
Abstract
Meningiomas are slow-growing benign lesions that constitute ∼ 25% of primary intracranial tumours. Extracranial meningioma of the sphenoid sinus is extremely rare and may arise from ectopic arachnoid nests left behind during embryonic development. We present the case of a 61-year-old woman with left oculomotor nerve paralysis. Magnetic resonance imaging (MRI) revealed a 43 × 31 × 33 mm mass in the sphenoid sinus invading anteriorly into the posterior ethmoid sinus and superiorly into the base of the anterior cranial fossa. Microscopic transnasal transsphenoidal surgery was performed with multilayer reconstruction to the cranial base. Postoperative MRI confirmed total resection and recovery was uneventful. The pathological diagnosis was grade I meningothelial meningioma. Meningioma should be included in the differential diagnosis of sphenoid sinus mass. Surgery is the first-choice treatment and a transnasal transphenoidal approach is recommended. Cranial base reconstruction is important to avoid postoperative cerebrospinal fluid leakage.
Introduction
Meningiomas are slow-growing benign lesions that constitute ∼25% of primary intracranial tumours. 1 Most meningiomas are located in the falx cerebri, convexity, tuberculum sellae, sphenoidal ridge or olfactory groove. The intraventricular and posterior fossae can also be involved. 2 Extracranial extensions of primary intracranial meningioma occur in up to 20% of cases, mostly involving the orbit, middle ear and soft tissues. Extensions into the nasal cavity and paranasal sinuses are rare, 3 and primary meningiomas of these locations are even less common. 4 Cases have been reported involving frontal sinuses, ethnoid sinuses and maxillary antrum, however. 5 Here we present an extremely rare case of meningioma of the sphenoid sinus, resected via a transnasal transsphenoidal approach.
Case study
A 61-year-old woman presented at the Department of Neurosurgery, Second Affiliated Hospital, School of Medicine, Hangzhou, China on 28 April 2014, complaining of vertigo and left eye blurred vision for the previous 12 days. She also described headache with nausea and vomiting but there was no history of fever, seizure, hearing loss, hydrouria or paralysis. Her medical history was unremarkable with the exception of a 1-year history of hypertension controlled with standard oral antihypertensives. Vital signs were stable. Neurological examination revealed blepharoptosis, oculomotor apraxia and dull pupillary light reflex of the left eye, attributed to left oculomotor nerve paralysis. Magnetic resonance imaging (MRI) revealed a 43 × 31 × 33 mm mass in the sphenoid sinus, invading anteriorly into the posterior ethmoid sinus and superiorly into the base of the anterior cranial fossa. The mass displayed a slightly hypointense signal on T1 weighted imaging (T1WI), a slightly hyperintense signal on T2WI and diffuse enhancement with contrast (Figure 1). Laboratory analyses found pituitary hormone levels and tumour markers were within normal range.
Magnetic resonance images of the head of a 61-year-old woman with sphenoid sinus meningioma. Preoperative images (a–d) revealed a mass in the sphenoid sinus (arrows), invading anteriorly into the posterior ethmoid sinus and superiorly into the base of anterior cranial fossa. (a) Sagittal T1 weighted image showing a slightly hypointense signal; (b) coronal T2 weighted image showing a slightly hyperintense signal; (c) coronal contrast image showing diffuse enhancement; (d) sagittal plane contrast image showing diffuse enhancement. Postoperative images (e–h) at 48h after surgery confirm total resection. (e) Sagittal T1 weighted image; (f) coronal T1 weighted image; (g) coronal contrast image; (h) sagittal plane contrast image. The colour version of this image (red arrows) is available at: http://imr.sagepub.com
Microscopic transnasal transsphenoidal surgery was performed 2 days after MRI, and a grey, firm textured mass with a rich blood supply was found in the sphenoid sinus (Figure 2). Damage was visible to the anterior, inferior and superior walls of the sphenoid sinus. A biopsy was taken and meningioma was suspected. The tumour was resected using a pericapsular dissecting technique and intracavitary decompression. Cerebrospinal fluid leakage occurred when the tumour base was removed from the anterior cranial fossa dura. Multilayer reconstruction was performed using Duraform® dural graft implant (DePuy Synthes, West Chester, PA, USA), fat graft and fascia lata. Lumbar drainage was removed on the seventh postoperative day.
