
Abstract
Objective
To develop a predictor of early surgical intervention in patients with adhesive small-bowel obstruction (ASBO), to optimise treatment strategies and improve patient outcomes.
Methods
A retrospective analysis was conducted of patients with ASBO between August 2019 and June 2024. Clinical, laboratory and imaging data were analysed. A scoring system was developed using C-reactive protein (CRP) concentration, white blood cell (WBC) count, body mass index (BMI), and imaging findings.
Results
The developed ASBO surgical score predicted the need for early surgery with a sensitivity of 89.6%, a specificity of 87.3%, and an area under the curve of 0.88. Patients with a score of 5 to 7 were significantly more likely to require surgical management: 75% of these patients underwent surgery, versus 4.2% in the Conservative treatment group. Key predictors of the need for surgery were high CRP concentration (>54.3 nmol/L), high WBC count (>11.0 × 109/L), BMI <22 kg/m2, maximum small intestinal diameter on computed tomography images >3.85 cm, and free fluid in the abdominal cavity.
Conclusions
The ASBO surgical score is a practical tool that should aid in the timely identification of patients requiring surgical intervention, and may reduce the risk of complications and improve the outcomes of patients.
Keywords
Introduction
Adhesive small-bowel obstruction (ASBO) is a common complication of abdominal surgery, and accounts for approximately 60% to 75% of cases of small-bowel obstruction.1,2 Despite the high incidence of ASBO, there is currently no standard treatment protocol, and therefore the management strategy used often depends on the clinical experience of the surgeon. Most patients experience improvements in symptoms and clinical findings of over 70% without surgical intervention.3,4 However, delays in surgical intervention are closely associated with higher mortality and morbidity, as well as prolonged hospital stays. Previous studies have shown that if surgical intervention is delayed for more than 4 days, the mortality rate can increase by over 60%.5,6 This greater mortality is linked to complications such as small-bowel ischemia, gangrene, bacterial translocation, and perforation.
Although various guidelines have been issued that were based on the evaluation of conservative and surgical treatment options for patients with ASBO, delays in surgical treatment continue to occur in clinical practice.7,8 Therefore, the early identification of patients who require surgical intervention is crucial. To this end, researchers have developed multiparametric scoring systems to predict the need for surgery at the time of emergency admission. These scoring systems are typically based on clinical, laboratory, and imaging data, and aim to improve the recognition of surgical need and reduce the incidences of complications and mortality associated with delayed surgery.
In the present study, we aimed to use recognised clinical, laboratory, and imaging parameters to establish an effective model for the prediction of the need for early surgical intervention in patients with ASBO to optimise treatment strategies and improve patient outcomes.
Materials and methods
We performed a retrospective analysis designed to identify key factors associated with the need for early surgery in patients with ASBO and to create a predictive model. We studied patients admitted to the general surgery departments of Nanjing Yimin Hospital and The First Central Hospital of Baoding between August 2019 and June 2024. The inclusion criteria were as follows: age ≥18 years, ASBO diagnosed using the clinical presentation and imaging findings, a history of previous abdominal surgery leading to adhesion formation and admission to the general surgery departments of Nanjing Yimin Hospital or The First Central Hospital of Baoding between August 2019 and June 2024. The exclusion criteria were as follows: newly diagnosed or recurrent intra-abdominal cancer; bowel obstruction owing to strangulation, intra-abdominal hernia, closed-loop obstruction, or bowel ischemia; obstruction owing to intraluminal foreign body, obstructive enteroliths, or other non-adhesive aetiologies; and missing relevant clinical, laboratory or imaging data.
