
Abstract
Optic disc capillary hemangiomas, a rare capillary hamartoma that often invades optic nerve fibers and disc plaque bundles, have been a therapeutic challenge for ophthalmologists in recent years due to their unique location. A woman in her early 50s presented with blurred vision in the right eye for 2 days. On ocular examination, her best-corrected visual acuity was 20/340 in the right eye. Wide-field fundus imaging revealed a red mass on the temporal side of the optic disc. Optical coherence tomography revealed macular edema. The diagnosis was optic disc capillary hemangioma. Subsequently, 0.5 mg ranibizumab was intravitreally injected into the right eye once monthly, for a total of two injections. The patient was re-examined at 15 days, 50 days, and 21 months after the first operation. The patient’s postoperative best-corrected visual acuity improved to 20/60, and macular edema and exudation were reduced in the short term compared with those in the previous period; however, the tumor did not change significantly. The anti-vascular endothelial growth factor agent ranibizumab is effective in treating optic disc capillary hemangiomas.
Keywords
Background
Optic disc capillary hemangioma is composed of capillary clusters of connective tissue and dilated blood vessels with uneven tubular diameters. It is a congenital developmental hemangioma and a component of retinal hemangiomatosis (von Hippel–Lindou (VHL) syndrome); however, it is far less common than retinal capillary hemangioma in terms of clinical morbidity. 1
These tumors tend to be orange–yellow or red in color and have a round or oval-like mass. Small tumors may partially obscure optic disc structures, whereas large tumors may completely obscure them. Regardless of its size, the center of the tumor is mostly located outside the margin of the optic disc. When patients exhibit symptoms of vision loss, they often experience varying degrees of peritumoral retinal exudation and edema, with a poor treatment effect.
Owing to the unique location of optic disc capillary hemangiomas, they often invade optic nerve fibers and disc plaque bundles, which makes them difficult to treat. There are currently no treatment guidelines, and the treatments reported in the literature include traditional laser photocoagulation, photodynamic therapy (PDT), transpupillary thermotherapy (TTT), vitreoretinal surgical treatments, and anti-vascular endothelial growth factor (anti-VEGF) treatments.
Case presentation
In August 2022, a woman in her early 50s presented to the Department of Ophthalmology, the Provincial Hospital of Shandong First Medical University (Shandong Provincial Hospital), Jinan, Shandong Province, China, with a history of blurred vision in her right eye for 2 days. She had a history of lung cancer for >1 year (pT1bN0M0) and underwent lung cancer ablation 2 months prior without metastasis. There was no relevant family history and no history of trauma. Specialized examination revealed that the best-corrected visual acuity was 20/340 in the right eye and 20/20 in the left eye, and there was no improvement with best correction. Intraocular pressure in both eyes was within the normal range. Anterior segment examination was normal with a mild nuclear sclerotic cataract.
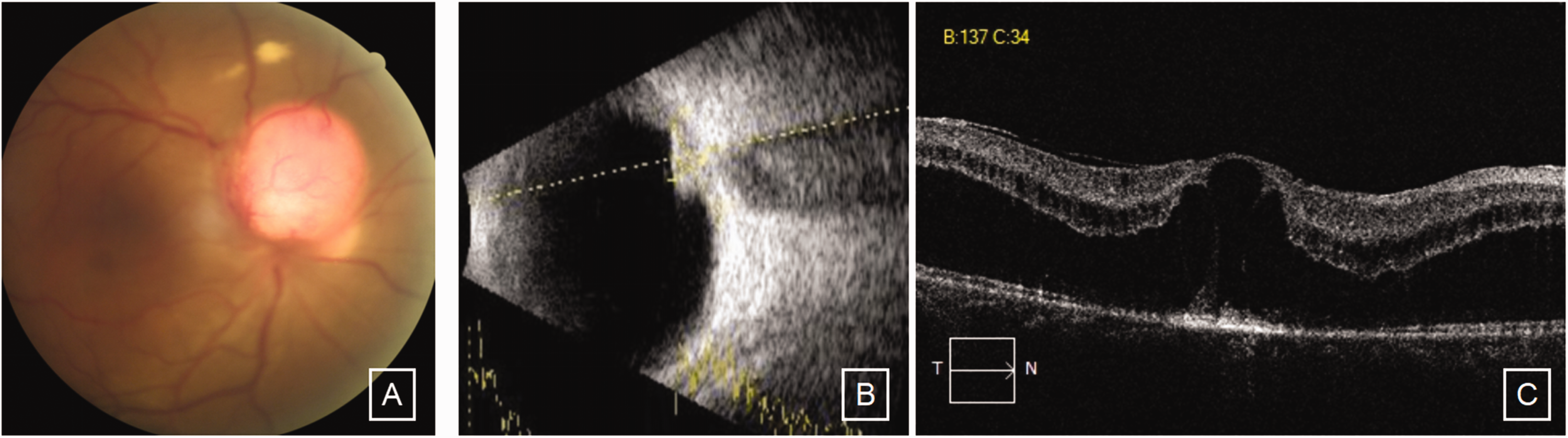
Specialized examinations, including wide-field fundus imaging, ocular ultrasound, optical coherence tomography (OCT) of the macula and optic disc, and fundus fluorescein angiography, revealed optic disc capillary hemangioma and macular edema in the right eye (Figure 1(a–h)). Orbital magnetic resonance imaging revealed that the retina of the right eye was thickened. The optic chiasm alignment was normal, and no significant thickening or atrophy was observed. The visual crossover was clear, and there was no obvious destruction of the orbital bone or signs of space occupation. Whole-body positron emission tomography–computed tomography revealed no abnormalities, with no postoperative changes in the lungs. Combining the patient’s symptoms, signs, and fundus imaging, the diagnosis of optic disc capillary hemangioma (endogenous type) of the right eye and postoperative lung cancer was considered.

