
Abstract
Necrotizing fasciitis (NF) is a rapidly progressing condition with a high mortality rate. The poor prognosis is often due to delayed diagnosis, which is typically made clinically or radiologically. This case report highlights a rare instance of fulminant NF with an atypical presentation—no initial clinical signs and an unusual radiological appearance. Both the localization and microbiological findings (non-resistant Klebsiella pneumoniae) were uncommon for NF. The patient presented with no suspicious skin changes, pain, or medical history indicative of NF. A computed tomography scan revealed entrapped air, a pathognomonic sign of NF; however, the air was predominantly located in the abdomen, leading to an initial suspicion of hollow organ perforation because this is an unusual location for NF. Subsequently, NF was suspected based on the computed tomography findings combined with laboratory results. Despite prompt surgical intervention and broad-spectrum antibiotic therapy, the patient died of multi-organ failure within 16 hours. This case underscores the importance of recognizing the subtle and varied presentations of NF and using tools such as the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score. Healthcare providers must maintain a high index of suspicion for NF, even when clinical, radiological, and laboratory findings seem inconspicuous.
Keywords
Introduction
Necrotizing fasciitis (NF) is a rapidly progressing bacterial infection that affects soft tissues, including the skin and subcutaneous layers, extending to the deep fascial planes and causing fulminant necrosis. NF is typically classified into three types.1,2
The most common form, type I (70%–90%), is polymicrobial, involving both anaerobic and aerobic bacteria. Type II is monomicrobial, usually caused by group A streptococci or Staphylococcus aureus.3–7 Type III, which is less common, is caused by Clostridium species. The present report describes a case of NF characterized by several unique features. The patient had the rare type II NF, but the only pathogen identified was Klebsiella pneumoniae, which is unusual for this form. NF caused by K. pneumoniae (hereafter referred to as KP NF) is most often reported in immunocompromised patients1,2,8; our patient was receiving high-dose prednisolone therapy. Geographically, KP NF has a predilection for East Asia, 1 yet our patient was White and treated in a German hospital.
NF can occur anywhere in the body, with the lower extremities affected in approximately 50% of patients.1,3,9 Intra-abdominal cases of NF are rare and typically occur following abdominal surgery.6,10,11 Notably, our patient had no history of abdominal surgery.
Common symptoms described in the literature include disproportionate pain (likelihood ratio [LR] +4.5), systemic shock (LR +8), skin necrosis (LR +30), hemorrhagic bullae (LR +8), and soft tissue emphysema.8,10 Early signs may include local warmth, skin induration, altered mental status, tenderness, erythema, and swelling.4,7 Aside from leg edema, our patient presented with none of these clinical signs. Although edema, severe pain, and fever are considered the classic triad of NF, swelling is reported in only 10% to 40% of cases.1,4 A 2015 case–control study involving 40 patients with NF revealed a sensitivity of 0.6 and a specificity of only 0.08 for skin swelling. 12
Radiological imaging, particularly computed tomography (CT) and magnetic resonance imaging (MRI), can assist in diagnosing NF by identifying gas inclusions in the soft tissues and along the fascia. CT has a sensitivity of 80%, while MRI, regarded as the gold standard, has a sensitivity of 93%.2,9 The presence of dissecting gas along the fascia without penetrating trauma is pathognomonic for NF. 9 In this case, however, imaging revealed free air in the peritoneal cavity, extending into the thigh through the obturator foramen.
In many reported cases, patients present in critical condition, often in septic shock, with significant clinical symptoms.6,13,14 However, our patient exhibited only moderate swelling and pain that began 39 hours prior to admission. Remarkably, the patient was ambulatory and reported no leg pain upon arrival. Vital signs were normal, with no clinical signs of NF other than leg edema. Unfortunately, despite timely and intensive treatment, the patient died of multi-organ failure within 16 hours of admission.
This article addresses a significant gap in the existing literature by presenting an unusual case of NF, highlighting the critical role of the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score and imaging techniques in the diagnosis and management of NF. By illustrating the diverse clinical presentations of NF, which can often appear deceptively benign, we aim to enhance the understanding of this condition and promote the use of the LRINEC score in clinical practice, particularly given that monobacterial NF in the abdomen has not been previously documented in the literature.
The reporting of this study conforms to the CARE guidelines. 15
Patient information
All patient details have been de-identified to maintain privacy and confidentiality. The patient provided written informed consent for the operation and verbal informed consent for all other treatments.
