
Abstract
Objective
To compare operative outcomes between single-port laparoscopy (SPL) and conventional laparoscopy (CL) to remove adnexal masses during pregnancy.
Methods
This retrospective case–control study included all patients who had undergone laparoscopic removal of benign adnexal masses during pregnancy between October 2010 and January 2020. Multiple clinical characteristics and operative outcomes were retrospectively analysed and compared between patients who had undergone SPL versus CL, including cosmetic satisfaction with the scar, measured on a 10-point scale (10 indicating very satisfied).
Results
A total of 64 patients were included (SPL, n = 22; and CL, n = 42). Overall scar satisfaction scores significantly favoured SPL versus CL (9.1 ± 1.7 versus 8.1 ± 1.3, respectively), however, surgery duration was significantly longer for SPL than CL (69.2 ± 21.0 min versus 54.7 ± 20.7 min). No incisional hernia was detected in the study. Operative blood loss, decrease in estimated haemoglobin level, length of hospital stay, and hospitalization expenses were comparable between the two groups. Pregnancy and fetal outcomes were not remarkably different.
Conclusion
For removal of benign adnexal masses during pregnancy, SPL may offer superior cosmetic satisfaction versus CL, and was not associated with additional perioperative danger, economic burden, or adverse pregnancy and neonatal outcomes.
Keywords
Introduction
Single-port laparoscopy (SPL) is a surgical technique that was developed from conventional laparoscopy (CL) during the 1970s. 1 As SPL surgery requires only one skin incision, better cosmetic satisfaction is expected compared with CL. The first SPL procedure was introduced for tubal sterilization, and to date, this technique has been applied to urology, gynaecology, and digestive surgeries.2,3
In gynaecology, SPL has been widely evaluated for removal of benign adnexal masses compared with CL. 4 However, the application of SPL during pregnancy has not been well verified. Despite several published reports,5–9 to the best of our knowledge, no retrospective study has evaluated the strengths and weaknesses of SPL and CL for adnexal cystectomy during pregnancy using validated assessments. Thus, concerns remain over SPL management of adnexal masses in pregnant patients. 10
The aims of the present study were to evaluate the operative outcomes of SPL and CL surgeries for benign adnexal masses during pregnancy, and to investigate the feasibility and safety of SPL in pregnant patients.
Patients and methods
Study population
This retrospective cohort study included patients who underwent laparoscopic adnexal surgeries during pregnancy at the Department of Gynaecology, the Obstetrics and Gynaecology Hospital of Fudan University, Shanghai, China, between October 2010 and January 2020. Surgical intervention was deemed to be warranted in cases with a strong suspicion of malignancy; a large mass (>6–10 cm); patient reported symptoms; or an increased risk of torsion, rupture, or obstruction of labour. The inclusion criteria were normal preoperative test values, including complete blood count, electrolytes, chemistry, and coagulation test, and no severe complications, including non-pregnancy-related and pregnancy-related complications. Patients in whom malignant ovarian tumours were suspected by ultrasonography were excluded from the study.
As the present study was a retrospective review of patient data, and the study included deidentified patient data, ethics approval was not deemed necessary. All participants provided written informed consent before the study began for their data to be included in any future medical research. All patient details have been de-identified and the reporting of this study conforms to STROBE guidelines. 11
Perioperative outcomes
Perioperative outcomes were evaluated by collecting relevant data from the medical records, including operative time (interval between skin incision and closure), estimated blood loss (in ml; estimated based on experience), change in haemoglobin level after surgery (estimated before surgery and on the first postoperative day), duration and costs of hospital stay, and intraoperative and postoperative complications. Discharged patients were followed-up by telephone between 6 and 12 months following the operation, to collect data regarding cosmetic results. Patients were asked to rate overall scar satisfaction on a 10-point scale, with 10 indicating very satisfied and 1 indicating very unsatisfied. In addition, pregnancy and neonatal outcomes were followed and recorded.
