
Abstract
Objective
We compared the application value of noninvasive positive pressure ventilation (NIPPV) and intermittent positive pressure ventilation (IPPV) in the treatment of very premature infants and extremely low birth weight infants.
Methods
Multivariate logistic regression analysis was used to identify factors influencing the transition from noninvasive to invasive ventilation in this infant cohort.
Results
Among extremely preterm infants, 83.3% with gestational age <25 weeks transitioned from noninvasive to invasive ventilation, as did 80.6% of those with birth weight <1000 grams. Multivariate analysis indicated that gestational age <25 weeks, birth weight <1000 grams, and Apgar score ≤7 were significant factors affecting the likelihood of transitioning to invasive ventilation. The survival rate at discharge was 94% for the NIPPV group compared with 89% for the IPPV group. The NIPPV group demonstrated significantly lower rates of complications, shorter weaning times, and reduced lengths of hospital stay compared with the IPPV group.
Conclusions
Both NIPPV and IPPV effectively improved oxygenation and ventilation in extremely preterm infants. However, NIPPV showed significant advantages in reducing complications, shortening weaning time, and decreasing the hospital stay duration. Prioritizing the use of NIPPV may enhance treatment outcomes and survival quality, providing evidence-based support for clinical practice.
Keywords
Introduction
In the realm of neonatal intensive care, the management of extremely preterm infants (EPT) and extremely low birth weight infants (ELBW) presents considerable clinical challenges. 1 Owing to the immaturity of organ systems, particularly the lungs, these neonates frequently depend on mechanical ventilation to support fundamental respiratory functions. Historically, intermittent positive pressure ventilation (IPPV) has been the primary method for assisting this vulnerable population. However, the application of IPPV is closely linked to a range of complications, including ventilator-associated pneumonia (VAP) and bronchopulmonary dysplasia (BPD), which may manifest within the first 3 months, alongside risks such as tracheobronchial injury. 2
Advancements in medical technology have led to the emergence of noninvasive respiratory support methods, as critical components of neonatal respiratory management. Noninvasive positive pressure ventilation (NIPPV) represents a novel approach that reduces the complications associated with invasive ventilation by delivering intermittent positive pressure while allowing for spontaneous respiratory efforts in the infant. This technique effectively enhances gas exchange, positioning it as a viable alternative strategy.3,4
In recent decades, extensive research has been conducted on the implementation of NIPPV in neonates, particularly EPT and ELBW infants. Evidence suggests that NIPPV may decrease the need for invasive ventilation, lower ventilator-related complications, shorten hospital stays, and potentially enhance survival rates, in comparison with IPPV.5,6 Nonetheless, the comparative efficacy and safety of NIPPV versus IPPV in this population remain subjects of debate, likely attributable to disparities in study design, sample sizes, and intervention methods. 7
In this retrospective study, we aimed to systematically compare the effects of NIPPV and IPPV in EPT and ELBW infants, with a specific emphasis on key clinical indicators such as weaning duration, rates of conversion from noninvasive to invasive ventilation, the incidence of short-term complications, and survival at discharge. These metrics are not only critical to the immediate prognosis of these newborns but also have profound implications for their long-term health and development. 8 Through this investigation, we aspire to provide clearer guidance for the respiratory management of EPT and ELBW infants, offering a scientific foundation for clinicians to select the most appropriate respiratory support strategies. Ultimately, this may enhance clinical outcomes for this particularly vulnerable cohort. Furthermore, the findings may serve as evidence to inform updates to clinical guidelines and the formulation of health policies.
Methods
Study design and participants
This retrospective observational study was conducted among infants who were very premature and classified as very low birth weight, admitted to the neonatal intensive care unit (NICU) at our hospital between May 2022 and May 2023. To protect patient confidentiality, all identifying information was completely removed from the data.
Infants were eligible for inclusion if they were diagnosed as preterm, with a gestational age ranging from 22 to 28 weeks and a birth weight below 1500 grams. The first method of respiratory support provided upon NICU admission was either NIPPV or IPPV. Written informed consent was obtained from the guardians of all participants.
