
Abstract
Objective
To determine the risk factors associated with peripheral intravenous therapy infiltration and extravasation (PIVIE) in paediatric surgery inpatients.
Methods
This retrospective observational study was conducted at a tertiary general hospital in Sichuan, China. Logistic regression was employed to identify independent risk factors predictive of PIVIE. Kaplan–Meier survival analysis was undertaken to determine the relationship between the occurrence of PIVIE and the duration of that event (survival time).
Results
This study included 11 006 paediatric surgery inpatients and 19 771 peripheral intravenous catheters (PIVCs). The incidence of PIVIE was 16.93% (3347 of 19 771). The following were significant predictors of PIVIE: sex (odds ratio [OR] 0.834; 95% confidence interval [CI] 0.772, 0.900); age (OR 0.945; 95% CI, 0.934, 0.956); disease classification (OR 0.962, 95% CI 0.950, 0.976); puncture site (OR 1.061; 95% CI 1.044, 1.078); and indwelling time (OR 1.257; 95% CI 1.215, 1.300).
Conclusions
Sex, age, type of disease, puncture site and indwelling time were risk factors for PIVIE. The puncture site should be effectively assessed and accurately selected. Informed judgements should be based on the child’s sex, age and medical condition, so that the appropriate preventive measures to minimize the risk of PIVIE can be implemented.
Keywords
Introduction
Intravenous therapy is one of the most commonly employed and effective treatment methods in clinical practice. 1 Superficial peripheral veins serve as the preferred route for short-term intravenous therapy. 2 Compared with deep venous catheters, peripheral intravenous catheters (PIVCs) offer advantages such as ease of operation, safety and convenience. 3 Despite these benefits, the occurrence of complications associated with PIVCs remains a concern for both patients and nursing staff, highlighting the need for stringent quality and safety control in intravenous fluid administration. 4
The 2024 Infusion Therapy Standards of Practice, published by the Infusion Nurses Society, emphasizes that newborns and children should be recognized as a distinct group of specialized patients, necessitating individualized, collaborative and age-appropriate care. 3 Children often experience significant challenges with venipuncture and exhibit poor cooperation following successful puncture, leading to a markedly higher incidence of complications compared with adults. 5 Research indicates that the use of PIVCs for intravenous infusion therapy in hospitalized children can result in complication rates ranging from 18.9% to 71%, including issues such as phlebitis, infiltration, extravasation, catheter blockage and accidental catheter detachment.5–7 Peripheral intravenous therapy infiltration and extravasation (PIVIE) is one of the most common complications associated with intravenous therapy, with an incidence of exudation ranging from 6% to 87%.1,5,8,9 This condition not only impairs the effectiveness of intravenous treatment in children but can also lead to local skin redness, swelling and discomfort. In severe cases, PIVIE may result in tissue ulceration, necrosis, scarring or dysfunction. 10 Compared with adults, children exhibit several unique characteristics, including a significantly reduced thickness of the skin cell layer, narrower blood vessel diameters, a more fragile vascular system, decreased adhesion between the dermis and epidermis, and highly flexible and expandable subcutaneous tissue. These factors contribute to a higher incidence of PIVIE-related damage in paediatric patients compared with adults. 11 Consequently, the management of intravenous therapy in this population poses significant challenges.1,5,6 With regard to the definition of infiltration and extravasation, both refer to unintended leakage of fluids. 12 Infiltration involves the leakage of a non-vesicant solution into the surrounding tissue, which is a relatively common occurrence and may result in symptoms such as redness, swelling, pain or discomfort. In contrast, extravasation pertains to the leakage of vesicant fluid from a blood vessel into the surrounding tissue. Both conditions can lead to serious complications; in extreme cases, interventions such as surgical debridement, skin grafting or even amputation may be necessary.
Therefore, this current study investigated the current situation of PIVIE in paediatric patients at a tertiary general hospital in China with the aim of providing nursing staff with a reference for evaluating, identifying and managing intravenous infusion infiltration and extravasation.
Patients and methods
Study design and participants
This retrospective observational study enrolled consecutive patients Department of Paediatric Surgery, West China Hospital of Sichuan University, Chengdu, Sichuan Province, China between January 2021 and December 2021. The Department of Paediatric Surgery at this hospital encompasses various specialties, including Paediatric Neurosurgery, Paediatric Ophthalmology, Paediatric Otolaryngology Surgery, Paediatric Burn Plastic Surgery, Paediatric Cardiovascular Surgery, Paediatric Thoracic Surgery, Paediatric Urology, Paediatric Orthopaedic and Trauma Surgery and the Paediatric General Surgery Ward. The inclusion criteria were as follows: (i) age 0–14 years; (ii) non-intensive care unit paediatric surgery inpatients who had undergone peripheral intravenous catheter insertion. The exclusion criteria were as follows: (i) incomplete or incorrect data collection.