Ancillary eye examinations at the first visit. (a) The optic disc border was unclear, and a well-defined roundish red mass with a diameter of approximately 2.0 PD was observed on the temporal side of the optic disc. The center of the tumor was located outside the edge of the optic disc, blood vessels were visible, and the surrounding retina was edematous, with hard exudates. The macular light reflex was absent, Continued.and three nerve fiber layer hemorrhages were observed in the retina of the inferotemporal periphery. (b) The left optic disc and macula were normal. (c) Ocular ultrasound revealed that a roundish, strongly echogenic light mass with a size of approximately 3.80 mm × 3.87 mm could be detected on the wall of the globe above the optic disc in the right eye, with a membranous band attached to the surface of the light mass. (d) Optical coherence tomography (OCT) of the macula showed macular edema and thickening. The central subfield thickness was 770 μm, subretinal fluid was combined with neuroepithelial detachment, and the reflex of the pigment epithelial layer was disrupted. (e) OCT of the optic disc revealed a wide, highly elevated light band on the surface of the tumor at the optic disc. (f) In the arterial and early venous stages, the tumor filled rapidly and the fluorescence was uneven, showing a mottled change; in contrast, the basic outline of the tumor was clearer. (g) In the venous stage, the size and shape of the tumor basically remained unchanged but continued to increase and (h) in the late stage of contrast, the tumor showed fluorescein staining at the margins and around the tumor and fluorescein regression within the tumor.
After establishing the diagnosis, 0.5 mg ranibizumab was administered via intravitreal injection into the right eye with the aim of reducing the macular edema, improving best-corrected visual acuity, and decreasing the risk of vision loss. At the postoperative half-monthly review, the patient reported a gradual recovery of vision and a decrease in the number of floaters in front of the eyes compared with that in the previous period. The best-corrected visual acuity of the right eye was 20/60. Upon fundus examination, there was no significant change in the size or shape of the tumor compared with that at the first visit (Figure 2(a)). OCT of the optic disc showed no significant changes (Figure 2(b)). OCT of the macula revealed that the edema of the macular area of the right eye was significantly reduced compared with that at the first visit (Figure 2(c)).

Examinations at the half-month review after the first vitreous injection of ranibizumab. (a) There was no significant change in the size or shape of the tumor compared with that at the first visit, retinal edema had occurred around the tumor, and a light reflex in the macular area was observed. (b) Optical coherence tomography (OCT) of the optic disc showed no significant changes and (c) OCT of the macula revealed that the edema of the macular area of the right eye was significantly reduced compared with that at the first visit.
Twenty days after the operation, 0.5 mg ranibizumab was reinjected into the vitreous cavity of the right eye. One month after the second injection, the best-corrected visual acuity of the right eye was 20/60, and fundus examination and ultrasound of the eye showed no obvious change in the size or shape of the tumor (Figure 3(a–b)). Optic disc OCT and macular OCT revealed that the macular edema persisted, although it reduced compared with that at the first visit, and aggravated from the initial review (Figure 3(c–d)).