All the patients enroled in the study underwent abdominal computed tomography (CT) examination upon admission. Patients with either matted or single-band adhesions comprised the sample. We collected clinical, laboratory, and imaging data for these patients from the hospitals’ health information systems. The data collected were the demographic characteristics (age and sex), patient history (of previous surgery, whether related to cancer or other conditions, and of chemotherapy or radiation therapy), clinical characteristics (symptoms and signs present at admission, including abdominal pain, vomiting, abdominal tenderness, and rebound tenderness), laboratory data (including white blood cell (WBC) count, C-reactive protein (CRP) concentration, and the total, direct, and indirect bilirubin concentrations) and imaging data (the findings of abdominal X-ray and CT performed at admission, focusing on the maximum diameter of the small intestine and the presence or absence of free fluid in the abdominal cavity) of the patients. We developed an ASBO surgical need scoring system using the key parameters previously described. 9 The scoring criteria were as follows: CRP concentration 54.3 nmol/L: 1 point, WBC count >11.0 × 109/L: 1 point, body mass index (BMI) <22 kg/m2: 1 point, maximum diameter of the small intestine on CT images >3.85 cm: 2 points, and presence of free fluid in the abdominal cavity on CT images: 2 points.
Before surgical intervention was considered, all the patients received standard conservative management, which included gastrointestinal decompression (the insertion of a nasogastric tube to relieve intraluminal pressure and reduce vomiting), fluid and electrolyte management (the intravenous administration of fluids to correct dehydration and electrolyte imbalances), bowel rest (to avert further intestinal distention, the patients were subjected to a fasting protocol), monitoring (regular assessment of vital signs, abdominal examinations, and monitoring for signs of deterioration) and supportive care (the administration of analgesics and antiemetics as required to maintain patient comfort).
An exemption was provided by the institutional review board regarding the requirement for ethics approval because of the retrospective nature of the study. The investigators de-identified all the patient information. The reporting of the study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 10 Written informed consent was obtained from all of the participants. The study was conducted in accordance with the principles of the Declaration of Helsinki of 1975, as revised in 2013.
Statistical analysis
The normality of continuous datasets was initially evaluated, and the Kolmogorov–Smirnov test was used to further assess the distribution. Categorical datasets are summarised using frequencies and percentages and continuous datasets are summarised using mean ± standard deviation or median (interquartile range) according to the data distribution. The groups were compared using the independent samples t-test, the Mann–Whitney U test, or the chi-square test, as appropriate. Receiver operating characteristic (ROC) curve analysis was employed to determine the optimal threshold for surgical need. P < 0.05 was considered to indicate statistical significance. Statistical analyses were conducted using IBM SPSS software version 26.0 (IBM Corp., Armonk, NY, USA).
Results
We analysed the characteristics and clinical parameters of patients with ASBO who underwent surgery or conservative treatment. A total of 108 patients were included, of whom 12 underwent surgery and 96 underwent conservative treatment.
Table 1 summarises the demographic and clinical characteristics of the two groups. The mean age of patients in the Surgery group was 63.4 ± 12.6 years, and that of patients in the Conservative treatment group was 65.1 ± 10.8 years. The sex distribution of the two groups was similar (8 men and 4 women in the Surgery group, and 60 men and 36 women in the Conservative treatment group). However, the mean BMI of the Surgery group (21.5 ± 2.8 kg/m2) was lower than that of the Conservative treatment group (24.6 ± 3.2 kg/m2) (p = 0.013).
Comparison of the characteristics of patients in the Surgery and Conservative treatment groups.

Data are mean ± SD, numbers, or numbers (percentages). The groups were compared using the independent samples t-test, Mann–Whitney U test or chi-square test, as appropriate.
BMI, body mass index; ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease.
The surgical history of the two groups was comparable, with 75.0% of the Surgery group and 72.9% of the Conservative treatment group having undergone surgery previously. The American Society of Anesthesiologists (ASA) classification and the prevalences of comorbidities, including of pulmonary, renal, cardiovascular, and chronic obstructive pulmonary disease, diabetes, smoking, and hypertension, did not significantly differ between the groups.
