
Abstract
Neurofibromatosis type 1 (NF1) is an autosomal dominant disease characterized by neuorocutaneous lesions and multisystem involvement. Other notable features of NF1 include vasculopathy in the form of stenosis, occlusion, aneurysm, pseudoaneurysm, arteriovenous deformity, and rupture, which are difficult to manage and can have fatal outcomes. We describe two cases of extensive and progressive brachial artery hemorrhage following blunt trauma in patients with NF1. Management of these patients included combined endovascular and surgical treatment based on the patients’ condition. The patients had a poor prognosis because of uncontrolled bleeding. While one patient died, the other survived, but the involved arm was amputated. Endovascular treatment is a widely used, popular, minimally invasive, and safe method to control the bleeding associated with NF1. However, this treatment can be challenging at times. Close collaboration between an interventional radiologist and surgeon is necessary for optimal treatment and careful follow-up for this condition.
Background
Neurofibromatosis (NF) is an autosomal dominant disorder affecting approximately 1 in 3000 individuals. NF type 1 (NF1) is the most common subtype with characteristic café au lait macules, benign neurofibromas, and iris hamartomas. 1 Although NF1 is rare, patients with this condition might also develop cardiovascular disease, including vascular stenosis, occlusion, aneurysm, pseudoaneurysm, and fistula formation. 2 Most patients with NF1-related vascular lesions are asymptomatic. However, vascular disease often presents as rupture of an undiagnosed lesion, which has a high mortality among young patients with NF1 and is the second most common cause of mortality in NF1 after malignancy. 3 The most common lesions of NF1 vasculopathy involve the renal, aortic, and mesenteric arteries. 4 To the best of our knowledge, five case reports involving a ruptured brachial artery aneurysm in patients with NF1 have been published.5–9 Of these patients, two died, one survived, but the associated arm was amputated, and only two patients had successful treatment outcomes.5,6 Bleeding from the brachial artery in patients with NF1 is rare, but some patients have a particularly poor prognosis compared with other patients.4,7,8 Therefore, further studies on NF1 are necessary We report our experience of two cases of NF1 with extensive and progressive brachial artery hemorrhage following blunt trauma, which had a lethal outcome. We also discuss the optimal treatment strategies of NF1.
Case presentation
We obtained informed consent from the patients to treat their disorder. The reporting of this study conforms to the CARE guidelines. 10
Case 1
A 33-year-old man with NF1 presented to our hospital with rapidly increasing massive swelling and pain in his left shoulder after a fall from the stairs 30 minutes previously. On arrival, his blood pressure was 120/73 mmHg and the hemoglobin level was 123 g/L. However, his hemoglobin level fell to 75 g/L in 2 hours, which required packed red blood cell transfusion of 4 units. Computed tomography (CT) showed a huge hematoma with active bleeding in the left shoulder (Figure 1a). Left subclavian artery angiography showed active bleeding and alteration of vessels arising from a branch of the brachial artery (Figure 1b). The feeding branches were selectively catheterized and embolization was performed using gelfoam. Subsequent angiography showed successful exclusion of the active bleeding. On the sixth day after embolization, the patient’s condition deteriorated, with a rapid increase in swelling along with severe pain in the left shoulder again. A follow-up CT scan showed an increase in the size of the hematoma in the left shoulder. During the second endovascular approach, left subclavian angiography showed that the brachial artery and its branches were tortuous and hypertrophied with multiple pseudoaneurysms, which drained into the subclavian vein and created an arteriovenous fistula (AVF) (Figure 1c). Embolization of these vessels was performed using a mixture of n-butyl cyanoacrylate and iodized oil. and subsequent angiography confirmed successful exclusion of the pseudoaneurysms and the AVF (Figure 1d). However, on the following day after the second embolization, severe pain and swelling of the left shoulder recurred, and the patient had to undergo amputation of the left shoulder. After the surgery, hemodynamic stability was achieved and the patient was discharged 3 weeks after surgery.