Operative techniques
The SPL port retractor adopted in this study (Beijing Hangtian KaDi Technology R&D Institute, Ding’an, Hainan, China) consists of four access ports, including two 5-mm ports and two 10-mm ports. A 30° rigid, 10-mm laparoscope was inserted through one of the 10-mm ports. Elongated rigid straight instruments were inserted through other ports. Standardized adnexal cystectomy procedures were performed in both groups and the endobag technique was used to prevent spillage. 12
Under general anaesthesia, the patient was placed in the dorsal lithotomy position with both legs supported in stirrups. A 2.5-cm umbilical incision was made to insert the 4-cm inner ring of a wound retractor to stretch the fascial incision, and the outer ring of the wound retractor was rolled for connecting the sealing member. Except for the number of ports, identical surgical procedures were followed for SPL and for CL. In the SPL group, an extracorporeal surgical approach was employed, as described by Kim et al. 13 To close the umbilical incisions in SPL, the peritoneum, fascia, and skin were sutured separately. The peritoneum and fascia were closed using simple continuous suture with Safil absorbable surgical suture (B. Braun Medical, Barcelona, Spain). Skin closure was performed using subcuticular suture with Surgical Gut Suture (Johnson and Johnson, New Brunswick, NY, USA). Maternal vital signs, oxygen saturation, and end-tidal carbon dioxide pressure were continuously monitored during the operation. Fetal surveillance included sonographic monitoring of the fetal heart rate before and just after the operation. Video footage of the surgical procedure is provided in a Supplemental file.
Statistical analyses
Data are presented as mean ± SD or n (%) prevalence. Between-group differences in quantitative data that displayed normal distribution were analysed using Student’s t-test, while quantitative data without normal distribution were analysed using Wilcoxon rank sum test. Between-group differences in qualitative data were analysed using Fisher’s exact test and χ2-test. All analyses were performed with SPSS software, version 20.0 (IBM, Armonk, NY, USA) and a P value <0.05 was considered to indicate statistical significance.
Results
This study included a total of 64 pregnant female patients who underwent laparoscopic surgeries for benign adnexal masses at the Obstetrics and Gynaecology Hospital of Fudan University during the study period. Of these, 22 patients underwent SPL (34.4%) and 42 underwent CL (65.6%). No differences in patient age, parity, or prevalence of multiple gestation, high-risk pregnancy, or history of caesarean section were found between the two groups (Table 1).
Patient characteristics and properties of adnexal masses in 64 pregnant patients who underwent either single-port laparoscopy (SPL) or conventional laparoscopy (CL).

Data presented as mean ± SD or n (%) prevalence.
aHigh-risk pregnancy: gestational hypertension, chronic hypertension, gestational diabetes, preeclampsia, and other high-risk factors.
No statistically significant between-group differences (P ≥ 0.05).
The mean gestational age was 12.6 ± 4.7 (range, 5–25) weeks in the SPL group and 13.9 ± 4.9 (range, 6–22) weeks in the CL group, with no statistically significant between-group difference (P = 0.320). Among the 10 adnexal torsion cases (15.6% of all cases), three patients underwent salpingo-oophorectomies, while all others underwent cystectomy.
Pathological types of adnexal cysts varied among the study population, and comprised teratoma (28.1% of cysts), endometriotic cyst (18.8%), and serous cystadenoma (15.6%). There were no statistically significant differences in cyst type between the two groups (Table 1).
Overall cosmetic satisfaction with the scar significantly favoured the SPL group (9.1 ± 1.7 versus 8.1 ± 1.3 in the CL group, P = 0.002; Table 2). Regarding wound complication, neither umbilical hernia nor infection was noted in either of the two surgical groups. Postoperative pain results were not investigated as patients were deemed unable to evaluate their postoperative pain precisely due to the long interval between surgery and follow-up (between 6 and 12 months).
Outcomes of single-port laparoscopy (SPL) and conventional laparoscopy (CL) adnexal surgeries in 64 pregnant female patients.
