
Abstract
Laryngeal masks are widely used by anesthesiologists in clinical practice because of their advantages of no tracheal injury, minimal airway stimulation, limited airway tissue invasion, and easy implantation and airway establishment. We herein describe a patient with congenital heart disease who developed unilateral sublingual nerve paralysis after application of a laryngeal mask airway. The patient reported perioral numbness and exhibited unclear speech and slight right deviation of the tip of the tongue after surgery. On physical examination, the patient had normal muscle strength, symmetrical frontal lines, normal occlusion, and a normal nasolabial groove. We performed head computed tomography and computed tomography angiography to rule out cerebrovascular disease, and no abnormalities were found. The patient’s imaging findings and clinical symptoms suggested unilateral right sublingual nerve palsy. After active treatment, the patient’s symptoms improved by 75% on the third postoperative day and by 90% on the fifth postoperative day. Despite the extremely low incidence of sublingual nerve palsy after application of a laryngeal mask airway, anesthesiologists should be aware of this complication. Although the nerve palsy can resolve spontaneously, the nerve damage may be permanent.
Keywords
Introduction
Laryngeal masks are widely used by anesthesiologists in clinical practice because of their advantages of no tracheal injury, minimal airway stimulation, limited airway tissue invasion, and easy implantation and airway establishment. 1 However, laryngeal masks also have some drawbacks such as sore throat, air leakage, and displacement. 2 Sublingual nerve injury associated with a laryngeal mask airway (LMA) is a rare complication, but it can cause severe symptoms such as dysarthria and speech impairment, taste loss, and numbness. 3 We conducted a PubMed search and found a total of 23 articles on sublingual nerve paralysis after LMA application.3–25 The patients described in these reports had different degrees of sublingual nerve paralysis after surgery, and they basically recovered completely within 6 months after conservative treatment (Table 1). Notably, these reports mainly involved normal patients. We herein report the first case of unilateral sublingual nerve palsy after use of an LMA in a patient with congenital heart disease.
Comparison of previously published relevant cases.

M, male; F, female; ET, endotracheal; GA, general anesthesia; BMI, body mass index.
Case Presentation
A man in his early 30s (height, 170 cm; weight, 65 kg) was scheduled for arthroscopic left knee exploration and anterior cruciate ligament reconstruction. The patient had no special medical history or family history, and his cardiac function was level I to II.
Cardiac ultrasound suggested congenital heart disease with corrected transposition of the great arteries (SLL type), patent foramen ovale, left and right atrium sizes within the normal range, and an ejection fraction of 62%. An electrocardiogram suggested sinus bradycardia, left deviation of the electrical axis, counterclockwise transposition, abnormal Q waves in the right ventricular leads, and heart rate of 52 beats/minute. Twenty-four-hour Holter electrocardiogram and laboratory findings were unremarkable. The patient’s American Society of Anesthesiologists physical status was grade II.