A 33-year-old man with neurofibromatosis type 1 presented to our hospital with rapidly growing massive swelling and pain in the left shoulder after a fall. (a) Computed tomography shows a huge hematoma with active bleeding (red arrow) in the left shoulder. (b) Left subclavian artery angiography shows active bleeding (red arrow) arising from a branch of the axillary artery. (c) On the sixth day after the first embolization, left subclavian angiography shows that the axillary artery and its branches are tortuous and hypertrophied with multiple pseudoaneurysms (red arrow). The axillary artery and its branches drain into the subclavian vein (open red arrow), suggesting an arteriovenous fistula (AVF). (d) Embolization of these vessels was performed and subsequent angiography confirmed successful exclusion of the pseudoaneurysms and an AVF.
Case 2
A 32-year-old man with NF1 presented to our hospital with severe swelling and pain in his right upper arm caused by bumping into a chair 1 hour before admission. He had a blood pressure of 80/40 mmHg and a heart rate of 104 beats/minute on arrival to the hospital. A CT scan showed a huge hematoma with active bleeding in the right upper arm, and a pseudoaneurysm arising from the right bronchial artery was identified on a volume rendering image (Figure 2a). The surgical team on-call decided to proceed with surgical resection and ligation of the involved vessel as the first-line treatment. Unfortunately, the patient’s condition deteriorated that night with increasing swelling and pain in the right upper arm, and emergent angiography was recommended. Selective subclavian artery angiography showed extravasation of the contrast medium at multiple locations and a pseudoaneurysm arose from the branches of the brachial artery. Additionally, all of the feeding vessels were tortuous and hypertrophied (Figure 2b). Embolization was performed via a microcatheter, using a mixture of n-butyl cyanoacrylate and iodized oil, microcoils, and gelfoam. Post-embolization angiography showed successful occlusion of the active bleeding. However, the size of the hematoma in the right upper arm gradually increased 4 days after embolization, and the patient became hemodynamically unstable. Therefore, upper extremity amputation was performed. Angiography was repeated because of swelling of the right shoulder 1 day after surgery, and subclavian angiography showed new and multiple active bleeding sites arising from the branch of the axillary artery (Figure 2c). Complete total embolization of the axillary artery was performed using a mixture of n-butyl cyanoacrylate and iodized oil. Subsequent angiography showed successful complete obliteration of the axillary artery (Figure 2d). Despite aggressive treatment, on the seventh day after repeated embolization, the patient developed shock and died of uncontrolled bleeding.

A 32-year-old man with neurofibromatosis type 1 presented to our hospital with severe swelling and pain in his right upper arm after bumping into a chair. (a) A computed tomography scan shows a pseudoaneurysm (red arrow) arising from the right brachial artery, which was identified on a volume rendering image. (b) Selective subclavian artery angiography shows multiple extravasations of the contrast media (red arrowheads) and pseudoaneurysms (red arrows) arising from the branches of the subclavian artery. All feeding vessels are tortuous and hypertrophied. (c) Repeated subclavian angiography 1 day after the upper extremity amputation shows new areas of active bleeding (red circle) arising from the branch of the axillary artery. (d) Complete total embolization of axillary artery was performed. Subsequent angiography shows successful complete occlusion of the axillary artery.
Discussion and conclusions
NF1 is caused by mutation of the neurofibromin-encoding gene, which is located on the long arm of chromosome 17q11.2. 1 Impairment of this gene results in an increased propensity for uncontrolled spindle cell growth in the vessel walls and subsequent dysplasia of the smooth muscle in the intimal and medial layers. Therefore, these changes in normal vascular maintenance and repair controlled by neurofibromin leads to vasculopathy and probably arterial fragility. This makes repairing bleeding vessels in patients with NF1 challenging. 11
We experienced two cases of NF1 with extensive and progressive bleeding caused by traumatic vascular injury, and this led to a lethal outcome in one patient. Despite the combined management with endovascular and surgical treatment based on the patients’ conditions, they had a poor prognosis owing to uncontrolled massive bleeding. In both cases, angiography showed tortuous and hypertrophied vasculature in the injured area, which suddenly progressed and gradually widened within 4 to 6 days after the first embolization.
To date, there have been no reports or studies about traumatic vasculopathy of the brachial artery with a lethal outcome in patients with NF1. However, because of the pathogenesis of vascular abnormalities in NF1, any vessel in the body might be affected by NF1 because of its multisystem involvement. This situation reduces the integrity of the vessel wall due to a deficiency of neurofibromin. 12 Therefore, following this trauma, the injured vessel architecture might undergo a sequence where the injured vessel ruptures and subsequent bleeding increases local pressure on nearby vessels, causing rapid progression of vascular damage and repeated bleeding. The friability of these vessels propagates this cycle, causing additional bleeding that is difficult to control, as found in the current cases.