Infants were excluded if their guardians opted to discontinue treatment within the first 24 hours post-birth. Additional exclusion criteria included congenital heart defects, severe asphyxia, congenital respiratory anomalies, serious complications such as bleeding or infections that could compromise treatment efficacy, respiratory distress owing to meconium aspiration syndrome or wet lung, and infants unable to breathe independently. Infants with incomplete medical records or those who could not be adequately followed were also excluded.
Participants were categorized into two groups based on the type of ventilation received: the NIPPV group and the IPPV group.
This study received ethical approval from the Ethics Committee of the Fourth Hospital of Shijiazhuang (4/27/2022, approval number: EC2022-0501) and complies with the ethical standards outlined in the Declaration of Helsinki. Written informed consent was obtained from all parents or legal guardians of the infants involved in the study. The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 9
Methods
For both groups of premature infants, bedside electrocardiogram monitors were used to rigorously track vital signs, including respiratory rate, heart rate, and blood oxygen saturation. Additionally, protocols were established to ensure airway patency, maintain thermal stability, and create an optimal internal environment for the infants while also facilitating tube feeding and other necessary interventions.
Noninvasive positive pressure ventilation (NIPPV) group
Infants in the NIPPV group were treated with NIPPV using a continuous positive airway pressure ventilator (Fritz Stephan GmbH, Gackenbach, Germany). The ventilator was calibrated with the following parameters: the fraction of inspired oxygen (FiO2) was set between 25% and 40%, and positive end-expiratory pressure (PEEP) was adjusted to a range of 4 to 10 cm H2O.
Intermittent positive pressure ventilation (IPPV) group
Infants in the IPPV group received invasive mechanical ventilation. Oral intubation was performed, adhering to stringent aseptic techniques and completed within 20 s. Ventilation was administered using the SLE5000 ventilator (Sector-135, Noida, India). During the ventilation period, comprehensive respiratory management was implemented, which included the removal of respiratory secretions and regular replacement of the endotracheal tube. The initial ventilator settings were as follows: FiO2 above 25%, peak inspiratory pressure set between 15 and 20 cm H2O, PEEP between 4 and 6 cm H2O, tidal volume of 6 to 8 mL/kg, and a respiratory rate of 30 to 50 breaths per minute. Extubation was considered when the infant’s condition stabilized, as indicated by favorable blood gas parameters, typically occurring after an average of 5 to 7 days, followed by a transition to noninvasive ventilation.
For the NIPPV group, the ventilation withdrawal criteria included a mean airway pressure (MAP) of less than 6 cm H2O and FiO2 below 30%. For the IPPV group, the criteria comprised MAP <6 cm H2O, FiO2 <30%, and a respiratory rate of less than 30 breaths per minute. Successful extubation was defined as adequate spontaneous breathing, improved chest X-ray findings, oxygen saturation >0.90, and normalized blood gas metrics.
Outcomes
The primary endpoints were 1) changes in arterial partial pressure of carbon dioxide (PaCO2), arterial partial pressure of oxygen (PaO2), oxygenation index (OI), and the ratio of PaO2 to FiO2 (PaO2/FiO2) in both groups post-ventilation, to discern intergroup variations; and 2) the incidence of complications, including VAP, BPD, and pneumothorax.
Secondary endpoints were the survival rate at discharge, alongside relevant treatment metrics such as ventilator weaning time and length of hospital stay. Additionally, the proportion of infants in the NIPPV group necessitating conversion to invasive ventilation for life-sustaining treatment was calculated, along with evaluation of potential contributing factors.
Data analysis
Descriptive statistics were used to analyze baseline characteristics, with continuous variables expressed as mean ± standard deviation and categorical variables reported as frequency and percentage. Weaning times were compared using independent samples t-tests, and complication and survival rates were analyzed with chi-square tests. A multivariate logistic regression analysis was conducted to identify independent factors affecting the transition from noninvasive to invasive ventilation, considering variables such as gestational age, birth weight, Apgar score, and maternal complications during pregnancy. Statistically significant variables (P < 0.05) were included in the regression model to derive adjusted odds ratios (OR) and 95% confidence intervals (CI) for the influence of each factor. All statistical analyses were executed using IBM SPSS version 26.0 (IBM Corp., Armonk, NY, USA), with P < 0.05 considered statistically significant.