Intraoperative photograph of sphenoid sinus meningioma in a 61-year-old woman, which presented as a grey, firm-textured mass. The colour version of this figure is available at: http://imr.sagepub.com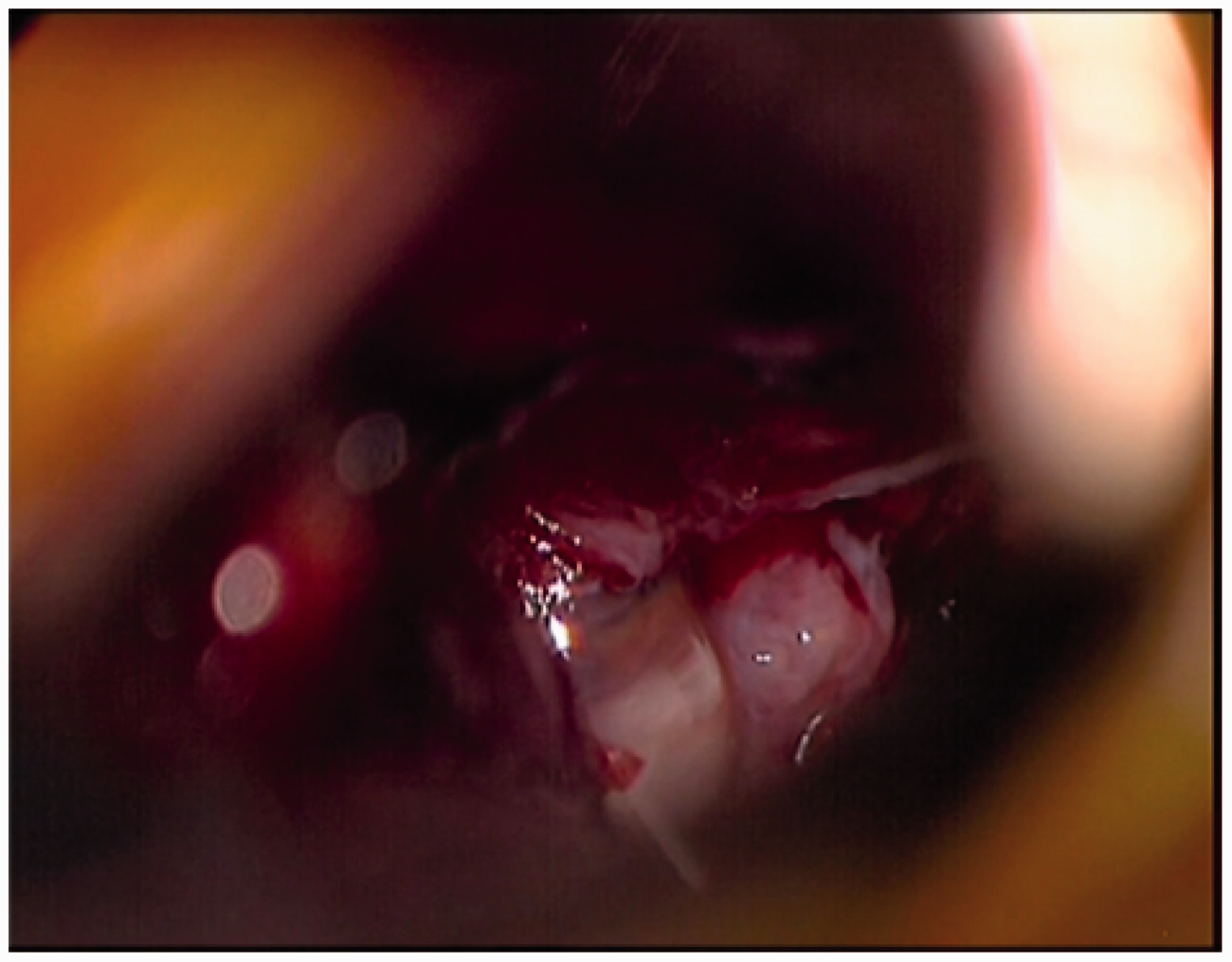
The patient had an uneventful recovery without additional neurological deficit except persistent oculomotor nerve paralysis. Postoperative MRI confirmed total resection. The final pathological diagnosis was grade 1 meningothelial meningioma (WHO classification 6 ). Immunohistochemistry revealed positive staining for epithelial membrane antigen and vimentin.
The patient provided written informed consent for publication of this case report and any accompanying images. The School of Medicine, Hangzhou, China, does not require ethical approval for reporting individual cases.
Discussion
Meningioma is the third most frequent intracranial tumour type, and is known to arise from arachnoid cells. 7 Extracranial meningiomas, although rare, have been reported and are clinically classified as primary and secondary subtypes according to origin from the extracranial and intracranial regions, respectively. 8 Meningiomas originating in the paranasal sinuses are extremely rare and are thought to arise from ectopic arachnoid nests left behind after embryogenesis. 9
Published cases of sphenoid sinus meningioma.