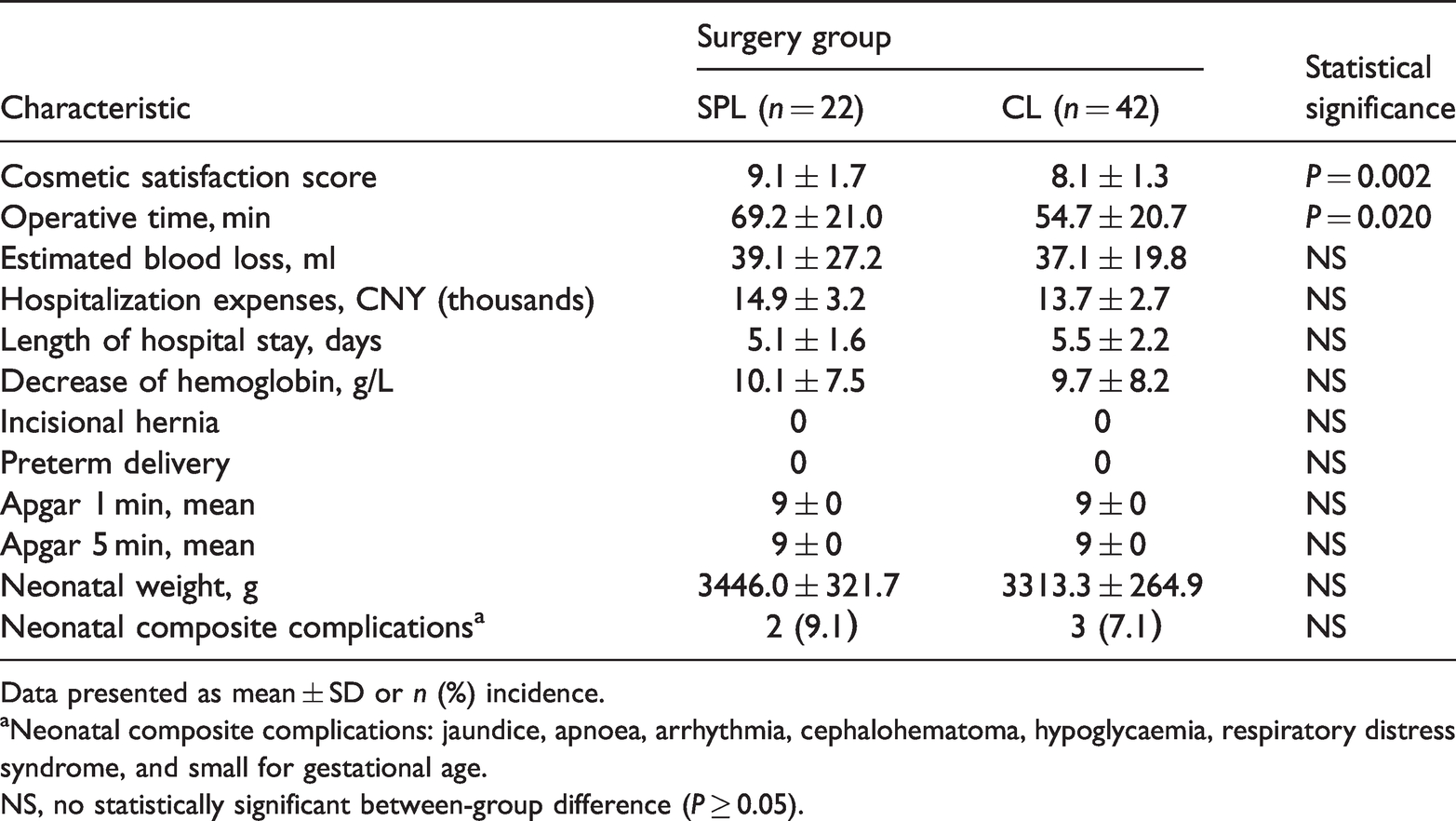
Data presented as mean ± SD or n (%) incidence.
aNeonatal composite complications: jaundice, apnoea, arrhythmia, cephalohematoma, hypoglycaemia, respiratory distress syndrome, and small for gestational age.