Results
Comparison of baseline characteristics between NIPPV and IPPV groups
Baseline characteristics of 200 neonates in the NIPPV and IPPV groups (100 newborns in each group) were compared, as shown in Table 1. The sex ratio was 0.92:1. Baseline characteristics were comparable across both groups, with no significant differences noted. Gestational age and birth weight were not significantly different between the two groups; the mean gestational age was approximately 26 weeks and the mean weight was approximately 1200 grams. The Apgar score (5 minutes) was also similar between the two groups, with a mean of 7.4. In terms of maternal complications during pregnancy, the proportions in the two groups were similar, with approximately 30% of mothers having complications during pregnancy.
Comparison of baseline characteristics between the two groups.
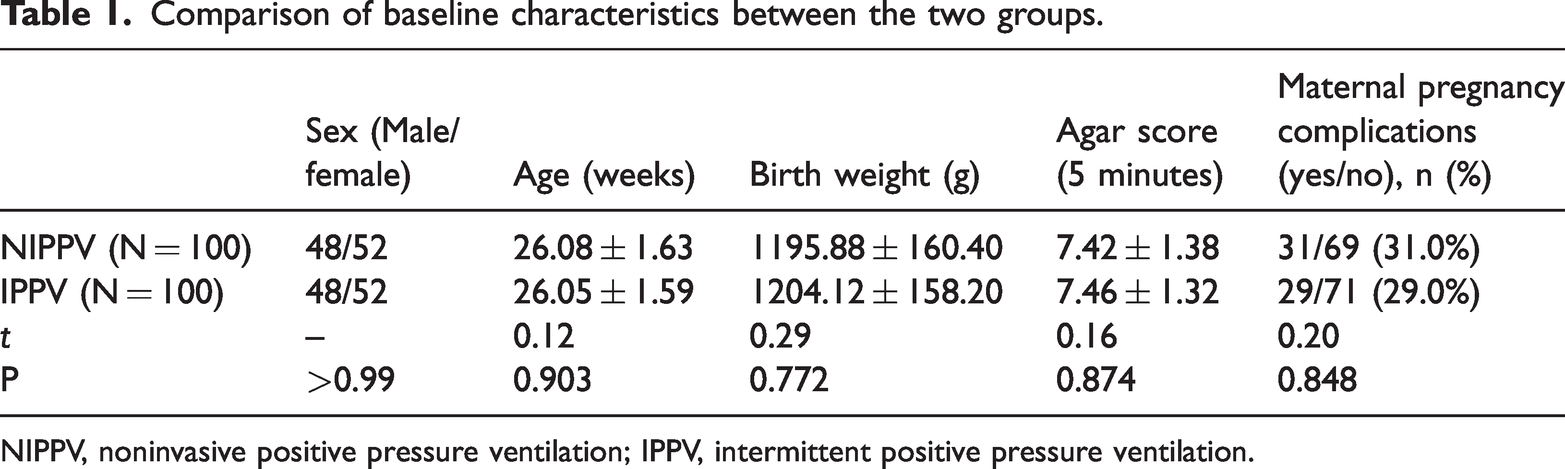
NIPPV, noninvasive positive pressure ventilation; IPPV, intermittent positive pressure ventilation.
Comparison of related treatment conditions between groups
The weaning times and hospital stays in the NIPPV group were significantly shorter than those in the IPPV group, as shown in Table 2 (P = 0.001).
Comparison of weaning time between the two groups.

NIPPV, noninvasive positive pressure ventilation; IPPV, intermittent positive pressure ventilation.
Comparison of blood gas analysis indicators between groups
There was no statistically significant difference in PaCO2, PaO2, the OI, respiratory index (RI), and PaO2/FiO2 between the two groups of newborns before mechanical ventilation treatment. After mechanical ventilation treatment, PaCO2, OI, and RI were decreased and PaO2 and PaO2/FiO2 were increased; compared with before treatment, there were statistically significant improvements in both groups (P < 0.05). After treatment, there was no significant difference in the levels of PaCO2, PaO2, OI, RI, and PaO2/FiO2 between the two infant groups, as shown in Table 3.
Comparison of blood gas analysis indicators between the two groups.

NIPPV, noninvasive positive pressure ventilation; IPPV, intermittent positive pressure ventilation; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; FiO2, fraction of inspired oxygen; OI, oxygenation index; RI, respiratory index.