A man in his 60s presented to our orthopedic and trauma department with a 2-week history of progressively worsening bilateral leg edema and a 15-hour history of pain in both legs. Laboratory results from his general practitioner revealed an elevated creatinine level.
His medical history was significant for chronic obstructive pulmonary disease, obesity, atrial fibrillation with pulmonary edema 19 months previously, arterial hypertension, Crohn’s disease, urethral stricture, and bilateral hip prostheses (right side 20 years prior and left side 13 years prior). Additionally, the patient had received an orthopedic injection in the left knee 25 months prior.
The patient’s medication regimen included 11 drugs, most notably high-dose oral prednisolone (40 mg/day), anticoagulation therapy with apixaban, and analgesic therapy with transdermal fentanyl (50 µg/h) and oral tramadol (50 mg, three times daily).
During the past 12 months, the patient had been hospitalized three times for acute heart and kidney failure, but he was discharged home after each admission.
Clinical findings
At the pretreatment clinic, the patient presented with tachycardia (100 beats/minute), anasarca, and severe swelling in both legs and the left arm. However, his body temperature remained within the normal range. Physical examination revealed no signs of acute inflammation, dyspnea, or tenderness in the abdomen.
During our initial examination, the patient was able to walk, was fully oriented, and reported no pain. His vital signs were stable, with a blood pressure of 130/79 mmHg, heart rate of 119 beats/minute, body temperature of 36.4°C, and peripheral oxygen saturation of 95% despite his history of chronic obstructive pulmonary disease. Physical examination revealed significant edema in the legs and arms, as well as a distended but soft and non-tender abdomen. Importantly, there were no clinical signs of NF as described by Wong and Wang, 16 such as tenderness, erythema, skin warmth, crepitus, skin fluctuation, or bullae. No entry wounds for infection were identified.
Initial laboratory tests indicated renal failure, followed by signs of nonspecific inflammation and sepsis, with evidence of ongoing organ failure. Although the individual blood results used to determine the LRINEC score were unspecific, the scores were as follows: not taken, 10, 7, 9, and 9 (see Diagnostic assessment section).
