
Abstract
Objective
This study was performed to determine the dimensions of the sella turcica (ST) in relation to sex, age groups, and sphenoid sinus (SS) pneumatization patterns in a cohort of Iraqi individuals.
Methods
This cross-sectional study analyzed computed tomography images of 99 individuals (53 men, 46 women) aged 24 to 59 years to measure ST dimensions, including length, width, height, depth, and surface area. SS pneumatization was classified by sex and age. We also examined the relationship between ST size and SS pneumatization patterns.
Results
Women exhibited a significantly greater mean ST depth (9.37 mm) than men (8.19 mm). The ST diameter was significantly larger in the middle-aged group (13.1 mm) than in the young adult group (11.83 mm). The ST area showed a highly significant difference between sexes. The sellar pneumatization pattern was the most common, whereas the conchal pattern had the lowest prevalence. A significant correlation was observed between ST size and SS pneumatization.
Conclusion
The ST depth and diameter showed statistically significant differences across sex and age groups, respectively. The variability in SS pneumatization patterns underscores the importance of considering pneumatization types during surgical planning to minimize the risk of iatrogenic injury and improve treatment outcomes.
Introduction
The sella turcica (ST) is a saddle-shaped depression located in the middle of the sphenoid bone. Its developmental and morphological patterns are diverse and well-documented. 1 The anterior boundary of the ST is the tuberculum sellae, while the posterior boundary is the dorsum sellae. It projects four clinoid processes, two anteriorly and two posteriorly. The ST, situated in the middle cranial fossa on the intracranial surface of the sphenoid sinus (SS) bone, houses the pituitary gland.2,3 Previous studies have revealed significant anatomical variations in the size and shape of the ST across different ethnicities and age groups.4,5
The sphenoid bone is an unpaired, complex bone located at the base of the anterior and middle cranial fossae. It features two pairs of wings (lesser and greater) and two pterygoid processes that extend inferolaterally. The SS, varying in size and shape, develops secondary to aeration of the bone body. Enlargement of the SS occurs as a result of bone wall resorption and thinning with age. 6 The pneumatization patterns of the SS vary geographically, racially, and ethnically. 7
Computed tomography (CT) is the preferred imaging technique for assessing the structural and volumetric characteristics of the SS. 8 Although CT is considered the gold standard for three-dimensional evaluation of the paranasal sinuses, cone-beam CT offers improved image resolution, reduced scan times, lower radiation doses, and lower costs. 9 Despite the extensive knowledge of ST and SS anatomy, the relationship between ST dimensions and SS pneumatization types has been insufficiently explored. This study aims to address this gap by investigating the association between the ST and SS pneumatization types.
A comprehensive understanding of the SS and surrounding critical structures is crucial for reducing complications during functional endoscopic sinus surgery and transsphenoidal surgery, particularly concerning the intersinus septum and carotid artery pathway. This study was performed to determine the dimensions of the ST based on sex and age groups and its relationship with SS pneumatization patterns in a sample of Iraqi individuals.
Materials and methods
Research design
In this prospective cross-sectional observational study, we examined the size of the ST using CT images. We measured and compared the dimensions of the ST, including its length, width, diameter, depth, and surface area, in millimeters across sex and age groups. We followed an established methodology described in the literature that determined the classification and distribution of SS pneumatization among different sex and age groups.10,11 Additionally, we assessed the relationship between ST size and SS pneumatization. The reporting of this study conforms to the STROBE guidelines. 12
Data collection
The study involved Iraqi patients who visited the Radiology Department of Al-Karama Hospital for reasons unrelated to craniofacial pathology and underwent CT scans. In total, 99 individuals (53 men and 46 women) aged 24 to 59 years were included. The study was approved by the Ethics Committee of Al-Mustansiriyah University, College of Dentistry (MUOMED01) and adhered to the standards of the Declaration of Helsinki. Written informed consent was obtained from all participants, and all data were de-identified to maintain confidentiality.
