
Abstract
Single-port laparoscopic technology has become increasingly more popular in China as economic levels and medical technology have both improved. The advantages of single-port laparoscopic technology, such as less surgical trauma, quick recovery and less postoperative skin scarring, have been unanimously recognized and appreciated by patients. However, this technology has not been developed in Africa, which has relatively limited medical and surgical resources. The medical team of the Affiliated Hospital of Nantong University in Africa successfully performed a single-port laparoscopic giant nephrectomy in a patient who presented to Mnazi Mmoja Hospital, Zanzibar, Tanzania. The patient recovered well after surgery. This current case report demonstrated that single-port laparoscopy successfully treated giant hydronephrosis for the first time in Africa.
Introduction
Hydronephrosis is a serious secondary condition resulting from urinary tract obstruction. It is characterized by sterile urine-filled dilation of the renal pelvis and calices on one or both sides. Most patients with hydronephrosis are in a serious condition, so timely and effective treatment must be carried out in order to prevent complications such as infection and/or kidney stones, which will have a considerable negative impact on their subsequent renal function. Imaging methods for the diagnosis of hydronephrosis include intravenous urography, computed tomography (CT) and B-scan ultrasonography. Giant hydronephrosis is usually asymptomatic and may be incidental to unrelated intraperitoneal symptoms on imaging or in patients with chronic back pain and elevated creatinine levels. 1 Once giant hydronephrosis is confirmed, renal function should be assessed, as treatment depends on residual renal function and the severity of symptoms. 2 Nephrectomy is usually performed in patients with severe symptoms and poor renal function. 3
This current case report describes a patient with a giant hydronephrosis who was treated using single-port laparoscopic nephrectomy by the 31st China Medical Team at Mnazi Mmoja Hospital, Zanzibar, Tanzania. The patient recovered well after the surgery.
Case report
In March 2022, a single-port laparoscopic giant renal resection, reportedly the first of its kind in Africa, was performed successfully by the 31st China Medical Team in Mnazi Mmoja Hospital, the largest governmental hospital in Zanzibar.
One morning in March 2022, a female in her mid-30s who had experienced recurrent pain in the lower back and abdomen for more than 10 years, suddenly had severe pain in the lower back and abdomen, so she presented to Mnazi Mmoja Hospital, Zanzibar, Tanzania. The physical examination showed a huge bulge in the right lower back and the entire abdomen. With the accompanying pain becoming more and more intense, her everyday life was seriously negatively impacted. At this time, however, the local medical provision was not sufficient to undertake her treatment.
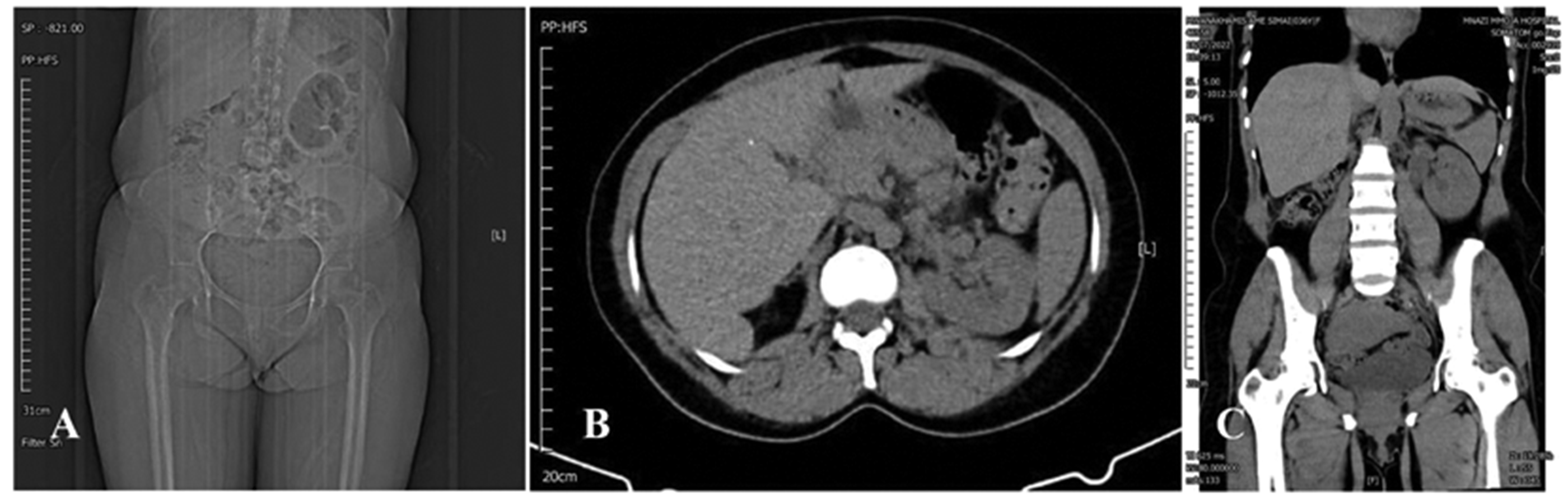
Accompanied by her family, the patient attended Mnazi Mmoja Hospital to ask for help from the 31st China Medical Team. A CT examination found the following: the right kidney was non-functional due to hydronephrosis; the cortex was thin; the right kidney was pressed to the left side of the abdominal cavity; the liver was squeezed by the right kidney’s upper pole; and the pelvic cavity was invaded by the lower pole. The size of the right kidney was measured as 29 * 18 * 15 cm (Figure 1). It was apparent that the condition had reached the point where surgery was necessary.

