
Abstract
Uterine smooth muscle tumors of uncertain malignant potential (STUMPs) are rare tumors of the uterine myometrium that are often misdiagnosed, owing to limited knowledge of their characteristics on ultrasonography (US) and magnetic resonance imaging (MRI). We report a woman in her mid-30s who was hospitalized because of a pelvic tumor. A 6-cm mass was found in her lower left abdomen. US and MRI revealed a well-demarcated mass in the left adnexal area, with both cystic and solid elements, visible blood flow within the septa, a strong signal across >50% of the volume on T2-weighted imaging (T2WI), and a strong signal on diffusion-weighted imaging (DWI). After hysterectomy and bilateral salpingectomy, immunohistochemical examination confirmed STUMP. A review of the literature revealed characteristic imaging features of STUMP. Ultrasonography reveals STUMP as a solitary, well-circumscribed lesion with isoechoic or mixed echogenicity, the absence of posterior shadowing, and variations in blood flow. STUMP is characterized by strong signal intensity on T2WI, small areas of strong signal on T1WI, and non-enhancing cystic areas on contrast-enhanced MRI scans. Early diagnosis is crucial for the management and treatment of STUMP, and here we have summarized the imaging features of the lesion, thereby providing a valuable diagnostic reference.
Keywords
Introduction
Uterine smooth muscle tumors encompass a spectrum of histologically heterogeneous and clinically diverse diseases, ranging from malignant leiomyosarcomas to benign leiomyomas. These also include a rare category of tumor1–3 that is challenging to classify definitively as benign or malignant, owing to its intermediate histopathologic characteristics. These tumors account for approximately 0.01% of all surgically treated smooth muscle tumors. 4 The World Health Organization classifies these indeterminate tumors as uterine smooth muscle tumors of uncertain malignant potential (STUMP). Clinicians need to exercise caution, because these tumors have a moderate potential for malignancy and may show local recurrence and/or distant metastasis.
Previous studies5–8 using medical imaging modalities have shown that the principal manifestation of STUMP is a well-demarcated heterogeneous mass, usually with cystic changes, with both benign and malignant characteristics. However, owing to the rarity of these lesions and the few previous reports, 9 especially regarding their features on ultrasonography (US) and magnetic resonance imaging (MRI), clinicians often have inadequate knowledge regarding such tumors, resulting in frequent misdiagnosis.
To address this lack of knowledge, we have combined the reporting of a case of STUMP encountered at our hospital with a literature review, in which we summarize the features of these tumors on US and MRI, to facilitate early diagnosis.
Case presentation
We report the case of a woman in her mid-thirties who was hospitalized because of the incidental discovery of a pelvic tumor 2 days earlier. Her family history was unremarkable. No significant abnormalities were identified on laboratory testing. The patient was in good general condition, and there were no obvious abnormalities on cardiopulmonary auscultation or abdominal examination. Her vulva had an appearance consistent with previously giving birth; her vagina was normal, with a small amount of white, odorless secretion; her cervix was smooth and of normal appearance, with no bleeding when manually examined; and her uterus was in a posterior position, of normal size, and regular in shape. A solid mass of approximately 6 cm in diameter was detected in the left adnexal region, which was hard, mobile, and not painful.
US revealed that the uterus was located posteriorly, was regular in shape, had a homogeneous myometrial echotexture, had a centrally located endometrium, and was approximately 1.1 cm thick. A 7.3-cm ×4.2-cm × 5.8-cm mixed cystic/solid mass was identified in the left adnexal region, and this contained multiple irregular septa and some solid structures. Color Doppler flow imaging (CDFI) revealed strip-like blood flow signals within the septa, with a pulsed-wave Doppler resistance index of 0.37 (Figure 1).