Sample size calculation
Based on data from the pilot study and calculations using the G*Power 3.1.9.7 program, the minimum required sample size for each group was determined to be 43 patients.
Participants
Inclusion criteria
Participants were clinically healthy and free from abnormalities affecting the craniofacial or maxillofacial region, such as cleft lip, palate, or bone disorders. Only images in which the SS was completely visible were included. Eligible participants were aged 24 to 59 years.
Exclusion criteria
Patients with medical histories of deformities, craniofacial or maxillofacial surgeries, SS surgery, orthognathic surgery, craniofacial trauma, or those with inadequate CT scan resolution were excluded. Because ST dimensions are thought to vary until skeletal maturation, the study included only patients older than 18 years. 4
CT settings
Images were acquired using the SOMATOM Sensation 16 CT Scanner (Siemens Healthineers, Erlangen, Germany) at settings of 39 mA, 100 kVp, and a slice thickness of 1.0 mm, displayed on an 18-inch color LCD monitor (Siemens). The RadiAnt DICOM viewer software (Medixant, Poznan, Poland), recognized for its reliability in previous studies, was used to display the images. 13
Measurements
The following parameters of the ST and SS were assessed using sagittal sections of CT images, with measurements obtained for each patient (Figures 1 and 2).
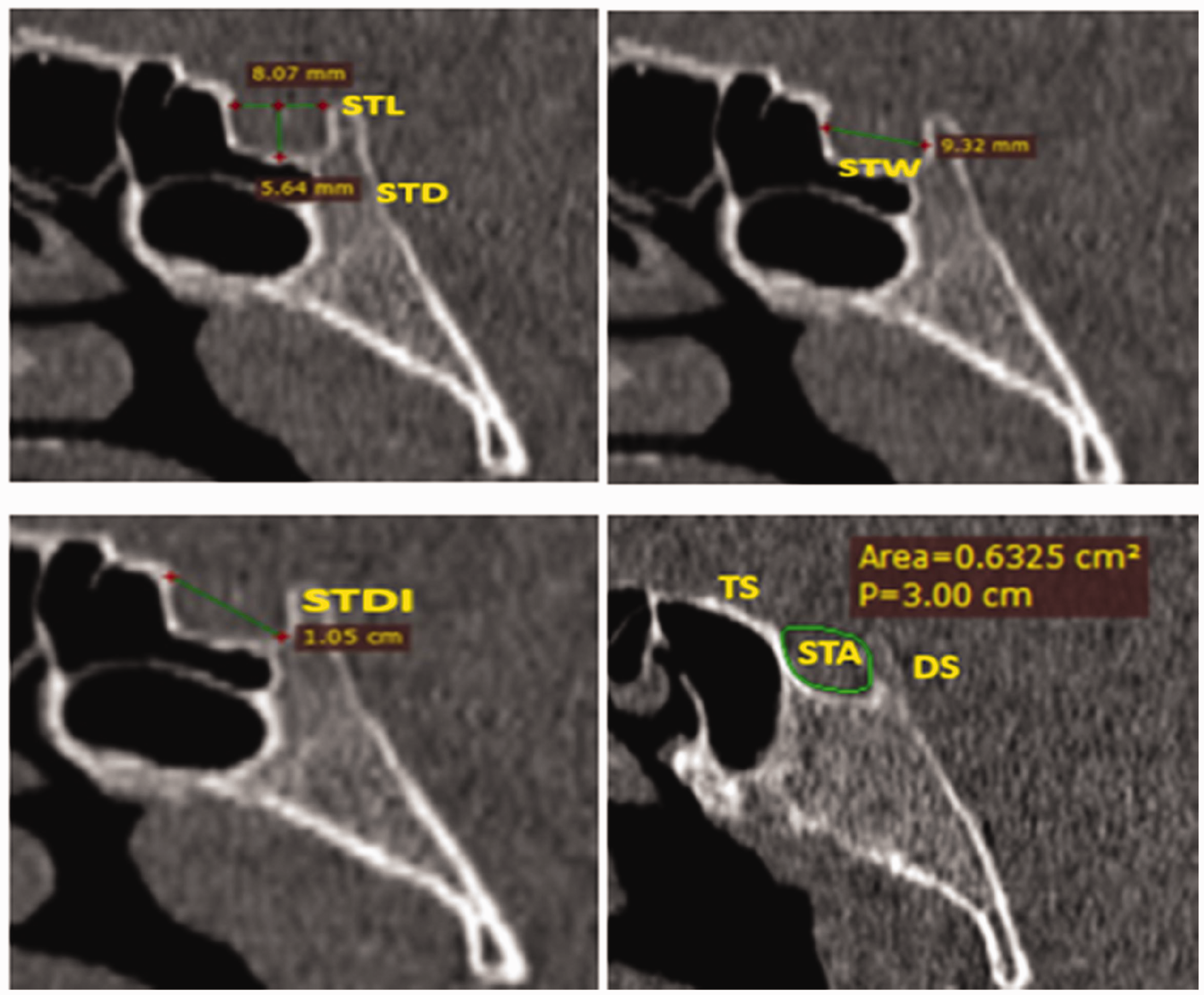
ST measurements (STL, STD, STW, STDI, and STA). ST, sella turcica; STL, sella turcica length; STD, sella turcica depth; STW, sella turcica width; STDI, sella turcica diameter; STA, sella turcica area; TS, tuberculum sellae; DS, dorsum sellae.

Pneumatization patterns of the sphenoid sinus (sellar, presellar, conchal, and postsellar).

Sex distribution in the study.
ST length (STL): The distance between the dorsum sellae and the tuberculum sellae.
ST depth (STD): The vertical distance from the STL line to the deepest point of the hypophyseal fossa.
ST width (STW): Measured parallel to the Frankfurt horizontal line, representing the greatest anteroposterior dimension between the anterior and posterior boundaries of the ST.
ST diameter (STDI): The distance from the tuberculum sellae to the most posterior point within the hypophyseal fossa.