Computed tomography scans of a female in her mid-30s who had experienced recurrent pain in the lower back and abdomen for more than 10 years, which suddenly became more severe causing her to seek medical treatment: (a) a scan showing severe right giant hydronephrosis crossing the midline with thinning of the renal parenchyma; (b) the right kidney was non-functional due to hydronephrosis, the cortex was thin and the right kidney was pressed to the left side of the abdominal cavity; (c) the liver was squeezed by the right kidney’s upper pole; (d) and the pelvic cavity was invaded by the lower pole.
After repeated consultations within the medical team and thorough consideration of the advantages and disadvantages of various treatment approaches, a decision was made to perform a single-port laparoscopic nephrectomy. Considering the current medical condition and the patient’s health status, the surgical team decided that this operation should be performed by making a 2-cm incision in the patient’s right waist, expanding the right abdominal cavity through the incision, and then inserting a single-port multi-channel puncture into the abdominal cavity, followed by introduction of the laparoscopic system. This was an extremely difficult minimally invasive procedure that was unprecedented in the local geographical area. The patient was adjusted to a left lateral recumbent position with the waist raised. A 2-cm incision was made at the midpoint between the right rib arch and the iliac ridge along the right axillary midline. The muscle layer and lumbar dorsal fascia were expanded with vascular forceps in the direction perpendicular to the skin and the parallel muscle fibres. A self-contained air sac was placed, into which 600 ml of air was filled to expand the potential posterior abdominal space and removed after 2 min. A single-port multi-channel combination kit was inserted, connected to the pneumatic machine and a pneumatic pressure of 12 mmHg was maintained. After satisfactory aeration, a laparoscope and operating instruments were inserted.
The perirenal fascia was opened and separated along the surface of the psoas major muscle towards the renal hilum. The renal artery was dissociated, ligated with a hem-o-lok clamp and cut off. The renal vein was dissociated, ligated and cut off in the same way. Blunt separation of the dorsal side of the inferior pole was performed along the surface of the psoas major muscle to locate the dilated ureter, which was ligated and cut off. Separation was performed close to the dorsal side of the kidney, up to the upper pole of the kidney and down to the lower pole. A 0.5-cm incision was made on the surface of the kidney and then approximately 4000 ml of the yellowish liquid was aspirated out of the kidney with a suction device to shrink the kidney and expand the posterior abdominal space, so that the peritoneum that had been pushed by the huge kidney to the left side of the body could be retracted to the right side for separation. Then the incision in the kidney was closed so that the remaining fluid inside the kidney would not leak out and partial tension in the kidney could be maintained.