A CT scan showed gas inclusions in both legs, the left gluteal region, and the bladder wall, as well as free air in the abdominal cavity.
Surgical exploration confirmed a complete presentation of NF (see Diagnostic assessment section). Blood cultures identified a monomicrobial infection with non-resistant K. pneumoniae (see Diagnostic assessment section).
Timeline
The hospital course was relatively short, which is common for NF, although the onset of symptoms was unusually prolonged. The patient reported progressively increasing edema in both legs over a 2-week period (Figure 1).
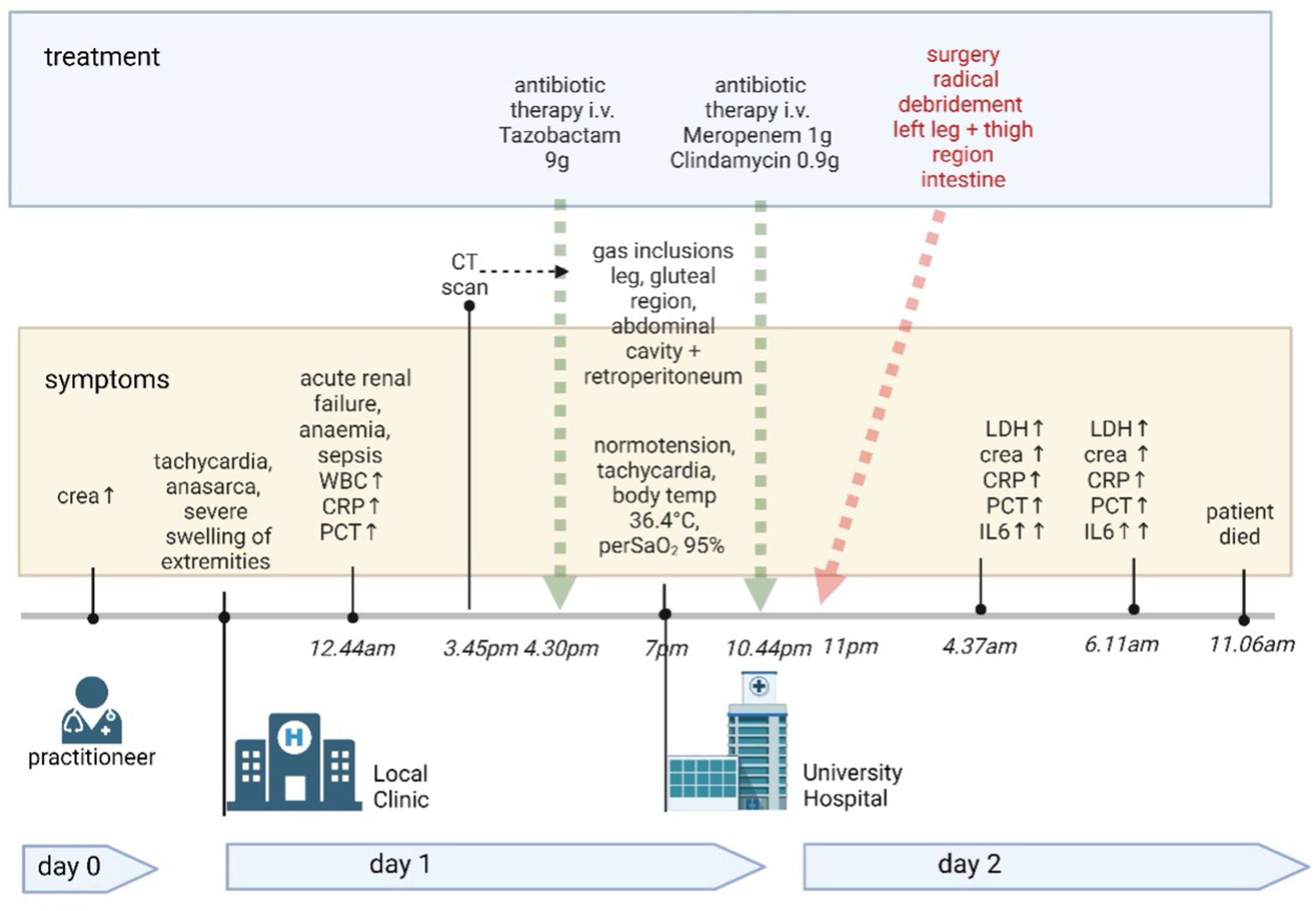
Timeline (created using BioRender.com). CRP, C-reactive protein; WBC, white blood cell count; PCT, procalcitonin; IL6, interleukin-6; LDH, lactate dehydrogenase; Crea, creatinine; perSaO2, peripheral capillary oxygen saturation.
On the morning of day 0, the patient awoke at 4:00
At 7:00
The CT scan performed at 3:54
Following surgery, the patient was transferred to the intensive care unit, where despite receiving maximal treatment, he died at 11:06
Diagnostic assessment
Before the diagnosis of NF, the patient’s vital signs remained stable. He had a Glasgow coma scale score of 15 before sedation for surgery and was fully oriented throughout his wakeful periods.
Initial laboratory results, obtained 4 hours after the first onset of pain, provided limited diagnostic information, although the creatinine level was elevated (2.06 mg/dL) with a nearly normal leukocyte count. Four hours later, a subsequent evaluation at the pre-treating clinic revealed worsening renal function, with a high creatinine level of 2.2 mg/dL accompanied by anemia (hemoglobin: 11.9 g/dL). Inflammatory markers were also elevated: the white blood cell count was 11.45 × 109/L, C-reactive protein (CRP) level was 22.95 mg/dL (229.5 mg/L), and procalcitonin level was 1.81 ng/mL (reference range: 0.0–0.5 ng/mL). The sodium level was slightly below normal at 131 mmol/L.
Further blood tests performed after admission to our department confirmed the presence of sepsis, with a normal white blood cell count (8.4 × 109/L) but significantly elevated CRP (277 mg/L), highly elevated interleukin-6 level at 2500 pg/mL, and an increased procalcitonin level of 3.29 ng/mL.