ST area (STA): The STA was measured as depicted in Figure 1. The measurement was conducted using the RadiAnt DICOM viewer software tools.
SS pneumatization patterns: SS pneumatization was categorized into four distinct patterns: sellar, presellar, postsellar, and conchal. 14
Statistical analysis
One week later, the same radiologist repeated the estimation process. A paired t-test conducted on 10 random CT scans showed no significant differences (p < 0.05) between the two readings, confirming intraobserver reliability as shown by the nearly identical results. Data analysis was performed using the Statistical Package for Social Scientists (IBM SPSS version 22; IBM Corp., Armonk, NY, USA). The normality and homogeneity of variance were assessed using the Shapiro–Wilk test and Levene’s test, respectively. Student’s t-test was used to compare the average differences in ST dimensions between sex and age groups. The study also evaluated the correlation between ST size and SS pneumatization patterns. Odds ratios (ORs) with 95% confidence intervals were calculated. A p-value of <0.05 was considered statistically significant.
Results
In total, 99 individuals were enrolled in the study. The participants comprised 53 (53.54%) men and 46 (46.46%) women, as shown in Chart 1. Table 1 shows the distribution of ST measurements. Women had a significantly greater mean STD (9.37 mm) than men (8.19 mm) (p = 0.002). The STA also showed a highly significant difference between the two sexes (p < 0.0001). The participants were categorized into two age groups: young adults (24–39 years) and middle-aged adults (40–59 years). Of the 46 women and 53 men, 50 were in the young adult group (35 women, 15 men) and 49 were in the middle-aged group (11 women, 38 men). The STDI was significantly larger in the middle-aged group (13.1 mm) than in the young adults (11.83 mm) (p = 0.018) (Table 2). Women were more likely than men to have a larger STD (OR, 2.498; p = 0.003). There was a statistically significant association between age groups and ST measurements, with the middle-aged group showing a larger STDI and STA (OR, 1.593; p = 0.005 and OR, 1.072; p < 0.0001, respectively) (Table 3).