The fat sac was completely cut open longitudinally along the lateral margin of the kidney to the front and the position of peritoneal fold was carefully identified after the extraperitoneal adipose tissue was cleaned. Then, the ventral side of the kidney was dissociated starting from the lower pole of the kidney to the upper pole. During the separation process, strict haemostasis was done and peritoneum damage was repaired in time. When the whole kidney was dissociated except for the upper pole, the kidney was opened for the second time and approximately 2000 ml of residual fluid was sucked out. At this time, the right kidney was hanging at the top of the diaphragm without tension. As a result, the posterior abdominal cavity was large and the operative field was clear. The upper pole of the right kidney was severed with an ultrasonic knife before the whole right kidney was resected. The cystic atrophic kidney was directly removed after the operating instruments were taken out and the single port was turned on. After the pneumoperitoneum was established again, laparoscopy and operating instruments were inserted, the pneumoperitoneum pressure was lowered. When no obvious active bleeding was detected at the renal pedicle vascular ligation site and wound surface, the single-port was removed, a silica gel drainage tube was placed in the incision, and the drainage tube was fixed with sutures and the incision was closed layer by layer (Figure 2). Postoperative pathology revealed that the kidney tissue exhibiting marked thinning and atrophy of the parenchyma with cystic dilatations lined by flattened cuboidal epithelium fibrosis and inflammation was also noted.

Representative photographs showing the preoperative, intraoperative and postoperative status of a female in her mid-30s who had experienced recurrent pain in the lower back and abdomen for more than 10 years, which suddenly became more severe causing her to seek medical treatment: (a) the patient in a preoperative supine position; (b) the right side of the patient’s preoperative supine position; (c) a single port was placed into the right waist area during the operation; (d) the atrophied kidney was removed via the single port; (e) the atrophied renal vessels were ligated using a vascular clip; (f) the patient’s postoperative outpatient review in the supine position and (g) the patient’s postoperative outpatient review of the right side of the waist area (visible surgical wound). The colour version of this figure is available at: http://imr.sagepub.com.
After the operation, a postoperative evaluation was made, which showed that the patient’s trauma was greatly reduced compared with traditional open surgery and ordinary laparoscopic surgery. The kidney, which was more than 10-times larger than the incision itself, was successfully removed through the 2-cm incision. The patient recovered well after surgery, the abdomen was significantly reduced and the incision healed well without any complications. Three months later, the patient came to the hospital for re-examination. She had no uncomfortable symptoms and all of her indicators were normal. The patient and her family were very satisfied with the treatment outcomes (Figures 2 and 3).
Computed tomography (CT) scans of a female in her mid-30s who had experienced recurrent pain in the lower back and abdomen for more than 10 years, which suddenly became more severe causing her to seek medical treatment: (a) postoperative CT plain film scan of the patient’s abdomen; (b) postoperative CT scan of the cross section of the patient’s abdomen and (c) postoperative CT scan of the coronal plane of the patient’s abdomen.