NS, no statistically significant between-group difference (P ≥ 0.05).
The mean operative time was significantly different between the two groups (69.2 ± 21.0 min for SPL surgeries compared with 54.7 ± 20.7 min for CL surgeries; P = 0.02). Estimated blood loss was comparable between the two groups (P = 0.948), as was the decrease in estimated haemoglobin level P = 0.779; Table 2). One patient who underwent CL ovarian cystectomy had an estimated blood loss of 400 ml within an operative time of 163 min, and one patient who underwent SPL ovarian cystectomy lost 600 ml of blood with a surgery duration of 130 min. Neither patient required blood fusion or conversion to laparotomy. The average length of hospital stay and hospitalization expenses were not significantly different between the two groups (P = 0.657 and P = 0.245, respectively; Table 2).
Pregnancy and neonatal outcomes are summarized in Table 2. All patients who received SPL or CL adnexal treatment during pregnancy had a full-term delivery. No statistically significant between-group difference in neonatal outcomes was noted regarding Apgar scores at 1 and 5 min and average birth weights. In addition, there was no statistically significant difference in the rate of neonatal composite complications, including jaundice, apnoea, arrhythmia, cephalohematoma, hypoglycaemia, respiratory distress syndrome, and small for gestational age (P = 0.785).
Discussion
To the best of our knowledge, the current study is the largest retrospective investigation of SPL and CL adnexal cystic treatments in pregnant female patients. The main finding was that pregnant patients who underwent SPL adnexal surgery reported better cosmetic satisfaction, and compared with the CL approach, SPL did not increase the risk of adverse events during the perioperative period, economic burden, or adverse maternal or neonatal complications.
The current study showed that, in pregnant patients, SPL had better cosmetic outcomes and patient satisfaction compared with CL, which concurs with the conclusions of several studies in non-pregnant patients.14,15 A possible explanation is that the reduced number of abdominal incisions better meets patients’ cosmetic requirements. Similar cosmetic results for the umbilical incision have been previously shown in SPL surgery and in CL surgery. 16 In addition, several studies have reported less postoperative pain in patients who underwent SPL, and demonstrated that SPL may be associated with shorter hospital stay in addition to less postoperative pain and lower anxiety,9,14,17 which was not evaluated in the present study.
Since laxity of connective tissue and abdominal stress both increase as pregnancy progresses, 18 there are concerns for postoperative hernia formation during pregnancy, particularly on enlarged umbilical incisions in SPL surgery. In the present study, SPL umbilical skin incisions were closed with simple continuous suture of the peritoneum and fascia and subcuticular suture of the skin layer separately. Among these patients, no cases of umbilical hernia or other umbilical incisional complications were noted, providing evidence of the satisfactory healing of single-port umbilical incision in pregnant patients.
No statistically significant between-group differences were noted in respect of other perioperative results. Estimated operative blood loss was similar, and decreases in haemoglobin level were mild in the two groups (10.1 ± 7.5 g/L in the SPL group and 9.7 ± 8.2 g/L in the CL group). The mean length of hospital stay in the SPL group was 5.1 ± 1.6 days, which was not significantly different from that in the CL group at 5.5 ± 2.2 days. The safety of SPL surgery in non-pregnant female patients has been confirmed previously, with operative blood loss and hospital stay similar to that reported for CL.19,20 The presented results provide convincing evidence of the comparable safety and reliability of SPL adnexal surgery versus CL surgery during pregnancy. In addition, the hospitalization expenses were similar between the two groups indicating that there would not be any extra economic burden to patients if SPL was performed instead of CL.