As this study was a retrospective analysis, the Ethics Committee of West China Hospital of Sichuan University approved the study and waived the requirement for patient consent forms. However, each patient had a standard consent form signed by their authorized representative prior to venipuncture. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013. All information was kept confidential and all patient details were de-identified. The reporting of this study conforms to STROBE guidelines. 13
Sampling and sample size
This study used cluster sampling. The following formula was used to calculate the required sample size: n = μ2α/2P(1−P)/δ2, where n is the sample size, μ is the population mean, α is the Type I error probability, P is the estimated PVC failure rate and δ is the allowable error. Assuming 45% PIVIE, the calculated sample size was 9508.
Data collection
Using the Personal Digital Assistant (PDA) information system, data on PIVIE events among inpatients in the Department of Paediatric Surgery at West China Hospital of Sichuan University were collected from January 2021 to December 2021. The collected data included the child’s name, hospitalization number, sex, age, diagnosis, date of the event, presence of PIVIE, location of PIVIE, grade of PIVIE and the indwelling time of PIVCs.
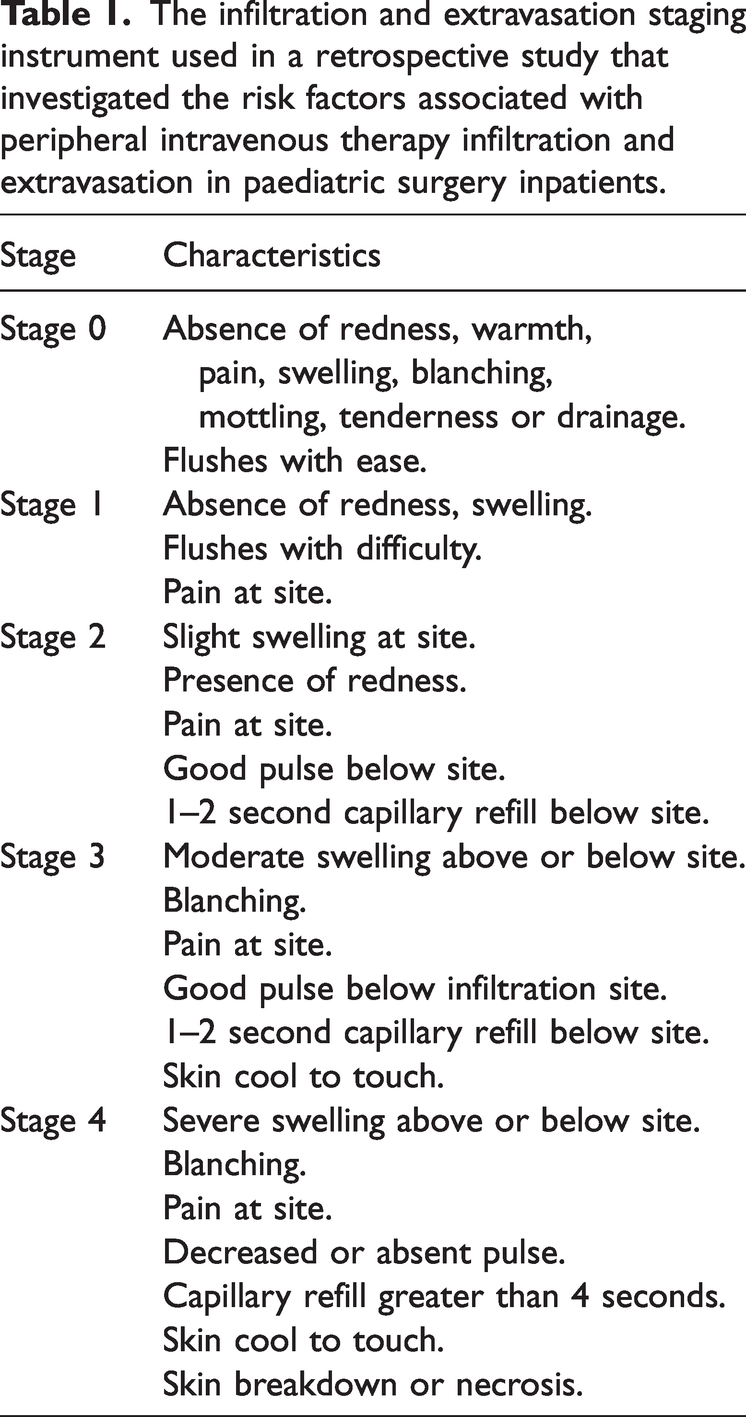
The data collection of PIVIE events in paediatric surgery inpatients was conducted in two phases. In the first phase, involving the use of the PDA information system, the nurse registered the insertion of the PIVC by scanning the wristband. Upon discontinuation of the PIVC, the nurse scanned the wristband again to record the event. The PIVIE was documented using the infiltration and extravasation staging instrument (Table 1). In the second phase, which focused on the backend organization of the PDA information system, specialized nurses responsible for intravenous infusion treatment logged into the Hospital Information System backend weekly to organize and eliminate invalid or incorrect data. They subsequently reported this information to the quality control department of the hospital’s nursing division for summary.