The LRINEC score is calculated using several factors, including the sodium level (<135 mmol/L = 2 points, ≥135 mmol/L = 0 points), CRP level (≥15 mg/dL = 4 points, <15 mg/dL = 0 points), and white blood cell count (>25 × 109/L = 2 points, 15–20 × 109/L = 1 point, <15 × 109/L = 0 points). Additional relevant parameters include hemoglobin (<11 g/dL = 2 points, 11–13.5 g/dL = 1 point, >13.5 g/dL = 0 points), serum creatinine (>1.59 mg/dL = 2 points, ≤1.59 mg/dL = 0 points), and glucose (>10 mmol/L = 1 point, ≤10 mmol/L = 0 points).4,7,11,17,18 While the LRINEC score is typically used for diagnosis rather than as a progression parameter, we assessed it at various points in this case because of the patient’s presentation across multiple departments (general practice, internal medicine clinic, and our clinic). This serves to highlight the patient’s consistently elevated LRINEC scores, which remained high despite the absence of classic NF symptoms. The scores were as follows: 10 upon initial blood testing, 7 after treatment with sodium and glucose infusions, and 9 the day after (Table 1).
Laboratory results.

1Results obtained by general practitioner. 2Results obtained by Internal Medicine Department, Helios Clinic Niederberg. All other results obtained at Trauma Clinic, BG Klinikum Duisburg.
INR, international normalized ratio; CRP, C-reactive protein; IL-6, interleukin-6; PCT, procalcitonin; LRINEC, Laboratory Risk Indicator for Necrotizing Fasciitis.
Microbiological analysis revealed K. pneumoniae as the sole pathogen present in the initial blood cultures (Table 2). Blood cultures that were taken 12 hours later detected Staphylococcus epidermidis.
Antibiotic resistance profile of Klebsiella pneumoniae isolated from blood cultures and surgical specimens.

s = sensitive, i = intermediate, r = resistant.
A CT scan revealed significant gas entrapment in various regions, including the subcutaneous tissue and muscles of the right thigh, proximal lower thigh on the left side, gluteal region, abdominal cavity, and retroperitoneum.
A major diagnostic challenge was determining the need for a large and radical surgery, particularly because the clinical presentation suggested other, more likely diagnoses. The CT scan, which arrived at our clinic more than 5 hours after it was performed, initially suggested free air in the abdominal cavity and bladder wall. This raised suspicion of a hollow organ perforation, with gas potentially passing through the inguinal canal or obturator foramen to the left leg.
After a thorough review of the clinical data, including new blood test results, reassessment of the LRINEC score, and consultation with radiologists, NF became the most likely diagnosis despite the patient’s relatively good clinical condition.
NF has a high mortality rate, with estimates ranging from 70% to 80% in the literature.3,9,16 Specifically, KP NF is known to carry a higher mortality risk than NF caused by other pathogens. 1
Therapeutic intervention
Once the diagnosis of NF was confirmed, a multidisciplinary team involving the departments of abdominal surgery, radiology, urology, anesthesiology, and intensive care was assembled to provide a highly interdisciplinary approach to the patient’s treatment.
In cases such as this, immediate initiation of guideline-based broad-spectrum intravenous antibiotic therapy is critical after obtaining blood cultures. In addition, prompt and extensive surgical debridement is essential to manage NF effectively. At the pre-treating clinic, the patient had received 9 g of intravenous tazobactam. Upon transfer to our clinic, a calculated broad-spectrum antibiotic regimen was started with meropenem (1 g) and clindamycin (900 mg), adhering to the current gold standard. 5
The multidisciplinary surgical intervention focused on the left leg and thigh. This included radical debridement, wide fasciectomy, and collection of tissue samples. The muscle tissue of the thigh was found to have infectious fascia, largely necrotic subcutaneous tissue, muscle necrosis, and pus. The remaining tissue was significantly swollen. Additionally, the capsule tissue of the left hip joint had disintegrated, exposing the hip prosthesis. Necrotic tissue was also identified in the left gluteal region, extending to the sacral bone.
A paramedian laparotomy was performed simultaneously. This approach was chosen because imaging had indicated that the primary focus of infection was in the left abdomen. The incision provided excellent visibility of the organs on that side and could be extended if necessary. During the procedure, the retroperitoneum was found to contain pus, which had spread to the thigh through the inguinal canal. Further inspection revealed that the rectosigmoid junction was necrotic and perforated. Extensive debridement was performed, along with incisions extending from the lateral thigh to the proximal lower thigh, fasciotomy, and adaptive sutures on the leg.
Surgical removal of the rectum was necessary, and a stoma was created. Because of the complexity of the surgery, primary closure of the abdominal wound was not feasible, and a vacuum-assisted closure system was used for temporary wound management. It became clear during the operation that the patient’s prognosis was poor. If the patient had survived, follow-up microbiological sampling could have been performed after a 4-week course of intravenous antibiotics tailored to the antibiogram, along with the potential placement of local antibiotic chains in a Girdlestone procedure or with a spacer. If no pathogens were detected after the 4 weeks, reimplantation of a hip prosthesis with extended antibiotic therapy could have been considered.