No preoperative medication was administered before surgery. Upon arrival in the operating room, the patient was given midazolam 2 mg, granisetron 3 mg, propofol 1.5 mg/kg by continuous intravenous infusion, sufentanil 0.2 µg/kg, cisatracurium 0.15 mg/kg, and dopamine 4 mg/hour by pump infusion. When the relaxant was fully effective, we successfully inserted a tetracaine-infiltrated laryngeal mask (size 4.0, Lot #20221115; TuoRen Medical, Changyuan, China) on the first attempt without difficulty using the standard insertion technique with 30 mL of air and no gas leakage with pressure-controlled ventilation. Meanwhile, right radial artery puncture was performed to monitor the patient’s blood pressure, and an ultrasound-guided left saphenous nerve block (15 mL of 0.33% ropivacaine) was administered. With the patient in the supine position, we maintained anesthesia using remifentanil 0.1 to 0.2 µg/kg per minute, propofol 2 mg/kg, sevoflurane 2% (80% oxygen, 2.5 L/minute), bispectral index of 40 to 55, and mean arterial pressure of > 70 mmHg. The patient remained hemodynamically stable during surgery. The operation was very smoothly performed. The operation time was 150 minutes, and the anesthesia time was 180 minutes. The patient was transferred to the postanesthesia care unit after awake extubation at the end of surgery. The patient reported perioral numbness and exhibited unclear speech and slight right deviation of the tip of the tongue (Figure 1(a)). On physical examination, the patient had normal muscle strength, symmetrical frontal lines, normal occlusion, and a normal nasolabial groove. Five hours after the operation, however, the patient reported dysphagia, hoarseness, a vomiting reflex, and normal taste; he had no dyspnea. On physical examination, the right deviation of the extended tongue was aggravated (Figure 1(b)). Head computed tomography and computed tomography angiography were performed to rule out cerebrovascular disease, including cerebral infraction, but no abnormalities were found (Figure 2). The patient’s imaging findings and clinical symptoms suggested unilateral right sublingual nerve palsy. We administered methylprednisolone, vitamin B12, and methylcobalamin, and his symptoms improved by 75% on the third postoperative day and by 90% on the fifth postoperative day (Figure 1(c)). The patient was discharged and continued oral methylcobalamin for 2 to 3 weeks. The patient’s disease course is presented in a timeline in Figure 3. With reference to previous case reports (Table 1), we administered conservative treatment, and the anesthesiologist (L.X.) followed up the patient every week (Figure 4). His symptoms completely disappeared 5 weeks after surgery.
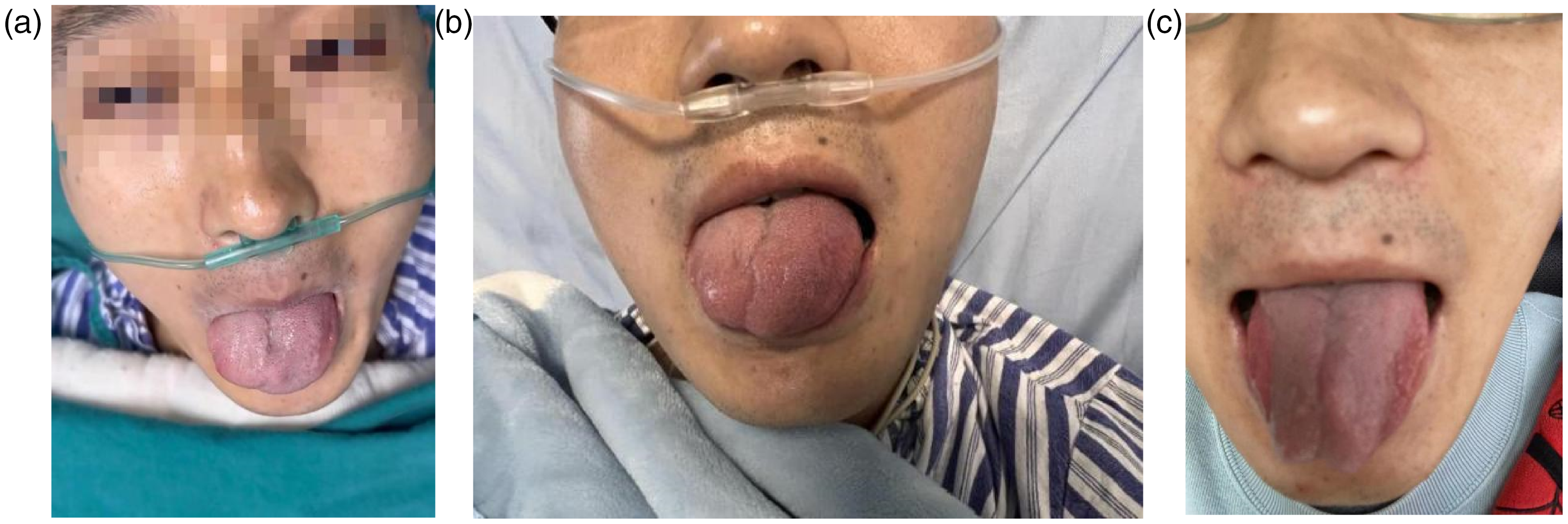
Postoperative clinical findings. (a) Slight deviation of tip of tongue. (b) Aggravation of tongue deviation and (c) Clinical improvement after treatment.

