
Abstract
We report a case of a man in his early 50 s who was admitted to our hospital for anorexia. An imaging examination led to a preoperative diagnosis of a gastrointestinal stromal tumor and gallbladder stones. He underwent treatment by laparoscopic cholecystectomy and distal partial gastrectomy with lymph node dissection. The final histopathological diagnosis was gastric schwannoma and tubular adenoma of the gallbladder. Gastric schwannoma accounts for only 0.2% of all gastric tumors, and tubular adenoma constitutes only 2.2% of gallbladder tumors. This report describes the diagnosis and treatment process for this combination of tumors, thus providing a reference for similar cases.
Keywords
Introduction
Reports of multiple tumors, especially primary malignancies in the digestive system, have recently increased partly because of improved diagnostic techniques and the increasingly aging population. 1 However, reports of multiple synchronous benign tumors are relatively rare. To the best of our knowledge, we report the first case of gastric schwannoma (GS) coexisting with tubular adenoma of the gallbladder (GB). We describe this unique combination of tumors with complete clinical data.
Case presentation
A man in his early 50 s with a 1-week history of anorexia visited our hospital for treatment. A physical examination and laboratory investigations showed no major findings. However, abdominal ultrasound showed a large hypoechoic mass (8.3 × 7.5 cm) located between the right hepatic lobe and the stomach. The mass exhibited an irregular shape, well-defined border, heterogeneous internal echoes, and a few blood flow signals in and around the mass (Figure 1a). When we focused on the GB in the fasting state, a hyperechoic polypoid protrusion (1.4 ×0.9 cm) was located in the GB neck and was attached to the wall with a thin stalk and without a shadow. There was no blood flow in or around the mass (Figure 1b).

(a) Ultrasound image showing a hypoechoic mass located between the right hepatic lobe and the stomach and (b) Ultrasound image showing a hyperechoic polypoid protrusion located at the gallbladder neck.
A contrast-enhanced coronal computed tomography scan showed a lobulated low-density mass (8.7 × 8.2 cm) on the lesser curvature of the gastric body. The growth pattern of this mass was mainly outside the gastric cavity, leading to mild compression of the right hepatic lobe. The gastric mucosa was enhanced to a greater degree than the mass (Figure 2a). A plain computed tomography scan of the GB showed no abnormalities other than gallstones (Figure 2b). Additionally, several enlarged perigastric lymph nodes were found. These imaging findings suggested that the mass was likely a gastrointestinal stromal tumor.
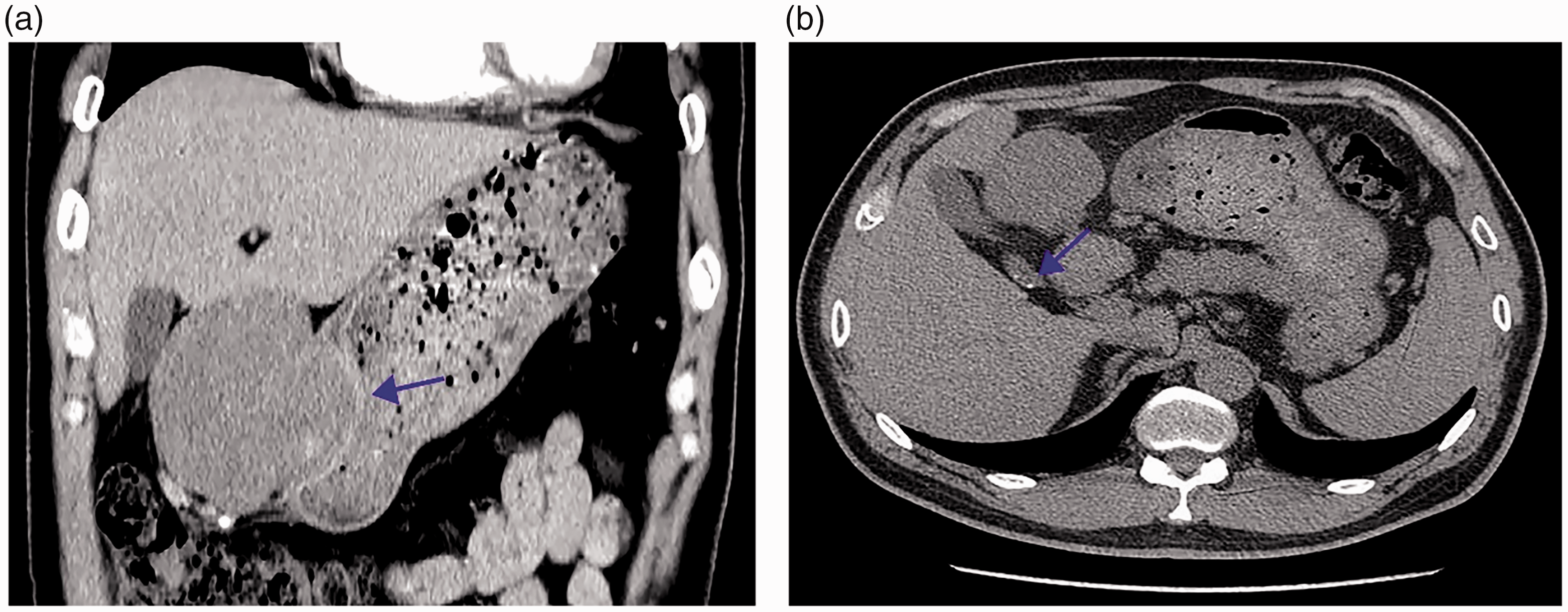
(a) Contrast-enhanced computed tomography scan shows a lobulated low-density mass located at the lesser curvature of the gastric body. The gastric mucosa (arrow) is enhanced to a greater degree than the mass and (b) Plain computed tomography scan showing several gallstones (arrow) in the neck of the gallbladder.