Follow-up and outcomes
The patient’s blood results indicated fulminant sepsis with organ failure. He was transferred to the intensive care unit, where hemodiafiltration was initiated using a hemofilter (CytoSorb; CytoSorbents Europe GmbH, Berlin, Germany) because of progressive renal failure. To manage persistent hypotension, catecholamines and intravascular fluid were administered, with monitoring facilitated by a pulse index continuous cardiac output (PiCCO) system (Pulsion Medical Systems, Muenchen, Germany). The patient’s anemia was treated by transfusion of red blood cell concentrates.
A second assessment by the general surgery department revealed no further evidence of intestinal ischemia. The second survey improved the ventilation parameters because of taking off the vacuum-assisted closure system. A wound dressing with only gauze was applied to the patient’s abdominal aperture.
The administration of high-dose hydrocortisone to manage septic shock was considered. However, evidence regarding its use in septic shock remains inconclusive. In our clinic, we decided against its use, following our standard operating procedures. We considered that the potential adverse effects outweighed the unproven benefits, as noted in the study by Venkatesh et al. 19
Despite the extensive multidisciplinary therapy, the patient’s condition deteriorated rapidly, and he died of fulminant septic shock and multiple organ failure 16 hours later.
Discussion
A limitation of this case report is that we were not involved in treating the patient from the very beginning. As a result, the pre-clinic and primary care physician’s results and findings were only available as written reports. Additionally, the CT scan was not performed in our clinic, so we were unable to obtain the rights to include screenshots in this report. Because of the rapid progression of the case, no photographs were taken during the operation.
A key strength of this case report is the close involvement of most of the authors with the patient. They accompanied him through the emergency room, surgery, and intensive care unit and were involved in every decision and the interpretation of new results. Furthermore, this case provides comprehensive data necessary for a diagnosis of NF, including laboratory results to calculate the LRINEC score, blood culture findings, and intraoperative observations.
NF is a rare disease with an incidence of 0.4 to 1 per 100,000 people, and it carries a mortality rate of up to 80%. 3 It is caused by gas-forming bacteria that rapidly spread along the fascia, leading to a fulminant, necrotizing infection. NF is classified based on microbiology into polymicrobial (type I) and monomicrobial (type II) infections. Type I is the most common, accounting for 80% of cases, and involves a combination of bacteria including streptococci, Enterobacteriaceae, Escherichia coli, Acinetobacter species, Pseudomonas species, Klebsiella species, Proteus species, and Bacteroides species.3–5,8 Monobacterial NF is rarer, representing only 20% of cases, with group A streptococci being the most common pathogens. Since 1996, KP NF, although rare, has been increasingly reported, particularly in Asian countries.1,5 KP NF is associated with high mortality rates, even with appropriate surgical and antimicrobial treatment, because of its rapid progression, tendency to invade, and hematogenous spread, which often results in severe sepsis. 20
To contextualize this case within the broader research landscape, we compared it with the first five case reports or reviews found on PubMed using the search terms “necrotizing fasciitis” and “case report.” We concluded that NF is highly variable, with little consistency across cases, underscoring its reputation as a “chameleon” with symptoms that make early diagnosis challenging. The most thorough review by Rahim et al., 1 performed in 2019, included 71 cases of KP NF and identified diabetes and an immunocompromised state as predisposing factors; however, they are not always the main symptoms.