Descriptive statistics of ST measurements.

SE, standard error; SD, standard deviation; ST, sella turcica; STL, sella turcica length; STD, sella turcica depth; STDI, sella turcica diameter; STW, sella turcica width; STA, sella turcica area.
Distribution of ST measurements by age groups and sex.

*Significant; **Highly significant.
SD, standard deviation; ST, sella turcica; STL, sella turcica length; STD, sella turcica depth; STDI, sella turcica diameter; STW, sella turcica width; STA, sella turcica area.
Relationships of ST measurements with sex and age of participants by binary logistic regression.

*Significant; **Highly significant.
CI, confidence interval; ST, sella turcica; STL, sella turcica length; STD, sella turcica depth; STDI, sella turcica diameter; STW, sella turcica width; STA, sella turcica area.
No statistically significant differences were observed in SS pneumatization patterns by age or sex. The distribution of SS pneumatization patterns was as follows: sellar, 59.6%; presellar, 16.2%; postsellar, 23.2%; and conchal, 1.0% (Table 4).
SS pneumatization patterns based on sex and age groups.

Table 5 shows that there was a significant negative correlation between ST size (STL, STW, and STA) and SS pneumatization, with p-values of 0.016, 0.002, and 0.010, respectively. A comparison of ST parameters and pneumatization patterns with existing literature revealed differences in measurements (Table 6).
Correlations between ST size (dimensions) and pneumatization patterns.

*Significant (point biserial correlation test).
ST, sella turcica; STL, sella turcica length; STD, sella turcica depth; STDI, sella turcica diameter; STW, sella turcica width; STA, sella turcica area.
Comparison of ST dimensions and SS pneumatization patterns between the present study and the literature.

ST, sella turcica; STL, sella turcica length; STD, sella turcica depth; STDI, sella turcica diameter; STW, sella turcica width; SD, standard deviation.
Discussion
The size and shape of the ST exhibit significant anatomical variations across different ethnicities and age groups. Establishing standard operating procedures for this critical region could facilitate the identification of structural anomalies.4,5 The findings of this study may assist neurosurgeons, otolaryngologists, and orthodontists in diagnosing and planning treatment for pituitary gland disorders. Additionally, ST measurements can serve as morphometric tools in forensic sciences and medicolegal issues and can help to determine the age and sex of deceased individuals. 15
The ST measurements in this study align with previously reported average values for length (5–16 mm) and depth (4–12 mm).5,16 Our findings showed that women had a greater average STD than men (OR, 2.498; p = 0.003), consistent with the report by Deepak et al. 17 In line with the current findings, Abebe et al. 18 analyzed 496 CT images and concluded that the STD varied significantly between the sexes. Likewise, Chauhan et al. 19 identified sex-related differences in STD. These differences were likely influenced by hormonal factors such as estrogen depletion post-menopause and hyperparathyroidism, which affect bone resorption. 20
Our results are consistent with those of Al-Dwairy et al., 14 who reported no significant differences in ST measurements between sexes and age groups, except for STD by sex and STDI by age group. Alkofide 4 found only slight sex-related differences in the Saudi population, suggesting that variations may be due to differences in the sex distribution and measurement techniques.
The STA was significantly different between the two sexes (men, 95.029 ± 19.397 mm2; women, 69.766 ± 20.502 mm2). Similarly, Keleş et al. 21 investigated 258 women and 282 men with a mean age of 50.52 years and found that the STA was significantly different between the sexes (p < 0.05). Turamanlar et al. 22 found a mean STA of 69.15 ± 17.45 mm2 among 101 healthy people aged 17 to 70 years.