Examinations at the 1-month review after the second injection of ranibizumab. (a) Fundus examination showed no obvious change in the size or shape of the tumor. (b) Ultrasound of the eye revealed that the surface of the optic disc was elevated, with a height × width of 1.77 mm × 2.77 mm (c) optic disc optical coherence tomography (OCT) revealed that there was still a highly elevated light band on the surface of the tumor at the optic disc of the right eye and (d) Macular OCT revealed that macular edema persisted, reduced compared with that at the first visit, and aggravated compared with that at the initial review; the extent of neuroepithelial detachment underneath increased compared with that at the last review.
Twenty-one months after surgery, the best-corrected visual acuity of the right eye was 20/60, and fundus examination and ocular ultrasound revealed that the tumor body was obviously enlarged, with a diameter of approximately 2.5 papilla diameter (PD) (Figure 4(a–b)). Macular OCT revealed significant edema and thickening of the macula (Figure 4(c)). As there was no obvious change in best-corrected visual acuity and the disease progressed slowly, no special treatment was administered, and the patient was followed up for observation.
Examinations at the 21-month review after the second injection of ranibizumab. (a) The tumor body was obviously enlarged, with a diameter of approximately 2.5 PD. (b) Ocular ultrasound revealed a confined elevated mass in the spherical wall above the optic disc deviation. The height of the mass was approximately 3.41 mm, the base was approximately 8.07 mm × 7.22 mm and (c) macular optical coherence tomography revealed significant edema and thickening of the macula.
All patient details have been de-identified. After fully informing the patient and her family about treatment and prognosis, we obtained her consent for treatment. This study was approved for publication by the review board of the Provincial Hospital of Shandong First Medical University (Shandong Provincial Hospital). The reporting of this study conforms to Case Report (CARE) guidelines. 2
Discussion and conclusions
Retinal capillary hemangioma is a benign vascular tumor that occurs in the retina. Optic disc capillary hemangioma occurs in the vicinity of the optic disc and is often reported as an isolated case because of its unique location and lack of obvious nourishing or refluxing vessels. Depending on the clinical manifestations and depth of the lesion, optic disc capillary hemangiomas can be classified as endophytic (limited) or exophytic (diffuse), with the endogenous type being more common in the clinic. 3
The diagnosis of optic disc capillary hemangioma is mainly based on the patient’s clinical manifestations and fundus examination. Optic disc capillary hemangiomas should also be differentiated from other diseases of the optic disc. Melanocytoma of the optic disc is a gray or black mass with clear, elevated margins, and glioblastoma of the optic disc tends to be a white mass; however, both of them rarely cause exudation and edema of the surrounding retina. Optic discitis presents with edema of the optic disc as well as exudation from the surrounding retina but does not allow for the detection of definitive mass-like structures on fundus examination. In particular, on fundus fluorescence angiography, a tumor-like lesion cannot be detected, and there is no characteristic “emptying” phenomenon of hemangiomas. 4 Vitreous warts of the optic disc are often observed in both eyes and can be identified via autofluorescence-assisted fundus fluorescence angiography, with no significant change in shape or size after the injection of contrast medium and no fluorescein leakage.
VHL syndrome is an autosomal dominant multisystemic neoplastic disease with a propensity for carcinoma and may manifest as craniospinal hemangioblastoma, renal cell carcinoma, pheochromocytoma, pancreatic tumor, retinal hemangioma, or their combinations.5–6 Retinal capillary hemangioma is one of the earliest and most common manifestations of VHL disease. 7 Therefore, for patients with optic disc capillary hemangioma, a detailed family history should be taken, examination of various systems of the body should be completed, and VHL gene screening should be performed if conditions permit. 8
It remains unclear whether the development of our patient’s eye disease was related to her lung cancer or lung surgery. Our patient had multiple nodules in both lungs. After right lung middle lobe resection, the pathology showed invasive adenocarcinoma (pT1bN0M0). Ten days after right lung surgery, the patient developed ocular symptoms. In this regard, we concluded that there was no significant correlation between the disease and lung cancer or lung surgery. Optic disc capillary hemangioma is a congenital developmental hemangioma. 9 VHL disease can affect various organs, including the brain, spinal cord, retina, kidneys, pancreas, and adrenal glands. However, no VHL disease associated with lung cancer has been described so far. To determine whether the patient’s optic disc capillary hemangioma was associated with lung cancer, further confirmation is needed.