The five most recent NF cases involved three male and two female patients aged between 2 and 73 years.13,21–24 In cases of KP NF, there is a slight male predominance. 1 The reported presentations of NF vary, ranging from an unconscious patient with toxic shock who could have been saved by hyperbaric oxygen therapy, antibiotics, and mastectomy, to a patient with NF in the left arm treated for cellulitis for 2 months with multiple debridements and an eventual fatal outcome.20,25 NF may be localized in various regions, including the right breast, hand, perineum, and chest/axillary region.21–24 One patient, similar to ours, presented with NF in the lower extremity. 23 A review of KP NF also noted a higher incidence in the lower limb. 1 None of the cases involved NF in the abdomen. The clinical courses ranged from subacute (2 months) to acute (1 day, as in our case).13,21–24 Three cases were polymicrobial, and one was monomicrobial, caused by Serratia marcescens. Only one polymicrobial case involved K. pneumoniae, similar to ours. 21
KP NF is significantly more common in Asia than in Europe, although cases are slowly increasing. The entry points for infection in the reviewed cases included an insect bite, vascular malformations treated with surgery and sclerotherapy, trauma, and diabetes.13,22,24 In two cases, CT scans did not show radiological signs of NF13,23; by contrast, CT imaging was key in our case. The other three cases did not mention imaging. All patients received antibiotics, but the combinations varied. The gold standard treatment includes meropenem and clindamycin, which we administered in our case. 5 Only one case used meropenem, two used clindamycin, but none used both in combination.13,21–24 Three patients survived with good cosmetic outcomes following debridement, one was saved by amputation, and one patient died. One received hyperbaric oxygen therapy.13,21–24 KP NF has been shown to have a higher mortality rate than NF in general. 1
Overall, these five cases and our case differ in terms of localization, bacteria, outcomes, risk factors, blood markers, age, sex, and symptoms. This highlights the highly variable presentation of NF, emphasizing the importance of raising awareness for NF as a differential diagnosis in patients with unusual clinical presentations.13,21–24 The increasing prevalence of KP NF, although still rare, suggests that it should be considered within the bacterial spectrum of potential pathogens, especially in immunocompromised patients. 1
Diagnosis of NF is frequently delayed, but it requires immediate action once suspected. While there are many diagnostic indicators, there is no universally established diagnostic guideline or pathway. The AWMF guidelines recommend surgical exploration when NF is suspected. This suspicion may arise from clinical signs, specific blood markers, or radiological findings, particularly from CT scans. 5 However, the definitive diagnosis of NF can only be confirmed through surgical exploration. 12
Inadequate pain resulting from ischemia is a leading clinical sign of NF.5,8,10 Other less specific signs include systemic shock, skin necrosis, hemorrhagic bullae, and soft tissue emphysema.8,10 The literature classifies NF as a clinical diagnosis.5,8,10 Risk factors, such as recent surgery, minor wounds, vascular diseases, or low immune status, are also unspecific but can provide clues.8,10
None of these signs were present in our patient, except for swelling, which Wong and Wang 16 identified as a potential feature. Inadequate pain could have been masked by the patient’s analgesic medication.8,10 Our patient had no recent surgery or wounds. The infection may have entered through the urinary system or resulted from a complication of the patient’s Crohn’s disease, such as colonic perforation. Steroid therapy has been identified as a risk factor for colonic perforation in Crohn’s disease. 26 Symptoms of classical peritonitis could have been masked by the patient’s use of painkillers and high-dose prednisolone therapy. Reuken et al. 27 demonstrated that gram-negative infections in colonic perforations associated with Crohn’s disease were more common in patients receiving steroid therapy than in patients without immunosuppression or those on nonsteroidal immunosuppressive therapy.
The first body site typically affected by NF is the superficial fascial layer of the skin. As the infection progresses, it involves deeper layers, such as the deep dermis and fascia. 16 In our case, the skin and subcutaneous tissues were almost completely preserved, which is highly unusual. Instead, the abdominal cavity and muscle were severely affected, which may have contributed to the absence of typical clinical signs.
Radiological imaging is a valuable tool in diagnosing NF. The gold standard is MRI, which has a sensitivity of 93%. However, CT scans have been shown to have a sensitivity of at least 80%, as demonstrated by Tso and Singh, 9 with the only pathognomonic sign being dissecting gas along the fascia in the absence of penetrating trauma. Although CT is mentioned in guidelines, it is not given high significance. 5 This case may support incorporating MRI into future guidelines.
Despite advances in imaging, laboratory tests for NF remain unreliable, and blood results in our case were highly nonspecific. 6 Murphy et al. 21 found that elevated white blood cell counts (>15,400 × 109/L) and serum sodium levels of >135 mEq/L were associated with NF, with a sensitivity of 90% but a specificity of 76%.5,21 In our patient, the first blood test results showed hyponatremia. The hypernatremia observed in the second blood sample can be explained by the intravenous administration of sodium. Additionally, none of the blood tests prior to diagnosis showed leukocyte counts above 11,500 × 109/L.