All patient details have been removed to ensure patient privacy and written informed consent was obtained from the patient prior to treatment. Because all patient details were de-identified, written informed consent for publication was not required. In addition, because of the nature of this study (case report), formal ethics committee approval was not required. The reporting of this study conforms to the CARE guidelines. 4
Discussion
Giant hydronephrosis is a slowly progressive disease that can sometimes only present as a huge abdominal mass. 5 It is a rare disease of the urinary tract system that has been defined in the literature as having more than 1000 ml of urine in the renal collection system or having more than 1.6% of the total weight of the kidney.6,7 Giant hydronephrosis may result from multiple causes such as a chronic obstruction of the distal ureter. 8
Up to 2015, more than 600 cases of giant hydronephrosis have been reported worldwide, most of which have been detected by B-scan ultrasonography, CT and magnetic resonance imaging. 3 The treatment of giant hydronephrosis often depends on the diagnosis and most cases are treated with simple nephrectomy or renal sparing therapy. 1 Atrophic nephrectomy is a high-risk, difficult operation that requires a professional medical team and comprehensive postoperative care measures to ensure the success of the surgery and the patient’s recovery. The huge kidney, which has accumulated water for a long time, is closely adhered to the surrounding tissues and important organs due to inflammation and other reasons, and the range of motion of the single-hole trocar is very small. The following complications during and after surgery may occur: (i) bleeding: the kidneys have a large blood supply and severe bleeding may occur during surgery, which could even lead to haemorrhagic shock; (ii) infection: postoperative infection is a common complication that requires close monitoring and prompt management; (iii) damage to adjacent organs: adjacent organs, such as the duodenum and pancreas, may be damaged during surgery resulting in postoperative complications; (iv) renal insufficiency: when one kidney is removed, the other kidney might not be able to fully compensate, resulting in renal insufficiency. Dialysis treatment is required in severe cases; (v) anaesthesia risks: reaction to anaesthetic medications may lead to intraoperative or postoperative complications. Thus, the indications for surgery should be carefully reviewed for each patient. With the further improvement of surgical instruments, the continuous accumulation of clinical experience and the completion of prospective large-sample multicentre clinical randomized controlled studies with optimized design, single-port laparoscopic technology is likely to play a greater role in the diagnosis and treatment of urological diseases.
Since its first report in 2007, 9 Laparo-Endoscopic Single-Site Surgery (LESS) has made significant progress in urology. LESS technology, while inheriting the characteristics of traditional laparoscopic techniques, offers unique advantages such as better postoperative cosmetic results and faster patient recovery. 10 With the development of laparoscopic technology in China for 30 years, many patients with giant hydronephrosis have benefited from the minimally invasive approach. Compared with traditional open surgery and conventional laparoscopy, single-port laparoscopy can greatly reduce patient trauma and speed up postoperative recovery. Reports have demonstrated that simple gasless single-port laparoscopy is suitable for use in middle- and low-income countries or primary hospitals. 11 Although single-port laparoscopic nephrectomy has become a major surgical method at home and abroad, and its safety and feasibility have been clinically recognized, the medical provision in Zanzibar remains relatively limited so this minimally invasive approach has not been carried out previously. This was the first single-port laparoscopic nephrectomy undertaken for giant hydronephrosis in Africa. The success of this operation in the current case has demonstrated that the Chinese medical team’s ability to carry out minimally invasive surgery in Africa has reached an international level of quality. Of course, the success of this single-port laparoscopic giant nephrectomy is encouraging, but the limitations of a single case report require further research to confirm its broad applicability. Some of the potential challenges for this surgical approach are poor exposure, instrument collision interference and difficult stitching. These potential challenges could be mitigated by placing the patient in the correct surgical position, selecting the appropriate surgical incision point and operating with robot assistance. These minimally invasive methods will not only improve the success rate of surgery, but also provide valuable experience and reference for other practitioners.
In conclusion, this current case report describes an unusual case of giant hydronephrosis managed successfully using single-port laparoscopy for the first time in Africa. The kidney, which was more than 10-times larger than the incision itself, was successfully removed through the 2-cm incision. The success of this single-port laparoscopic giant nephrectomy is encouraging, but further research to confirm its broad applicability is required.
Footnotes
Acknowledgements
We are thankful to the patient and all the physicians and technicians who participated in this case report.
Author contributions
H.L. and F.L: research idea and study design. H.L. and L.Q.: data acquisition, data analysis/interpretation. L.Q. and F.L.: statistical analysis and supervision or mentorship. F.L. takes responsibility that this study has been reported honestly, accurately and transparently, and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.