The infiltration and extravasation staging instrument used in a retrospective study that investigated the risk factors associated with peripheral intravenous therapy infiltration and extravasation in paediatric surgery inpatients.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Normally distributed data are presented as mean ± SD, while data that were not normally distributed are reported as median and interquartile range. Categorical data are presented as frequencies and proportions. The frequency of PIVIE was calculated and both univariate and multivariate logistic regression analyses were conducted to identify predictors of PIVIE. Univariate analysis utilized the χ2-test and statistically significant variables (P < 0.05) were subsequently included in the multivariate analysis. Odds ratios (ORs) along with their corresponding 95% confidence intervals (CIs) were calculated. Additionally, a Kaplan–Meier survival function graph was generated and a log-rank test was performed. A P-value <0.05 was considered statistically significant.
Results
This retrospective study included a total of 11 006 paediatric surgery inpatients, all of whom were admitted to various paediatric surgical departments to treat a wide range of medical conditions. Patient demographics are summarized in Table 2. The mean ± SD age of the paediatric surgery inpatients was 4.58 ± 3.481 years (range, 0–14 years), with 6913 (62.81%) being males and 4093 (37.19%) being females. Ear, nose, throat and neck diseases were the most prevalent, affecting 1994 (18.12%) of 11 006 paediatric surgery inpatients. A total of 6807 of 11 006 patients (61.85%) utilized only one PIVC during their hospitalization.
Patient and catheter characteristics in a retrospective study that investigated the risk factors associated with peripheral intravenous therapy infiltration and extravasation in paediatric surgery inpatients (n = 11 006).

Data presented as n (%).
A total of 19 771 PIVCs were investigated in this study and their characteristics are presented in Table 2. Among these, 10 428 catheters (52.74%) were inserted on the back of the hand. A total of 3347 catheters (16.93%) experienced PIVIE, the majority of which were classified as Grade 0 (3266; 16.52%), with no occurrences of Grade 4 PIVIE. Additionally, 12 340 catheters (62.41%) had an indwelling retention time of 24 h < t ≤ 48 h.
As shown in Table 3, the incidence of PIVIE was 18.39% (1417 of 7705 catheter insertions) among females (P < 0.05). Significant differences in the incidence of PIVIE were observed across different age groups (P < 0.05), with the lowest incidence reported in paediatric surgery inpatients aged 3 < age ≤ 6 years (881 of 7451 catheter insertions; 11.82%) and the highest in those aged 1–12 months (886 of 2961 catheter insertions; 29.92%). Additionally, there was a statistically significant difference in the incidence associated with various disease types (P < 0.05). The incidence of PIVIE in paediatric surgery inpatients with liver, gallbladder, pancreatic and splenic diseases was 59.59% (839 of 1408 catheter insertions). A significant difference in the incidence of PIVIE was observed among the various puncture sites (P < 0.05), with the highest incidence occurring at the head puncture site, recorded at 36.94% (140 of 379 catheter insertions). Additionally, there was a significant difference in the retention time of the PIVCs (P < 0.05), with the lowest incidence of PIVIE noted within an indwelling retention time of 24 h < t ≤ 48 h.
Comparison of the incidence of infiltration and extravasation according to several variables in a retrospective study that investigated the risk factors associated with peripheral intravenous therapy infiltration and extravasation in paediatric surgery inpatients (n = 11 006).