Maternal and neonatal outcomes of SPL and CL adnexal surgery were evaluated in the present study, with no adverse pregnancy results observed, including spontaneous miscarriage or fetal death. These results concurred with a previous study, in which SPL was shown to be a feasible and safe choice for gynaecological surgery during pregnancy. 8 Regarding neonatal outcomes, negligible difference was noted in neonatal morbidity (9.1% versus 7.1%) or Apgar scores. The mean neonatal birth weight in the SPL group was 3446 ± 322 g, which was similar to that in the CL group at 3313 ± 265 g. These results suggest that SPL adnexal surgery during pregnancy does not increase maternal or fetal complication rates compared with CL. The use of conventional laparoscopy for the management of benign adnexal masses in pregnant female patients is also supported by previous studies.21,22 These results should reassure patients and physicians that the SPL technique may be used to remove benign adnexal masses during pregnancy.
Regarding average operative time, SPL adnexal surgery took significantly longer than CL adnexal surgery in the present pregnant female study population (69.2 ± 21.0 min versus 54.7 ± 20.7 min, P = 0.02). Similar results have previously been noted in non-pregnant women, 4 suggesting that an internal factor of the SPL technique leads to longer operative time in SPL adnexal surgery during pregnancy. Possible reasons might be increased surgical difficulty associated with the SPL procedure and more time needed to close a single-port umbilical incision. In a learning curve analysis, 23 an average of 56 operations were required for surgeons to achieve proficiency in SPL adnexal cystectomy. An increased number of procedures may be required to attain proficiency in pregnant cases.
Various single-port retractors have been adopted in SPL gynaecological surgeries,22,23 and a proportion of surgeons have created single ports using surgical gloves. In the present study, commercialized disposable single-port retractors were used for convenience and better airtightness. Nevertheless, with the enlarged gravid uterus, the limited working space increased the surgical difficulty to some extent. From our experience, several approaches may be potentially used to reduce the extended operative time in SPL surgery. In pregnant female patients with large adnexal cysts, SPL provided a perfect site for exteriorized cystectomy and surgical suture of the ovary. In pregnant female patients with a small adnexal mass, extracorporeal surgical ovarian suture may still be performed in SPL surgery to save time. This unique technique simplified the procedure in SPL adnexal surgery and has proved practical and repeatable. In addition, as the endobag technique was widely used in the present surgeries, removal of the specimen from an enlarged umbilical incision without causing rupture became more practical, as the diameter of the SPL umbilical incision often reached 2 cm.
The results of the present study may be limited by several factors. First, the retrospective study design may have resulted in data that were not as reliable as those that would be obtained in a large randomized prospective study. However, a prospective study might need more time to accumulate enough cases. Secondly, a more robust cosmetic evaluation approach, such as the Patient and Observer Scar Assessment Scale (POSAS), 14 could be adopted for a more comprehensive result. Thirdly, the study did not include information on postoperative pain, because the patients were deemed unable to accurately assess pain after a long time following discharge. In future investigations, the authors aim to adopt a more comprehensive approach to cosmetic scar evaluation and implement postoperative pain assessment as an important referential index.
Conclusions
Compared with CL, SPL may provide better cosmetic satisfaction without causing additional perioperative danger, economic burden, or adverse maternal and neonatal outcomes for removal of benign adnexal masses in pregnant patients. However, more experience might be needed to achieve proficiency. By taking its favourable cosmetic advantages and better patient satisfaction into account, SPL may be considered a feasible and safe surgical option for benign adnexal masses during pregnancy.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221128153 - Supplemental material for Single-port laparoscopy versus conventional laparoscopy of benign adnexal masses during pregnancy: a retrospective case–control study
Supplemental material, sj-pdf-1-imr-10.1177_03000605221128153 for Single-port laparoscopy versus conventional laparoscopy of benign adnexal masses during pregnancy: a retrospective case–control study by Sishi Chen, Ganrong Zhang, Keqin Hua and Jingxin Ding in Journal of International Medical Research
Footnotes
Author contributions
Sishi Chen: project development, data Collection, and manuscript writing; Ganrong Zhang: manuscript writing and article submission; Keqin Hua: project development; and Jingxin Ding: project development and manuscript writing
Data accessibility
The authors declare that all data supporting the findings of this study are available within the article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the pubic, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.