Table 2 shows a comparison of the clinical data for the two groups. The mean initial WBC count was significantly higher in the Surgery group (15.2 ± 4.5 × 109/L) than in the Conservative treatment group (11.3 ± 3.6 × 109/L) (p < 0.001). Similarly, the mean CRP concentration was higher in the Surgery group (431 ± 147 nmol/L) than in the Conservative treatment group (292 ± 122 nmol/L) (p = 0.028). The mean maximum diameter of the small intestine, measured on CT images, was significantly larger in the Surgery group (5.2 ± 1.1 cm) than in the Conservative treatment group (3.8 ± 0.9 cm) (p = 0.007). Finally, free abdominal fluid was present in 66.7% of the patients in the Surgery group, but only 25.0% of those in the Conservative treatment group (p < 0.001).
Comparison of the clinical parameters of the patients in the Surgery and Conservative treatment groups.

Data are mean ± SD or numbers (percentages). The groups were compared using the independent samples t-test or Mann–Whitney U test, as appropriate.
WBC, white blood cell; CRP, C-reactive protein.
Table 3 shows the results of the logistic regression analysis, which identified several significant risk factors for the need for early surgery in patients with ASBO. The odds ratios (ORs) and 95% confidence intervals (CIs) for each parameter were as follows: BMI: OR 1.502, 95% CI 1.103 to 1.793, p = 0.027; initial WBC count: OR 1.253, 95% CI 1.098 to 1.575, p = 0.02; CRP concentration: OR 1.021, 95% CI 0.835 to 1.074, p = 0.014; maximum diameter of the small intestine: OR 1.045, 95% CI 0.923 to 1.164, p = 0.002; and the presence of free abdominal fluid: OR 1.322, 95% CI 1.212 to 1.602, p = 0.033.
Results of the logistic regression analysis to identify risk factors for the need for early surgery in the patients with adhesive small-bowel obstruction.
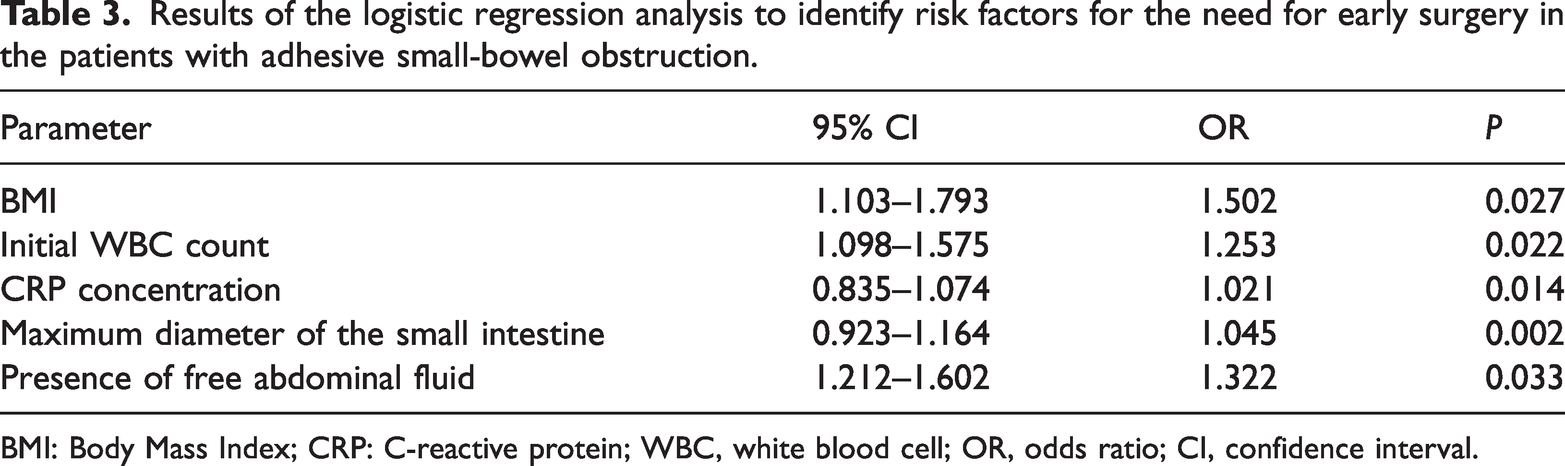
BMI: Body Mass Index; CRP: C-reactive protein; WBC, white blood cell; OR, odds ratio; CI, confidence interval.
