causing additional bleeding, which was difficult to control in our case.
Ruptured renal artery aneurysm in patients with neurofibromatosis type 1.

NA: not applicable; CT: computed tomography; M: male; F: female
Therefore, we recommend considering the following approach for hemorrhage from traumatic renal arterial rupture in patients with NF1. First, considering the pathogenesis of NF1, in which the bleeding leads to a cascade of rupturing vessels owing to the high fragility of the vascular wall, causing more vessels to rupture, more intensive care should be continued even after successful hemostasis until the patient fully recovers. Alertness to the possibility of recurrent rebleeding should be emphasized. Second, if the affected renal artery appears hypertrophied or shows progressive changes in morphology, early surgical treatment, such as total nephrectomy, should be actively considered over embolization. This case illustrates the limitations of repeated endovascular management in rapidly progressive vascular injuries and underscores the importance of timely surgical decision-making, even in transiently stabilized patients.
Considering the diverse vascular manifestations of NF1, it is essential to understand the potential arterial complications and their clinical significance. Table 2 summarizes the common arterial manifestations of NF1, including their typical imaging characteristics and implications for management.
Common arterial manifestations in neurofibromatosis type 1.

In conclusion, we report a case of traumatic renal arterial rupture with extensive and progressive bleeding in a patient with NF1, resulting in a lethal outcome. We suggest that a better outcome can be achieved through active management strategies based on a combined approach with endovascular and surgical treatment and more careful monitoring of rebleeding, with awareness of the possibility of a serious clinical course in vascular injury associated with NF1.
Footnotes
Acknowledgements
None.
Author contributions
Conceptualization: Jisun Lee, Yook Kim
Data curation: Jisun Lee
Formal analysis: Jisun Lee, Yook Kim
Investigation: Jisun Lee, Yook Kim
Writing—original draft: Jisun Lee
Writing—review & editing: Jisun Lee, Yook Kim.
Availability of data and materials
All data and materials are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The Institutional Review Board of Chungbuk National University Hospital approved the retrospective review of the patient’s medical records (IRB No. 2023-12-007). Written informed consent for clinical treatment and publication of relevant case details was obtained from the patient’s legal guardian, as the patient could not provide consent due to her critical condition.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.