Data presented as n (%).
Univariate analysis utilized the χ2-test.
A multivariate logistic regression analysis was conducted with PIVIE as the dependent variable, while a univariate analysis was performed to examine the factors associated with PIVIE as independent variables. The findings from the logistic regression analysis are presented in Table 4. The results indicated that sex, age, disease classification, puncture site and indwelling time were identified as risk factors for the occurrence of PIVIE (P < 0.05).
Multivariate logistic regression analysis of predictors of infiltration and extravasation in a retrospective study that investigated the risk factors associated with peripheral intravenous therapy infiltration and extravasation in paediatric surgery inpatients (n = 11 006).

Univariate analysis utilized the χ2-test and statistically significant variables (P < 0.05) were subsequently included in the multivariate analysis.
OR, odds ratio; CI, confidence interval.
Survival analysis is a statistical method that assesses the relationship between the occurrence of an event (designated as PIVIE in this study) and the duration of that event (survival time). In this research, survival analysis was employed to examine the time from the placement of each peripheral venous catheter to the onset of PIVIE. The maximum duration of indwelling needle use was set at 7 days, which constituted the observation period; and the occurrence of PIVIE was identified as the endpoint event. In addition, factors such as sex, age, disease classification and puncture site were incorporated into the survival analysis. As shown in Figure 1, the cumulative survival curve of PIVCs in paediatric surgical patients declined as the observation time increased. When comparing the two sexes, the curve for the male group was relatively flat, indicating a longer survival period for the indwelling needle in this group (Figure 2). In terms of age, the curve for the 1–12 month age group was the steepest, suggesting that this group experienced the shortest survival time for indwelling catheters. Among different disease categories, the curves for the liver/gallbladder/pancreas and splenic disease groups were the steepest, indicating that these groups had the shortest survival periods for indwelling catheters. Furthermore, when examining puncture sites, the groin and elbow groups exhibited flatter curves, which indicated a longer survival time for indwelling catheters in these areas. The differences observed between the groups were statistically significant (P < 0.05; Figure 2).

Kaplan–Meier survival curve of 19 771 peripheral intravenous catheters in a retrospective study that investigated the risk factors associated with peripheral intravenous therapy infiltration and extravasation in paediatric surgery inpatients (n = 11 006).

Kaplan–Meier survival curves of 19 771 peripheral intravenous catheters with different characteristics in a retrospective study that investigated the risk factors associated with peripheral intravenous therapy infiltration and extravasation in paediatric surgery inpatients (n = 11 006). The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
In paediatric surgery, perioperative intravenous infusion therapy for paediatric surgery inpatients is typically short-term, leading to the frequent use of PIVCs during hospitalization. The findings of this current retrospective study indicated that 61.85% of paediatric surgery inpatients utilized a single peripheral venous indwelling needle, while some required two or more such needles to fulfil the demands of perioperative intravenous infusion treatment.
The results of this current study indicated that the incidence of PIVIE was 16.93%, which is higher than that observed in adults. 14 These findings align with existing research on PIVIE in children, both domestically and internationally.10,15–18 An analysis of the incidence of PIVIE in the two sexes in the current study demonstrated that the incidence was significantly higher in girls compared with boys, which contradicts the findings reported previously in a paediatric cohort, 10 which noted that 66.7% of PIVIE cases occurred in boys. This discrepancy may be attributed to significant differences in sample sizes. Furthermore, the results of the univariate analysis indicated that the incidence of PIVIE was greater in paediatric surgery inpatients aged 1–12 months compared with the other age groups. This may be due to factors such as an immature immune system, poor coordination and thicker subcutaneous fat in children aged 1–12 months, which can lead to a lower quality of peripheral indwelling needle puncture compared with older children. In this current study, the incidence of PIVIE was found to be highest among paediatric surgery inpatients with liver, gallbladder, pancreatic and splenic diseases, with the shortest survival time observed in those with indwelling catheters. This may be attributed to factors such as compromised skin integrity, poor nutritional status, skin itching and diminished vascular visibility in this patient population. Regarding the impact of the puncture site on the incidence of PIVIE, a systematic review of adults indicated no statistically significant difference in PIVIE incidence between the forearm and the back of the hand. 15 The 2024 version of the ‘Practice Standards for Infusion Therapy’ recommends the forearm as the preferred location for peripheral venous indwelling catheters, with the dorsal vein of the hand being considered only for short-term infusion therapy (less than 24 h). 3 In this current study, the head exhibited the highest incidence of PIVIE. Although the back of the hand is the most commonly utilized puncture site, its incidence of PIVIE was lower compared with that of the head and forearm. A global survey demonstrated that two-thirds of PIVCs are inserted at the flexion site; however, complications such as PIVIE in this area can easily lead to nerve damage. 19 In summary, considering the characteristics of thick subcutaneous fat and the limited visibility of forearm veins in children, prioritizing dorsal hand puncture for peripheral vein indwelling in this population is recommended.