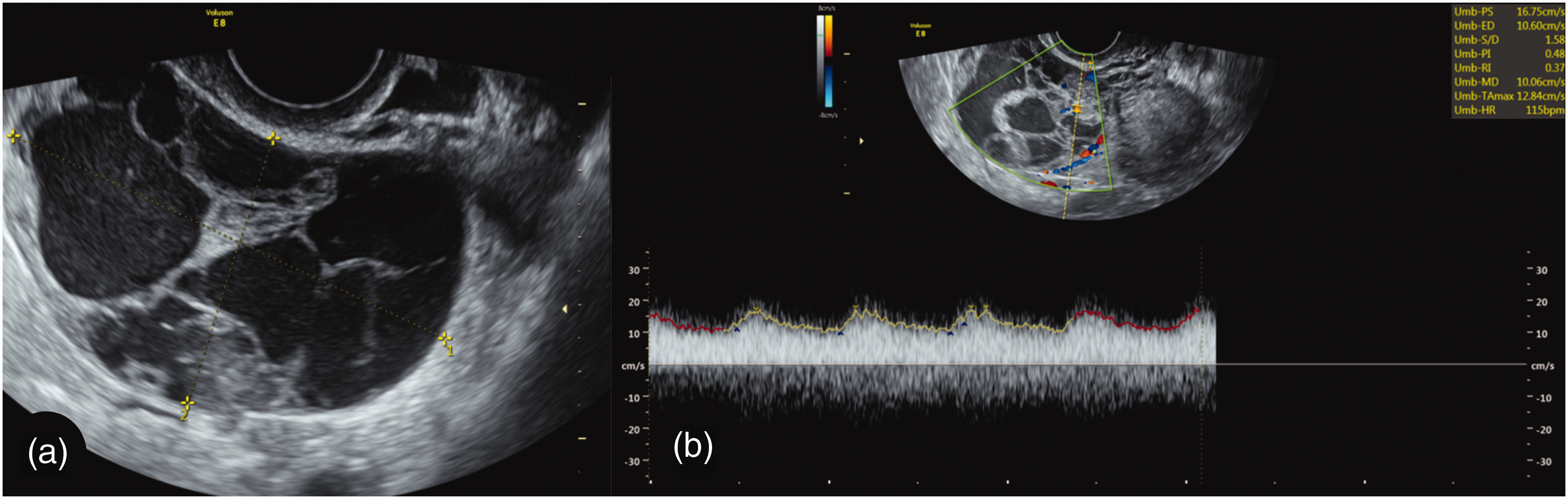
Ultrasonographic images. (a) A 7.3-cm × 4.2-cm × 5.8-cm cystic/solid mass was detected in the left adnexal area, and this had multiple irregular septa, some of which were solid and (b) Color Doppler flow imaging revealed strip-like blood flow signals within the septa. Pulsed-wave Doppler indicated a resistance index of 0.37.
MRI revealed that the uterus was in a central position, was normal in size, and had a regular endometrium with no thickening. The myometrium of the uterine body displayed a homogeneous signal intensity and no abnormal signals. A 7.6-cm × 5.2-cm mixed cystic/solid lesion was identified in the left adnexal region, with the solid component appearing iso- to slightly hyperintense on T1-weighted imaging (T1WI) and hyperintense on T2-weighted imaging (T2WI). Over 50% of the volume showed a strong signal on T2WI and there was also a strong signal on diffusion-weighted imaging (DWI). The lesion was attached to the patient’s left uterine wall, but no enlarged lymph nodes were identified in the pelvic cavity (Figure 2).

Magnetic resonance images. (a) A 7.6-cm × 5.2-cm mixed cystic/solid lesion was identified in the left adnexal area. The lesion exhibited mixed signals, which were generally iso- to slightly hyperintense on T1-weighted imaging (a), and hyperintense signals on T2-weighted imaging (T2WI), with over 50% of the area showing a strong T2WI signal (b) diffusion-weighted imaging indicated that the lesion was attached to the left uterine wall (c) and showed restricted diffusion (d).