Aneurysms of the brachial artery in patients with NF1 are rare. Only five cases involving a ruptured brachial artery aneurysm have been published in the English literature between 1998 and 20195–9 (Table 1). Of these five cases, two patients died after resection and ligation of the artery.7,8 In another case, saphenous vein reconstruction failed owing to postoperative bleeding, and this resulted in amputation of the upper arm. 9 There were two cases of successful management of a ruptured brachial artery aneurysm by reconstructing the ruptured brachial artery using the great saphenous vein.5,6
Reported cases of a ruptured brachial artery aneurysm in patients with neurofibromatosis type 1.
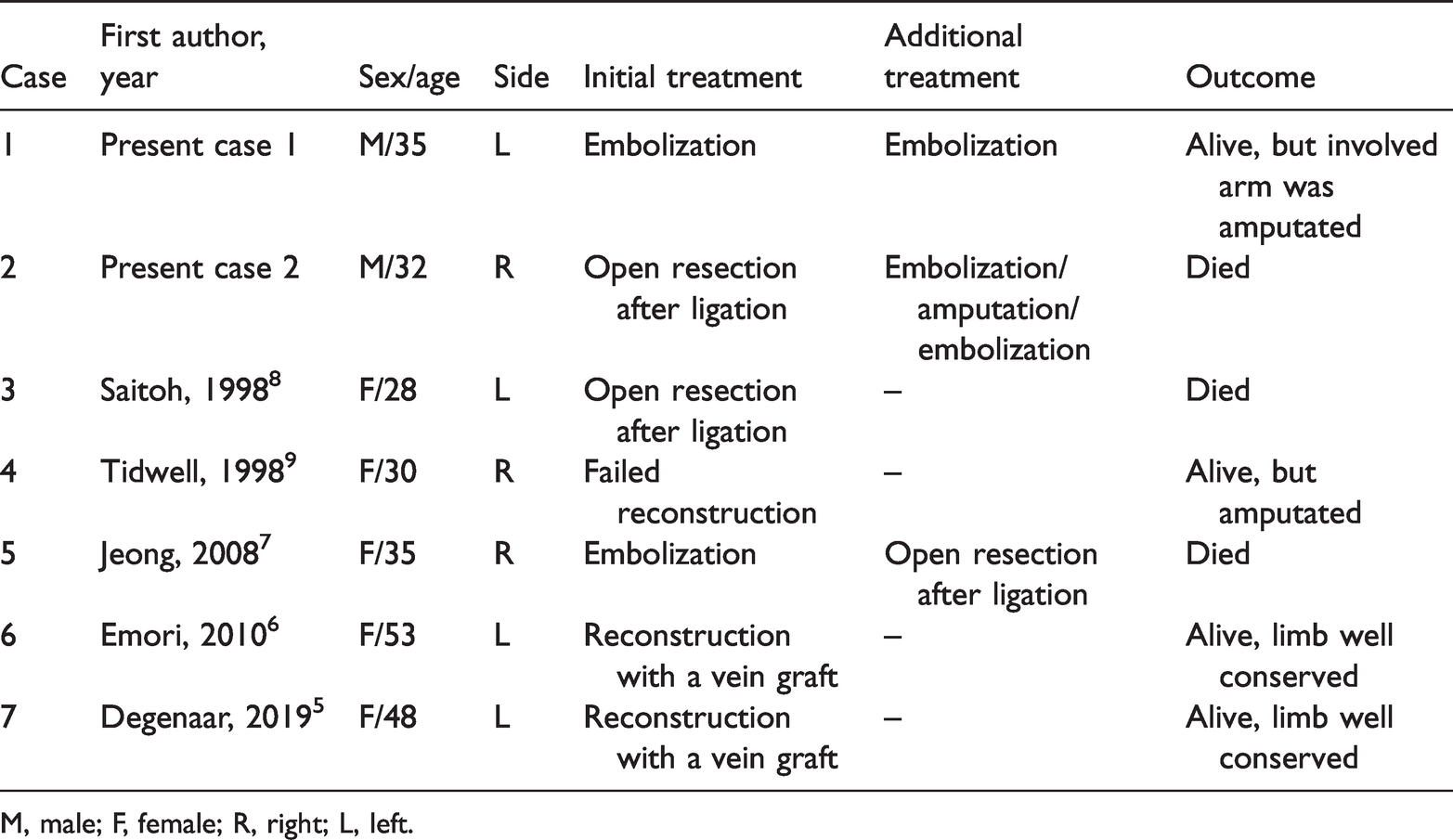
M, male; F, female; R, right; L, left.