The cumulative survival curve of the peripheral indwelling catheters in patients included in this study showed a decline with increasing observation time. Notably, the survival time of the indwelling catheters was the shortest in the 1–12 month age group, aligning with previous findings. 10 As early as the 2011 edition of the Standards of Practice for Infusion Nurses, the recommended retention time for PIVCs was revised to be based on clinical indications. A previous study reported that recent advancements in the materials used for PIVCs have significantly reduced irritation to blood vessels. A randomized controlled study aimed at determining the optimal timing for peripherally inserted central catheter replacement revealed that, while the mean retention time for PIVCs was 70 h, it extended to 99 h when PIVCs were replaced according to clinical indications. 20 Importantly, there was no significant difference in the incidence of phlebitis between the two patient groups, both of which reported an incidence rate of 7%. 20 Promoting the replacement of PIVCs based on clinical indications not only reduces patient medical expenses but also minimizes the frequency of needle insertion pain, thereby conserving nursing resources. For indwelling catheters that have been in place for 24 h, it is recommended that nurses evaluate the intravenous insertion site hourly to ensure safer intravenous injection practices. 21
At present, many researchers both domestically and internationally have made efforts to reduce the occurrence of PIVIE. The fixation of peripheral indwelling catheters is crucial for minimizing the occurrence of extravasation. Research indicates that employing new fixation products, such as octyl-butyl-cyanoacrylate adhesive, tissue adhesives and integrated fixation dressings, can significantly reduce the risk of PIVC failure. Consequently, this intervention should be considered for hospitalized patients, particularly those with anticipated longer hospital stays.2,22,23 Several researchers have used new sensor technology to provide early warning of PIVIE events in the neonatal population. 24 Previous research demonstrates that, according to the principles of feedforward control, minimizing risk factors associated with the extravasation of neonatal intravenous infusions can lead to a reduction in the incidence of extravasation. 25 The Intravenous Infiltration and Extravasation Risk Assessment Tool (IIERAT) has been specifically developed for assessing the risk of venous infiltration and extravasation in paediatric patients. 26 Additionally, several researchers have focused on enhancing the quality of nursing practices to minimize the incidence of infiltration and extravasation.18,27–29
In summary, when managing PIVIE in paediatric surgery inpatients, it is particularly important to master the selection and early identification of each infusion site. Utilizing the ‘5 Rights of Venous Access’, the Right device, for the Right vein, with the Right therapy, for the Right duration, for the Right patient, can lead to better outcomes and prevent unnecessary catheter-related complication. 30
This current study had several limitations outlined as follows. First, it is important to note that this was a single-centre retrospective study. While the sample size was substantial, the hospital’s structural constraints resulted in the inclusion of only paediatric surgery-related patients, which limits the generalizability of the findings. Secondly, the initial design of the information system focused solely on the infiltration and extravasation of peripheral venous catheters as outcome indicators, leading to the omission of other complications associated with peripheral venous catheters. Moving forward, it is essential to enhance the research design and undertake multicentre, prospective studies to address the limitations identified in this study.
In conclusion, PIVCs are the most commonly utilized intravenous infusion devices for paediatric surgery inpatients. Factors such as sex, age, type of disease, puncture site and duration of indwelling were identified as independent risk factors for PIVIE. Therefore, it is necessary for nurses to effectively assess and accurately select the puncture site, make informed judgements based on the child’s sex, age and medical condition, and implement appropriate preventive measures to minimize the risk of PIVIE.
Footnotes
Acknowledgements
We extend our sincere gratitude to all the patients who participated in this study.
Author contributions
WenJiao Huang: Conceptualization, Methodology, Software, Data curation, Writing – Original draft preparation. Zheng Liu: Visualization, Investigation. Hong Zhu: Supervision. Liwei Feng: Software, Validation.
Data availability statement
All data are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research was supported by the Sichuan Provincial Department of Science and Technology Project (2022JDKP0064). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.