Incidence of noninvasive to invasive ventilation and multivariate logistic regression analysis
The incidence of conversion from NIPPV to IPPV in the NIPPV group is shown in Table 4. In newborns with gestational age less than 25 weeks, 83.3% transitioned to invasive ventilation, compared with 20% in newborns with gestational age 25 to 28 weeks. Among newborns with birth weight less than 1000 grams, 80.6% required invasive ventilation. Multivariate logistic regression analysis showed that gestational age <25 weeks (p < 0.001), birth weight <1000 grams (p < 0.001), and Apgar score ≤7 (p = 0.028) were significant factors influencing the likelihood of transitioning from noninvasive to invasive ventilation. Additionally, infants whose mothers had pregnancy complications also had a higher risk of conversion to invasive ventilation, but this was not significant.
Incidence of noninvasive to invasive ventilation in multivariate logistic regression analysis.

CI, confidence interval.
Comparison of short-term complication rates between groups
The short-term risk of complications between the two modes of ventilation is shown in Table 5. In the NIPPV group, the incidence of BPD was 20%, that of pneumothorax was 13%, and that of VAP 15%. In comparison, the incidence of these complications was 32%, 20%, and 25%, respectively, in the IPPV group.
Comparison of short-term complication rates between the two groups.
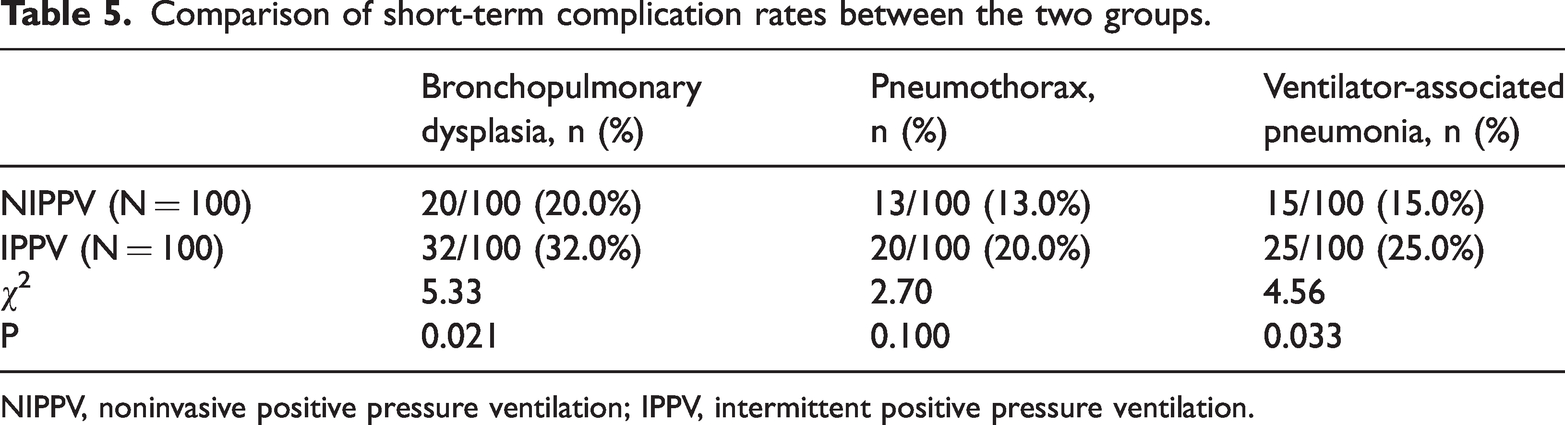
NIPPV, noninvasive positive pressure ventilation; IPPV, intermittent positive pressure ventilation.
Comparison of survival rates between groups
The discharge survival rates for infants in the two groups is shown in Table 6. The discharge survival rate was 94% in the NIPPV group and 89% in the IPPV group. Although survival was slightly higher in the NIPPV group, the difference was not statistically significant.
Comparison of survival rates between the two groups.

NIPPV, noninvasive positive pressure ventilation; IPPV, intermittent positive pressure ventilation.