Table 4 shows the distribution of the ASBO surgical scores for the patients in the Surgery and Conservative treatment groups. The score stratified the patients according to their need for surgical intervention. None of the patients in the Surgery group had scores of 0 to 2, whereas 74 (77.1%) of those in the Conservative treatment group had scores within this range (p < 0.001). However, 75% of the patients in the Surgery group had scores of 5 to 7, whereas only 4.2% of those in the Conservative treatment group had scores within this range (p < 0.001).
Distribution of the ASBO surgical scores for the Surgery and Conservative treatment groups.

Data are numbers (percentages) and the groups were compared using the chi-square test.
Table 5 summarises the predictive performance of the various parameters with respect to the need for early surgical intervention. The ASBO surgical score demonstrated the highest sensitivity (89.6%) and specificity (87.3%), with an area under the ROC curve (AUC) of 0.88 (p < 0.01). In addition, BMI, the initial WBC count, the CRP concentration, the maximum diameter of the small intestine, and the presence of free abdominal fluid showed significant predictive value, with AUCs ranging from 0.58 to 0.65.
Prediction of the need for early surgery in patients with adhesive small bowel obstruction.

BMI: Body Mass Index; CRP: C-reactive protein; WBC, white blood cell; ASBO, adhesive small-bowel obstruction; AUC, area under the receiver operating characteristic curve.
Figure 1 presents the results of the ROC analysis of the potential risk factors for the need for early surgery in the patients. The ASBO surgical score exhibited the best predictive ability, indicating its potential utility in clinical decision-making regarding timely surgical intervention.

Results of the ROC analysis of potential risk factors for the need for early surgery in patients with ASBO. ROC, receiver operating characteristic; ASBO, adhesive small-bowel obstruction; BMI, body mass index; CRP, C-reactive protein; WBC: white blood cell.
Discussion
ASBO remains a common challenge in postoperative care, with a substantial proportion of patients experiencing this complication following abdominal surgery. Despite advances in surgical techniques and postoperative care, the management of ASBO continues to rely heavily upon clinical judgment, which leads to variation in treatment strategies. Recent studies have shown the importance of timely surgical interventions to prevent complications such as bowel ischemia, necrosis, and perforation, which are associated with higher levels of mortality and morbidity.11–13 Current research focuses on the development of reliable predictive models to aid with the early identification of patients who require surgery.14,15 These models typically incorporate clinical, laboratory, and imaging data and are intended to improve decision-making processes. However, the lack of a standard approach and the variation in the accuracy of the models indicate the need for their further refinement and validation.
In the present study, we have identified several predictors of the need for surgical intervention in patients with ASBO: low BMI, high WBC count, high CRP concentration, a large maximum diameter of the small intestine on CT images, and the presence of free abdominal fluid. These factors were used to create a scoring system that demonstrated high sensitivity (89.6%) and specificity (87.3%), implying that it may be clinically useful. Logistic regression analysis confirmed the independent predictive value of each of the parameters. A high CRP concentration and a high WBC count suggest the presence of an inflammatory response, which may be indicative of complications such as bowel ischemia or necrosis that necessitate surgical intervention. Similarly, a large maximum diameter of the small intestine and the presence of free fluid may reflect more severe obstruction or the presence of complications such as perforation, which are further indications for surgery.
These findings imply that the ASBO surgical score provides a quantitative method of stratifying patients according to their risk of requiring surgery. This stratification is crucial in emergency settings, where timely decision-making can significantly affect patient outcomes. By identifying high-risk patients early, clinicians can prioritise surgical consultations and interventions, thereby potentially reducing delays to surgery and improving recovery rates.