Computed tomography angiography findings.

Timeline of disease course.

Flow diagram of present case.
The patient’s detailed information has been de-identified to the greatest extent possible. For details that could not be de-identified, the patient provided written informed consent for publication. The patient also provided written informed consent for treatment after acquiring a full understanding of the treatment options. Ethical approval for this study was given by our hospital’s institutional review board. The reporting of this study is in line with the CARE guidelines. 26
Discussion
More cases of postoperative tongue numbness have been reported in patients undergoing anesthesia using the supraglottic airway technique (e.g., LMA) than in patients undergoing endotracheal general anesthesia. 27 , 28 Potential risk factors for sublingual nerve injury are the use of nitrous oxide, an inappropriate LMA size, the lateral position, and over-rotation. 25 In our case, we selected the appropriate laryngeal mask model according to the patient’s body weight, the patient remained supine during the procedure, the patient had no relevant medical history, and the laryngeal mask was successfully inserted on the first attempt. Thus, none of the above-mentioned risk factors are applicable to our case. Our case suggests that a correctly positioned LMA can occasionally cause nerve damage.
The sublingual nerve originates from the sublingual nucleus within the medulla and leaves the skull via the hypoglossal canal of the occipital bone. At the level of the mandible, it becomes superficial and enters the base of the mouth.3,6 Thus, one possible site of injury is the hyoid bone, where the inflatable cuff on the laryngeal mask can compress the nerve. 29 We suspect that in our case, the nerve damage may have had two causes. First, it may have been due to the insertion of the laryngeal mask. The right part of the tongue may have flipped during this process, resulting in unilateral sublingual nerve compression. Second, during the prolonged anesthesia period, we did not continuously adjust the position between the laryngeal mask and the hyoid bone. Sublingual nerve injury has been reported to fully resolve within the first 6 months, although one patient developed permanent recurrent nerve palsy after use of an LMA. 30 This suggests that reversible or permanent damage may occur depending on the pressure and duration of the compression. Therefore, when a patient is diagnosed with sublingual nerve palsy caused by an LMA, clinicians should consider a follow-up period of at least 6 months during which no invasive surgery is performed because spontaneous recovery is usually required.
The main limitation of this case report is that because of the researchers’ cultural or personal factors, there may be certain deviations in the treatment of the patient’s various conditions during and after surgery.
Conclusion
We have herein reported the first case of unilateral sublingual nerve injury in a patient with congenital heart disease after general anesthesia with an LMA. This original case report serves as an instructive reminder on appropriate use of laryngeal masks for general anesthesia. Risk factors for nerve injury include excessive inflation of the laryngeal mask, the placement method used, aggressive insertion, a prolonged insertion time, and incomplete onset of muscle relaxation.
Despite their low incidence, lingual and recurrent laryngeal nerve palsy may still occur, and although nerve numbness may spontaneously resolve, the neuropathy may be irreversible. Skilled use of medical techniques and compliance with the manufacturer’s instructions for use can help prevent such complications.
Footnotes
Author contributions
LX: Study design, drafting and detailed writing of article, data analysis/interpretation, critical revision of article, approval of article, data collection.
JY: Study design, drafting and detailed writing of article, data analysis/interpretation, critical revision of article, approval of article, data collection.
HL: Study design, drafting and detailed writing of article, data analysis, critical revision of article, approval of article.
ZG: Study design, data analysis, drafting of article, critical revision of article, approval of article.
JH: Data interpretation, data collection, approval of article.
HD: Data interpretation, data collection, approval of article.
Availability of data and materials
The corresponding author can be contacted with data requests.
Consent for publication
Written informed consent was obtained from the patient for both treatment and publication of this case report.
Declaration of conflicting interests
The authors declare that there is no conflict of interest regarding the publication of this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Provenance and peer review
Not commissioned; internally peer-reviewed.