The patient underwent laparoscopic cholecystectomy and distal partial gastrectomy with lymph node dissection. A pathological analysis showed that features of gastric and gallbladder specimens were consistent with the GS and the tubular adenoma, respectively (Figure 3). Sixteen perigastric lymph nodes were characterized by reactive lymphoid hyperplasia. Fortunately, all surgical margins were negative. The patient was well with no special treatment 15 months after surgery.

(a) The stomach tumor is pathologically composed of bland spindle cells (hematoxylin and eosin, ×40). (b, c.) Positive immunohistochemical staining of S-100 and SOX-100 and (d) The polypoid lesion of the gallbladder has features consistent with a tubular adenoma (hematoxylin and eosin, ×40).
Discussion
A schwannoma is a type of nonepithelial tumor originating from Schwann cells in any nerve sheath. If the digestive tract is affected, schwannomas are most likely to occur in the stomach.2,3 Patients with GS are often asymptomatic, and their tumor is discovered incidentally. These characteristics, coupled with a lack of specificity on imaging, make the preoperative diagnosis of GS challenging, especially when differentiating a GS from a gastrointestinal stromal tumor. 4 A definitive diagnosis depends on a histopathological examination and immunohistochemical studies.3,4 Adenoma of the GB is a type of epithelial tumor and is usually benign. Adenoma is also a type of neoplastic polyp of the GB and is usually classified into tubular, papillary, and mixed types. 5 Epidemiological data have shown that tubular adenomas are less common with a lower risk of malignant transformation than papillary adenomas, and papillary adenomas are considered a premalignant condition of the GB.
It should be noted that Nishihara et al. 6 reported that their three cases of tubular adenoma of the GB were accompanied by squamoid spindle cell metaplasia, and the patients’ average age was 40 years. Turrini et al. 7 described a 29-year-old man with a tubular adenoma with focal adenocarcinoma. Therefore, clinicians should be aware of the likelihood of malignant transformation of tubular adenomas. The adenoma–carcinoma sequence and dysplastic carcinoma sequence are the primary pathogenesis for most carcinomas in the digestive tract.8,9
Importantly, Chen et al. 10 described a 72-year-old man with synchronous gastric adenocarcinoma, GB adenocarcinoma, and a stromal tumor of the stomach. Choi et al. 11 reported a 56-year-old man with synchronous primary gastric adenocarcinoma, mucosa-associated lymphoid tissue lymphoma, and schwannoma. Accordingly, we suspect that the occurrence of multiple synchronous tumors in the digestive tract is not just random, regardless of whether the combination is benign, malignant, or mixed. There might be an association between adenoma and adenocarcinoma of the GB or stomach with gastrointestinal mesenchymal tumors. There also may be an association between gastrointestinal mesenchymal tumors and adenomas of the digestive tract, such as in similar epidemiology, potential carcinogens, or shared or crossed pathogenetic molecular pathways.1,8,12 These issues require further validation and investigation in clinical practice.
The combination of tumors in our case, although rare, was relatively easy to treat because they could be excised entirely and did not shown malignant transformation. A thorough examination is warranted if a tumor occurs at one site of the digestive system.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231163049 - Supplemental material for Gastric schwannoma coexisting with tubular adenoma of the gallbladder: a rare combination
Supplemental material, sj-pdf-1-imr-10.1177_03000605231163049 for Gastric schwannoma coexisting with tubular adenoma of the gallbladder: a rare combination by Meng Cai, Xiaodi Chen, Yang Peng, Yufei Liu and Chang Zhou in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231163049 - Supplemental material for Gastric schwannoma coexisting with tubular adenoma of the gallbladder: a rare combination
Supplemental material, sj-pdf-2-imr-10.1177_03000605231163049 for Gastric schwannoma coexisting with tubular adenoma of the gallbladder: a rare combination by Meng Cai, Xiaodi Chen, Yang Peng, Yufei Liu and Chang Zhou in Journal of International Medical Research
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
The patient provided informed written informed consent for treatment and the publication of potentially identifiable images or data included in this article. The reporting of this study conforms to the CARE guidelines. 13 The study was approved by the Yichang Central People’s Hospital Ethics Committee (approval number: 2021-070-01).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.