The implementation of the ASBO surgical score in clinical practice would have several advantages. It would serve as a support to clinical decision-making that could be used alongside clinical judgment to improve the accuracy of the prediction of surgical need.16,17 This tool would be particularly useful in settings with limited resources, where rapid and accurate decision-making is essential. 18 Moreover, it should aid patient communication by providing a clear rationale for the recommended treatment approach. By quantifying the risk, healthcare providers can better explain the necessity of surgical interventions to patients and their families, thereby facilitating shared decision-making and making informed consent easier to obtain.19,20
In the present study, we identified several risk factors for the need for early surgical intervention in patients with ASBO. These were BMI, high WBC count, high CRP concentration, a large maximum diameter of the small intestine on CT images, and the presence of free abdominal fluid on CT images. These risk factors are consistent with those previously reported. High values of markers of inflammation have been consistently shown to be associated with the need for surgical intervention in patients with ASBO. For instance, Friziero et al. demonstrated that a high neutrophil-to-lymphocyte ratio predicts bowel ischemia in patients with non-strangulated ASBO. 16 In addition, the importance of CT imaging in patients with ASBO has been well documented. Studies such as that of Zins et al. have shown that findings such as bowel dilation and free fluid predict the need for surgery. 17 Furthermore, although less frequently highlighted, other studies have shown that low BMI may be associated with poor physiological reserves, and therefore a higher risk of complications that necessitate surgery.21,22
Several predictive scoring systems have been developed to assess the risk of a failure of conservative management in patients with ASBO. Paisant et al. developed a predictive model that included factors such as age, a previous history of obstruction, and CT findings, and the authors emphasised the importance of clinical and radiological parameters in decision-making. 23 Kim et al. developed a scoring system that was based on radiological features, such as the degree of obstruction and signs of ischemia, and emphasised the predictive value of specific CT findings. 24 Maraux et al. identified risk factors, including high values of markers of inflammation and surgical history, and suggested that the use of a combination of clinical and laboratory data enhances the accuracy of the prediction. 25 Finally, Cosse et al. developed a clinical score that focused on the use of symptoms and laboratory results to predict the need for surgery and included parameters such as the severity of pain, vomiting, and leukocytosis. 26 The ASBO surgical score developed in the present study is consistent with these models with respect to the integration of clinical, laboratory, and imaging data.
Despite its promising results, the present study had limitations that must be acknowledged. Its retrospective design may be associated with selection bias because the data were collected from patient records, which might not have included all the relevant data. In addition, the study was conducted in two hospitals, which may limit the generalisability of the findings to other settings with different patient demographics or healthcare practices. The sample size was sufficient for this initial analysis, but further studies should be performed of larger samples to enhance the robustness of the findings. Large, multi-centre studies would provide a more comprehensive evaluation of the ASBO surgical score and its applicability to a diverse range of populations.
Future research should take the form of prospective studies that aim to validate the use of the ASBO surgical score. Such studies would help confirm the accuracy and reliability of the score in real-world clinical settings. In addition, the inclusion of other biomarkers or advanced imaging data could further refine the predictive ability of the model. Further research could also investigate the effects of implementing the ASBO surgical score on clinical outcomes, such as the time between admission and surgery, the duration of the hospital stay, and overall recovery. A better understanding these effects would provide valuable insight into the practical benefits of the scoring system and its role in improving healthcare delivery.
Conclusion
We have developed a valuable model for the prediction of the need for early surgical intervention in patients with ASBO. The ASBO surgical score offers a practical, evidence-based tool for clinicians, which should improve their ability to make timely and informed decisions. Although further validation and research are necessary, the model holds significant promise as an approach to improving patient outcomes and optimising the management of ASBO. By continuing to refine and validate this tool, the medical community can better address the challenges associated with ASBO and enhance the quality of the care provided to patients.
Footnotes
Acknowledgements
The authors would like to thank the patients for their cooperation and consent for publication of this report.
Author contributions
Yanhao Sun drafted the manuscript. Yuanfang Sun performed the literature review and the surgical procedures. Yilong Hu collected and analysed the data. All the authors read and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.