Although there is currently no standard management for traumatic vascular injury in patients with NF1, endovascular treatment can be the first-line option because it is a minimally invasive and easily accessible technique. Moreover, the considerable fragility of the vascular wall leads to difficulty in achieving hemostasis.13,14 David et al. 4 reported a systematic review of endovascular management of NF-associated aneurysms, and concluded that endovascular management is safe and effective. However, they also reported that the rates of major and minor complications were 15% and 6%, respectively, and the rate of perioperative mortality was 6%. Successful management with endovascular treatment might not be effective in all cases of NF1. Therefore, open surgery might be required and better outcomes are achievable with a combined approach.15,16 If the brachial artery is involved in patients with NF1 following trauma, priority should be given to surgical treatment, such as reconstruction with a vein graft, rather than embolization.
Although endovascular treatment appears to be a safe and minimally invasive approach for controlling bleeding associated with NF1, our cases showed a limitation of endovascular treatment for a ruptured brachial artery associated with NF1. The choice of embolic agents is based on the vascular anatomy, angiographic findings, the catheter position, and the preferred operator. liquid embolic agents, such as glue or gelfoam, are preferred over a stent graft because of the fragile arterial walls associated with NF1 vasculopathy, causing additional arterial injury. In case 1, we successfully controlled bleeding from the brachial artery using only embolization using gelfoam and glue. However, after the first embolization, repeated angiography showed marked aggravation of hypertrophied vessels with an AVF and subsequent failure of repeated embolization, resulting in amputation of the arm. In case 2, although open surgery with resection and ligation of the involved vessel were performed, extended rupture of the vessels and continuous bleeding were observed on angiography. Despite amputation and total embolization of the right subclavian artery with a permanent embolic agent (i.e., glue), the patient died of uncontrolled bleeding. 4
To date, the results of endovascular management in patients with NF1 and brachial artery hemorrhage are not satisfactory. There is an insufficient number of NF1 cases to develop a consensus on the direction of treatment through surgery with reconstruction. However, if the patient is stable at the time of admission, active treatment and careful follow-up can improve the patient’s prognosis. There are no definite guidelines on the management of traumatic brachial arterial injury in patients with NF1. On the basis of our review, we recommend guidelines for NF1 as shown in Figure 3.

Proposed algorithm for treatment of traumatic injury to the brachial artery in patients with NF1
In conclusion, we report two patients with NF1 and traumatic brachial injury causing extensive and progressive bleeding with one lethal outcome. Although endovascular treatment is a widely used, popular, minimally invasive, and safe method for controlling bleeding associated with NF1, it can be challenging at times. Close collaboration between an interventional radiologist and surgeon is necessary to decide the appropriate line of treatment and careful follow-up.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211025344 - Supplemental material for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605211025344 for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature by Jisun Lee and Yook Kim in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211025344 - Supplemental material for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature
Supplemental material, sj-pdf-2-imr-10.1177_03000605211025344 for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature by Jisun Lee and Yook Kim in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605211025344 - Supplemental material for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature
Supplemental material, sj-pdf-3-imr-10.1177_03000605211025344 for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature by Jisun Lee and Yook Kim in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605211025344 - Supplemental material for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature
Supplemental material, sj-pdf-4-imr-10.1177_03000605211025344 for Life-threatening brachial artery hemorrhage and a lethal outcome in patients with neurofibromatosis type 1: two case reports and a review of the literature by Jisun Lee and Yook Kim in Journal of International Medical Research
Footnotes
Ethics statement
This study was approved by the institutional review board of Chungbuk National University Hospital (2019-01-014-003). Written informed consent was obtained from the patients for publication of this study and any accompanying images.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
JL and YK: study design, implementation of the study, data collection/validation, editing and revision of the manuscript, interpretation of results, and major contributions to writing the manuscript. All authors have read and approved the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.