The patient underwent total hysterectomy and bilateral salpingectomy. After the successful induction of anesthesia, a laparotomy was performed, during which a soft mass of approximately 6 cm in diameter, with a wide insertion on the left anterior wall of the uterus, was identified. The adnexa appeared normal bilaterally. Inspection of the peritoneum in the pelvic and abdominal cavities, uterorectal pouch, vesicular peritoneal reflection, intestines, greater omentum, liver, spleen, and subdiaphragmatic region of the patient showed no significant abnormalities. No enlarged lymph nodes were detected near the abdominal aorta or iliac vessels. A rapid pathologic examination indicated that the lesion was a low-grade malignant mesenchymal tumor of the uterine serosa, potentially a uterine perivascular epithelioid cell tumor or a low-grade epithelioid leiomyosarcoma, which would require immunohistochemical differentiation. Postoperative pathologic examination showed that it was a low-grade malignant epithelioid leiomyosarcoma of the uterus, with microscopic examination revealing slightly atypical cells with epithelioid characteristics. Immunohistochemistry revealed the following: cytokeratin (CK) broad-spectrum (−), CK CAM5.2 (−), epithelial membrane antigen (EMA) (−), human melanoma black (HMB)45 (−), leukocyte common antigen (LCA) (−), transcriptional repressor GATA binding (TRPS)1 (+), GATA-binding protein 3 (−), cluster of differentiation (CD)10 (−), H-caldesmon (scattered positive), desmin (2+), smooth muscle actin (SMA) (2+), smooth muscle (+), (discovered on GIST-1 (DOG-1) (−), CD138 (−), CD117 (−), CD34 (−), melan-A (−), inhibin-a (−), Sal-like protein (SALL4) (−), S-100 (−), CD38 (−), and Ki-67 (positive, 18% to 23%). These findings were consistent with STUMP of the uterus (Figure 3).

Histopathologic findings. (a) Epithelioid tumor cells arranged in trabeculae and sheets, with abundant eosinophilic cytoplasm, mild atypia, and occasional mitotic figures, but no tumor necrosis. Hematoxylin and eosin; ×200 and (b) the Ki-67 proliferation index was high, reaching 23% in active areas. EliVision immunohistochemical staining; ×200.
The patient did well postoperatively and did not experience complications. After discharge from the hospital, follow-up was planned for every 6 months for the first 5 years postoperatively and annually for the following 5 years. At the time of writing, the patient was doing well and was satisfied with the treatment plan and her recovery.
Discussion
Uterine STUMP, which was initially described by Kempson, is a rare smooth muscle tumor that arises from the myometrium and cannot be definitively classified as benign or malignant. Patients with STUMP have a mean age of 41 to 48 years, and the tumor can recur, metastasize, or progress to leiomyosarcoma. 10 The recurrence rate for STUMP is 36.4%, with a median time to recurrence of approximately 51 months. 9 The overall 5-year survival rate ranges from 92% to 100%. 11 A recent cohort study 12 performed in Italy comprised a review of 1010 charts that included nine postoperative diagnoses of STUMP. In all cases, the lesions were solitary and intramural, but they were relatively large, with a mean diameter of approximately 7.5 cm, which is consistent with the characteristics of the present case. In addition, this study showed that STUMP typically appears before the age of 50 years, which is also consistent with the present patient.
The low incidence and few reported clinical features of STUMP have led to poor levels of recognition by clinicians. In addition, the rapid growth and large size of STUMP lesions renders diagnostic imaging difficult, leading to confusion between STUMP lesions and other smooth muscle tumors. 13
On US, STUMP usually appears as a large, oval-shaped tumor with heterogeneous internal echogenicity. 5 It has previously been stated that a single irregular tumor without acoustic shadowing and the presence of free fluid are strongly associated with STUMP. 6 However, Cotrino et al. reported that specific US features should prompt suspicion of STUMP, including a well-defined mass with isoechoic or mixed echogenicity, possible anechoic areas or small cystic spaces, and significant differences in vascularization within and outside the mass. 9 In contrast, benign fibroids usually appear as well-defined, homogeneously echogenic, solid masses that rarely have a cystic component or significant differences in vascularization. In contrast, malignant fibroids and leiomyosarcomas tend to have more aggressive features, such as poorly defined borders, uneven internal echogenicity, and significant vascular hyperplasia. The US findings for the present patient were consistent with the typical features of STUMP, with clear lesion boundaries indicating a low level of invasiveness, but mixed echogenicity hinting at potential malignancy.