The LRINEC score is frequently recommended as a predictive tool for NF.7,9,18,28 A score of ≥6 has a positive predictive value of 92% and a negative predictive value of 96%. A score of ≥8 has a positive predictive value of 93.4%, indicating a strong likelihood of NF. 16 In our case, the initial LRINEC score was 10 and decreased following treatment. The LRINEC score is most helpful when there is already a suspicion of NF because the blood markers used are highly nonspecific. Unfortunately, the test is not widely known or utilized.
NF is a rare diagnosis with high mortality rates and often presents with nonspecific clinical symptoms.3,5,11,12,16 However, early diagnosis and prompt treatment with broad-spectrum antibiotics and surgery significantly improve outcomes. 5
Current guidelines emphasize the poor clinical condition of the patient and the presence of disproportionate pain as key early symptoms of NF. Additionally, sodium concentrations higher than 135 mmol/L and elevated leukocyte counts (>15,400 × 109/L) have been included as diagnostic criteria, along with gas on CT without evidence of perforation as a “characteristic sign.” 5
To follow the guideline’s recommendation for early surgical exploration when NF is suspected, physicians should be familiar with the most important diagnostic tools for NF, as indicated by this case and supported by thorough research:
NF is a “chameleon” in terms of clinical presentation, vital signs, blood results, and radiological findings. If any of these aspects raise suspicion of NF, physicians should be aware that it is common for NF to present in an atypical manner.12–14,16,20,23 NF is challenging to diagnose clinically, and while inadequate pain out of proportion is often an early symptom, it is not mandatory for diagnosis. The clinical stages outlined by Wong and Wang
16
may be helpful in the diagnostic process. The LRINEC score is a valuable and reliable tool in diagnosing NF.7,18,28 Entrapped air visible on a CT scan is pathognomonic, though not common. It can appear in atypical locations, such as the abdominal cavity, and may spare the skin and subcutaneous tissues, as in our case.
The primary conclusion is that diagnosing NF requires a combination of targeted patient history, a thorough clinical examination, interpretation of laboratory results, calculation of the LRINEC score, and careful evaluation of radiological imaging.
It is also crucial to consider potential sources of bacterial infection, such as minor injuries, a compromised immune system, or recent surgical procedures. NF symptoms may include tenderness, erythema, and warmth of the skin, although more distinct signs—such as crepitus, skin fluctuation, bullae, or disproportionate pain—may not always be present. Laboratory findings, particularly leukocyte counts of >15,400 × 109/L and serum sodium levels of >135 mEq/L, should be carefully considered because they are associated with 90% sensitivity for NF. When NF is suspected, the LRINEC score should be evaluated. Radiological imaging, such as CT or MRI, is recommended to identify the pathognomonic sign of dissecting gas along the fascia, particularly in the absence of penetrating trauma.
Despite all this diagnostic information, the most important point to remember is that NF often presents in atypical ways, making it a difficult but critical diagnosis to consider.
Footnotes
Acknowledgements
We thank Dr. med. N. Brinkmann from BG Klinikum Duisburg, University Duisburg-Essen, for his support with this article. As Head of the Department of Trauma Surgery at the treating hospital, he was involved in key therapeutic decisions in the operating room and the intensive care unit. Additionally, we would like to thank Dr. S. Yaman for his assistance with data management.
Author contributions
DKB and MR conceptualized and designed the study. DKB, MR, JW, SE, MD, and MH collected and analyzed the data. DKB, MR, and MH interpreted the data and drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Data availability statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request. Part of the dataset was collected by BG Klinikum Duisburg, University Duisburg-Essen, where we were the final hospital to provide treatment. Another dataset, including laboratory results, CT scans, and clinical examinations, was provided by the internal medicine department of Helios Clinic Niederberg, Germany. The initial examination and blood results were collected by Dr. S. Yaman, a general practitioner in Velbert, Germany.
Declaration of conflict interest
All authors confirm that there is no financial conflict of interest to acknowledge in this article. Any commercial or financial arrangements related to the article have been disclosed to the Editor, who has confirmed that there are no conflicts of interest to declare. Furthermore, we have not entered into any agreements with sponsors that could compromise the impartiality of our data reporting.
Ethics statement
According to established guidelines, this study did not require ethical approval because of its retrospective nature and focus on a single case report. All patient-related data have been thoroughly anonymized to maintain strict confidentiality.
Funding
This work was supported by the Open Access Publication Fund of the University of Duisburg-Essen, Germany.
Informed consent
The patient’s wife provided written informed consent for publication of this case report.