Discussion
Traditionally, IPPV is used primarily when a patient’s condition declines substantially, particularly when arterial blood gas analyses reveal critical abnormalities. However, the use of IPPV is not without its drawbacks as it carries the risk of complications associated with tracheal intubation. 10 Conversely, NIPPV is broadly applicable and is generally more acceptable to both patients and their families owing to its non-invasive nature. 11 In recent years, the clinical success rates of NIPPV have increased notably, particularly in treating acute exacerbations of chronic obstructive pulmonary disease. Additionally, NIPPV’s effectiveness has been affirmed in managing severe pneumonia, acute asthma, acute respiratory distress syndrome, and acute respiratory failure attributed to cardiogenic pulmonary edema.12,13
A study by Wang et al. 14 highlights that NIPPV can significantly improve respiratory rates and heart rates, with approximately 80% of patients exhibiting substantial improvements in arterial blood gas parameters following treatment and approximately 65% avoiding the need for intubation. In the present research, we investigated the comparative effects of NIPPV and IPPV in the treatment of ELBW infants. The findings revealed that both ventilation strategies led to significant enhancements in PaCO2 as well as the OI and RI, alongside notable increases in both PaO2 and the PaO2/FiO2 ratio. Although no significant differences were observed between the two modalities regarding these parameters, the NIPPV group demonstrated a considerably lower incidence of ventilator-associated complications compared with the IPPV group, alongside shorter weaning times and reduced hospital stays.
NIPPV maintains continuous positive pressure via a facial or nasal mask, effectively keeping the airway unobstructed, minimizing alveolar collapse, and reducing the risk of airway injury. Although IPPV also improves oxygenation and ventilation, it may inadvertently elevate the risk of mechanical ventilation-related complications.15–17 This aligns with the findings of Yin et al., 18 which suggest that NIPPV is more effective than IPPV in mitigating the risk of bronchopulmonary dysplasia. Furthermore, that study indicated that a shorter transition period from invasive to non-invasive ventilation correlates with improved weaning success rates. This observation is consistent with the work of Kundu et al., 19 who emphasized that early initiation of non-invasive ventilation enhances the likelihood of successful weaning. EPT infants, particularly those with gestational age under 25 weeks, are more likely to require conversion from NIPPV to invasive ventilation, likely owing to their immature pulmonary function. Yuan et al. 20 supported this perspective, noting that infants with very low gestational age respond less favorably to NIPPV compared with their more mature peers. These findings resonate with a systematic review and meta-analysis, 21 which asserted that non-invasive ventilation techniques, such as NIPPV, can significantly reduce complications associated with mechanical ventilation and improve weaning success rates.
This study has several limitations that should be considered. As a retrospective observational design, biases related to patient selection and data collection may have been introduced, limiting causal inferences. Although the sample size of 200 infants provides some insights, it may be insufficient to detect subtle differences between the NIPPV and IPPV groups, thereby affecting the statistical power of the findings. Additionally, the results are derived from a single institution, which may restrict their generalizability to other settings. Variability in clinical practice and potential inconsistencies in data recording could further impact the accuracy of the results. Although efforts were made to control confounding factors, unmeasured variables may still influence the outcomes. Moreover, this study primarily assessed short-term outcomes, such as weaning times and survival rates at discharge, without evaluating long-term effects on neurodevelopment and quality of life. Lastly, subjectivity in assessing complications may lead to variability in data interpretation. These limitations highlight the need for caution in interpreting the results and underscore the importance of further research to validate these findings in larger, multicenter studies with prospective designs.
Conclusion
This study indicated that both NIPPV and IPPV can effectively improve the oxygenation and ventilation indicators of EPT and ELBW infants. However, NIPPV showed significant advantages in reducing ventilator-related complications as well as shortening weaning times and hospital stays, making NIPPV particularly suitable for non-invasive supportive treatment. Additionally, we found that EPT infants with a younger gestational age may have a weaker response to NIPPV and are more likely to require a transition to invasive ventilation. These findings suggest that in the support of EPT infants, giving priority to NIPPV may help improve the treatment effect and survival quality and further reduce the mechanical ventilation rate in very premature infants. Future studies should continue to explore the application of NIPPV in preterm infants of different gestational ages and weights to optimize its clinical effect.
Footnotes
Authors’ contributions
Huifen Chen and Ming Zhang designed the research study. Xingyu Bai and Shuang Zheng performed the research. Dawei Wei, Mengbin Zhang, and Yanxia Qiao conducted the experiments and analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by Hebei Province Medical Science Research Project (No. 20231680).