In contrast to most studies, the present study showed higher values for all measured parameters. These disparities may be attributed to racial and environmental factors because the ST is highly variable and influenced by both genetic and environmental factors.17,18 Additionally, differences in results across studies could stem from variations in the age distribution and sample sizes of the research groups. The enlargement of the pituitary gland with age and somatic growth, particularly during puberty, likely contributes to the increasing size of the ST over time. Similar to the pattern of brain growth, the ST expands rapidly from birth until approximately 6 or 7 years of age. However, bone remodeling processes may continue to influence ST growth after puberty. 19
These findings align with previous studies that have demonstrated STDI enlargement with age due to bone remodeling.23,24 The sellar form of pneumatization was the most common, accounting for 59.6% of all SS pneumatization patterns, while the conchal type was the least prevalent at 1.0%. Neither Hiremath et al. (2018) 25 nor Abdalla (2020) 26 found evidence of the conchal type in their respective populations. The findings are consistent with those of Al-Dwairy et al., 14 who found that the sellar form of pneumatization was the type most frequently seen (66%) and that the conchal type was the least frequently seen (2%). Müderris et al. 27 (2021) examined the CT scans of 113 patients and found that 1.8% had conchal, 7.3% had presellar, 47.7% had sellar, and 43.3% had postsellar types.
Our findings are also in agreement with those of Gaddafi et al., 28 who reported that sellar and postsellar pneumatization of the SS were the most prevalent types (54.6% and 31.2%, respectively). Previous research has also demonstrated a higher prevalence of sellar and postsellar types than the conchal and presellar types.29–31 Given the clinical and surgical importance of these anatomical variants, a comprehensive preoperative assessment of the sinus is essential. The combined prevalence of sellar and postsellar pneumatizations in this study was 82.8%, and these types are particularly favorable for endoscopic endonasal transsphenoidal approaches. 32 These variants facilitate access to the sellar floor, as the floor and anterior wall of the sella are typically less than 1 mm thick. 27 However, the conchal type, because of its complex anatomy, is considered unfavorable for transsphenoidal surgery and has been linked to SS agenesis and retropharyngeal carotid arteries, making this approach contraindicated.11,33
Regarding the correlation between ST size and SS pneumatization, our study supports the findings of Lazzeroni et al., 34 who reported that smaller ST measurements are often associated with a highly pneumatized SS. This suggests that variations in SS pneumatization could impact ST size, particularly in cases of extensive SS pneumatization. Dogan et al. 35 examined CT scans of 420 people and identified a statistically significant association between SS shape, volume, and ST morphometrics, suggesting a potential connection between the ST and SS.
Understanding variations in SS pneumatization is crucial because it can significantly affect surgical planning and strategy. Surgeons must consider pneumatization types and levels to minimize the risk of iatrogenic injuries. A thorough understanding of pneumatization patterns is also essential for diagnosing sinus pathologies and improving patient care and surgical outcomes.36,37
This study contributes to the field by using CT scans to evaluate key anatomical landmarks in Iraqi patients, including ST dimensions, SS pneumatization patterns, and their interrelations. Notably, this is the first study to comprehensively assess all these anatomical features in a single publication, utilizing a novel anatomical morphometric method that may help identify ST variants in patients with different SS pneumatization patterns. This approach could lead to improved diagnosis and surgical outcomes in the future.
However, because this study was limited to CT images from a single center, caution is needed when generalizing these findings. Further large-scale, multicenter studies are required to confirm these results and provide a more comprehensive understanding of the frequency and characteristics of these CT findings.
Conclusions
This study showed no statistically significant differences in ST linear measurements across sex and age groups, except for STD by sex and STDI by age group. Additionally, no significant differences were found in SS pneumatization types. A significant negative correlation was observed between ST size (STL, STW, and STA) and SS pneumatization. These findings provide valuable information for surgeons employing the transsphenoidal approach, aiding in surgical decision-making.
Footnotes
Authors’ contributions
The authors designed the study, examined the data, established the methodology, gathered resources, and prepared and reviewed the original writing.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interest
The authors have no competing interests to declare that are relevant to the content of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed consent
Written informed consent was obtained from all participants.