In recent years, optic disc capillary hemangiomas have been a therapeutic challenge for ophthalmologists. These tumors have a wide range of clinical regression; however, the majority of patients tend to exhibit progressive tumors and severely impaired vision. 9 Optic disc capillary hemangiomas are often combined with a number of other complications, including macular edema and exudation, subretinal hemorrhage, anterior retinal membrane formation, or exudative or tractional retinal detachment. 10 Therefore, timely diagnosis and treatment of optic disc capillary hemangiomas are particularly important. However, most optic disc hemangiomas are located on the temporal side of the optic disc. Owing to their peculiar location, destroying the tumor while preserving the nerve fiber layer on its surface is almost impossible, making treatment difficult. 11 Various treatments have been reported in the literature, and it is important to select different treatment options according to the patient’s condition during clinical management. These methods include observation, conventional laser photocoagulation, PDT, brachytherapy, transpupillary warming, vitreoretinal surgery, and anti-VEGF therapy.12–13 Recently, belzutifan, a novel hypoxia-inducible factor-2α inhibitor approved by the US Food and Drug Administration, has been reported to be effective in the systemic treatment of VHL-associated tumors as well as the treatment of optic disc hemangiomas associated with VHL syndrome.14–15 Regardless of the treatment method, the focus of treatment is to stabilize and control the tumor while minimizing complications such as retinal exudation and hemorrhage secondary to the tumor to reduce the impact on visual function.
It has been reported in the literature that angiogenic factors are important for maintaining and promoting the growth of retinal capillary hemangiomas,16–17 and optic disc hemangiomas may be VEGF-dependent 18 ; therefore, anti-VEGF therapy for optic disc hemangiomas is effective.19–20 The role of anti-VEGF drugs in retinal hemangiomas has been reviewed, and intravitreal injections of anti-VEGF drugs have been reported to reduce macular edema and subretinal effusion. 21 Macular edema responds to VEGF therapy mainly in the following ways: (a) inhibition of neovascularization; (b) improvement of the permeability of retinal and choroidal microvessels; and (c) reduction of effusion and edema caused by vascular leakage.22–23 In the current case, OCT revealed that the right eye had thickened macular edema, combined with subretinal fluid. We first administered anti-VEGF therapy. Half a month after the vitreous injection of 0.5 mg ranibizumab, the best-corrected visual acuity of the right eye was 20/60. Although the size and shape of the tumor on fundus examination did not change significantly compared with those at the first visit, the patient reported that her best-corrected visual acuity had improved significantly. Edema of the macular area on OCT was reduced compared with that at the first visit. The patient’s best-corrected visual acuity improved, but the tumor size did not change significantly. Although the tumor was not eradicated at that time, anti-VEGF therapy for macular edema was continued to maintain or improve the patient’s best-corrected visual acuity. Upon review 21 months later, the patient’s tumor was significantly enlarged, and the edema and exudation in the macular area were worse than those at the first visit. TTT, PDT combined with anti-VEGF therapy, and other treatments were considered, but the patient’s best-corrected visual acuity did not obviously change. Moreover, the disease progressed slowly; therefore, no special treatment was administered, and the patient was followed up for observation. If the patient’s tumor continued to increase in size and vision loss was observed during follow-up, treatments such as TTT and PDT combined with anti-VEGF therapy could be considered. In patients with severe complications, such as vitreous fiber hyperplasia and retinal detachment, combined vitreoretinal surgery is required for further treatment. Although the effect of long-term treatment is poor, in the short term, anti-VEGF therapy can be helpful in reducing macular edema, improving best-corrected visual acuity, and enhancing the patient’s quality of life.
The anti-VEGF agent ranibizumab was found to be effective in the treatment of optic disc capillary hemangioma. Although it does not reduce the size of the tumor, it decreases macular edema, delaying progression of the disease in the short term, improving the patient’s best-corrected visual acuity, and enhancing the patient’s quality of life, as was evident in this case. Because of the long-term therapeutic effect, the tumor size tends to gradually increase, and the disease complicating macular edema is prone to recurrence, which needs to be treated with multiple vitreous cavity injections of ranibizumab. If the tumor size continues to increase, which considerably affects the patient’s best-corrected visual acuity, ranibizumab should be combined with vitreoretinal surgery for further treatment.
Footnotes
Acknowledgements
The authors thank the patient and her family for their cooperation at each follow-up. Furthermore, we thank them for their consent to share their clinical information for publication.
Author contributions
All authors contributed to the study conception and design. Acquisition of the patient data: SZZ and YLW. Original drafting of the manuscript: MH, FJL, and SNM. Manuscript revision: MH and WYZ. All authors have approved the final manuscript.
Consent to participate
Written informed consent was obtained from the patient for examination and treatment as well as for the publication of any potentially identifiable images or data included in this article.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article (and/or its supplementary materials).
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Ethics considerations
This study was approved by the Ethics Committee of the Provincial Hospital of Shandong First Medical University (Shandong Provincial Hospital).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.