Tanaka et al. 7 reported that if >50% of the affected volume has strong signal intensity on T2WI, there are small areas of strong signal intensity on T1WI, and there are non-enhancing cystic areas after contrast enhancement, there should be a suspicion of STUMP or leiomyosarcoma. Tasaki et al. 8 discovered that STUMP is associated with a stronger signal intensity on T2WI than leiomyoma. Strong DWI signal intensity and a weak apparent diffusion coefficient (ADC) signal suggest malignant potential of the lesion. Uneven enhancement after the administration of contrast material is also indicative of malignancy. In contrast, benign uterine fibroids usually generate well-defined and homogeneous signals on MRI. On T1WI and T2WI, fibroids generate a low-intensity signal, and enhanced scans show a homogeneous enhancement pattern. 8 Malignant uterine fibroids and uterine leiomyosarcomas usually generate a heterogeneous signal on MRI and may also demonstrate internal hemorrhage, necrosis, or cystic changes. DWI is usually associated with a high signal intensity and a low signal intensity on ADC maps. Enhanced scans show non-homogeneous enhancement and indicators of invasiveness. 7 In the present patient, MRI revealed that >50% of the volume had a strong T2WI signal, which markedly differs from that associated with benign uterine leiomyoma and suggests possible malignancy.
According to the 2019 Italian Association of Medical Oncologists guidelines, immunohistochemical assessment of progesterone receptor, p53, and Ki67 expression is helpful for the differential diagnosis of smooth muscle sarcoma, smooth muscle tumor, and STUMP. p16, a tumor suppressor gene, is expressed at high levels in aggressive tumors and is considered to be a useful marker of aggressive smooth muscle tumors. In addition, p53, p16, and Ki67 show higher expression in smooth muscle sarcoma than in STUMP.3
The prognosis of STUMP shows great inter-individual variation: most tumors grow slowly and have a favorable outcome, but there remains a risk of recurrence and malignancy. 14 According to a study by Iq et al., 15 4% to 27% of adequately managed STUMP lesions show malignant behavior, including recurrence and metastasis. Unlike typical leiomyosarcomas, STUMP lesions take longer to recur, and patients can survive for a long time, even after recurrence. Therefore, regular follow-up is essential, including annual imaging surveillance following hysterectomy. Furthermore, some authors recommend follow-up every 6 months during the first 5 years post-surgery, and annually during the subsequent 5 years.16,17
In conclusion, STUMP is a rare disease with the potential for recurrence and malignancy. Here, we have reported a case of STUMP encountered at our hospital and conducted a review of the literature, in which we have summarized the imaging characteristics of this condition. Although there have been some exceptions, the ultrasonographic characteristics of STUMP generally include the following: a solitary tumor, with well-defined margins, that shows iso- or mixed echogenicity and no acoustic shadowing, and demonstrates significant variation in peripheral and internal vascularization. The principal MRI features are as follows: >50% of the volume shows a strong signal on T2WI, there are small areas of strong signal on T1WI, and there are non-enhancing cystic areas after contrast enhancement. The accurate identification of these features can facilitate the early diagnosis of STUMP.
This case report was prepared to comply with the CARE guidelines. 18
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241279183 - Supplemental material for Imaging characteristics of uterine smooth muscle tumors of uncertain malignant potential: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605241279183 for Imaging characteristics of uterine smooth muscle tumors of uncertain malignant potential: a case report and literature review by Shuai Liu, Jing Chang, Wei Su, Hailian Lv, Bin Xu and Weiyi Gong in Journal of International Medical Research
Footnotes
Acknowledgements
The authors are grateful for the participation of the patient.
Author contributions
SL and JC produced the first draft of the manuscript and made substantial contributions to the editing and revision process. WS, HLL, and BX were significantly involved in manuscript writing and revision and contributed to figure production. WYG aided in the critical review of the manuscript prior to submission. All the authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
The study is a case report, and therefore the requirement for ethics approval was waived. We obtained the written consent of the patient for both treatment and publication.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.