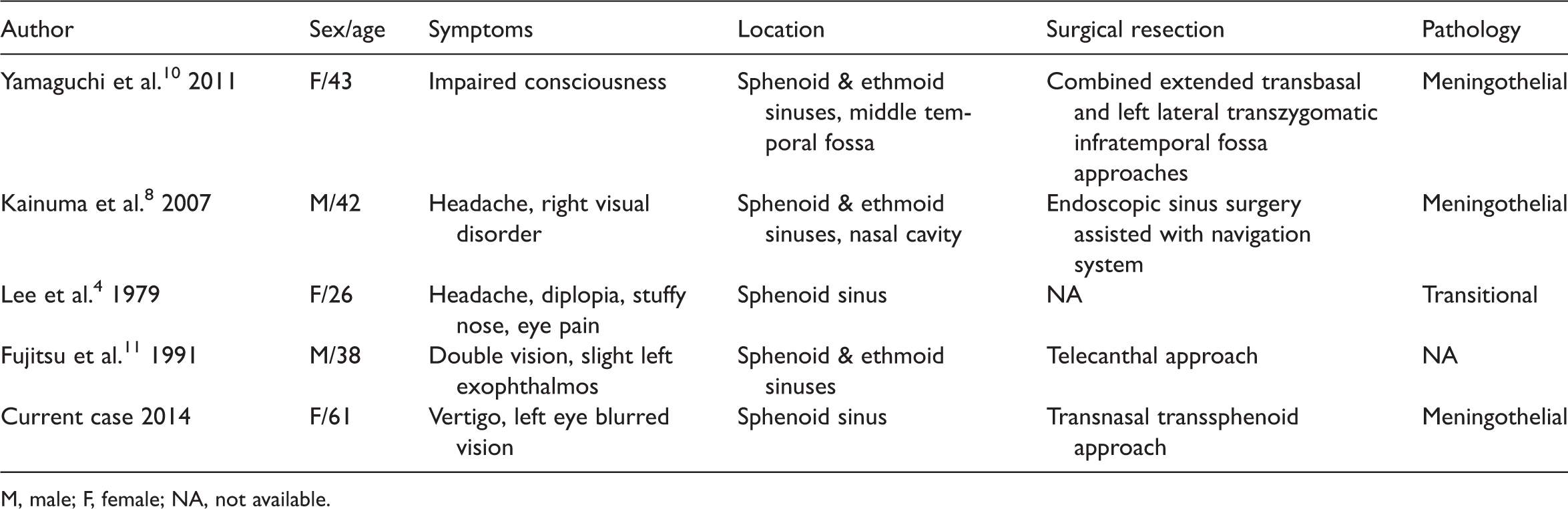
M, male; F, female; NA, not available.
Meningioma typically appears as an isodense or hyperdense mass on computed tomography (CT) images. MRI of menagioma generally reveals an isointense mass on T1WI and T2WI that is intensely enhanced with contrast and displays a dural tail sign. 12 Meningioma of the sphenoid sinus can lack these distinguishing radiological characteristics, thereby complicating preoperative diagnosis. 12 Differential diagnoses include mucocele, aneurysmal bone cyst, giant-cell lesions, meningioma, fibrous dysplasia, chordoma, craniopharyngioma, rhabdomyosarcoma, sinonasal carcinoma and neuroblastoma. 12 A careful study of T1-contrast MRI images in our case revealed a hyperintensified signal at the anterior cranial base, possibly due to abnormal thickening of the dura matter. This could be viewed as an atypical dural tail sign, and may help with preoperative diagnosis.
Surgical resection is the first-choice treatment for meningioma due to tumour radioresistance and the potential for radiation induced-injury to surrounding tissues. 13 The transnasal transsphenoidal approach is direct, has a good safety profile and is minimally invasive. 14 Moreover, it is easy to obtain a tissue sample for frozen biopsy, allowing rapid tumour classification and enabling the surgeon to determine the optimum resection technique. It is important to dissect along the neoplasm capsule and handle the feeding artery and draining vein properly in order to minimize bleeding and keep the surgical field clear. The tumour capsule and its attachment to the anterior cranial base should be excised in order to achieve Simpson grade I resection and avoid recurrence. 15 The requirement for cranial base reconstruction should be considered preoperatively, since cerebrospinal fluid leakage is inevitable once the anterior cranial base attachment is resected. Multilayer reconstruction is recommended according to lesion size, intradural or extradural location, and occurrence of intraoperative leakage. 16 From our experience, multilayer sealing with Duraform®, fat graft, fascia lata and possibly a nasoseptal flap was sufficient and effective. In this case, total resection was achieved and the patient had an uneventful recovery.
In conclusion, we report a case of sphenoid sinus meningioma resected via a microscopic transnasal transphenoidal approach. Total resection was achieved and recovery was uneventful. Although meningioma at this site is extremely rare, it should be considered as part of the differential diagnosis of sphenoid sinus mass. Surgery is the first choice treatment, and the minimally invasive transnasal transphenoidal approach is recommended. Cranial base reconstruction is important to avoid postoperative cerebrospinal fluid leakage.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.