
Abstract
We present the cases of two otherwise healthy adults, one with meningitis and another with a subdural abscess, with both conditions attributable to Streptococcus pneumoniae. A 31-year-old man was admitted with a 3-day history of fever, headache, and vomiting. Physical examination revealed intermittent confusion, irritability, and neck stiffness. Cerebrospinal fluid (CSF) culture was positive for S. pneumoniae. Contrast-enhanced magnetic resonance imaging (C-MRI) revealed multiple small lesions on the bilateral frontal lobes. Intravenous ceftriaxone and vancomycin were administered, followed by intravenous moxifloxacin. His symptoms resolved within 3 months. Additionally, a 66-year-old man was admitted for acute fever with confusion, abnormal behavior, and a recent history of acute respiratory infection. Physical examination revealed confusion, neck stiffness, and a positive right Babinski sign. CSF metagenomic analysis detected S. pneumoniae. C-MRI disclosed left occipitotemporal meningoencephalitis with subdural abscesses. Intravenous ceftriaxone was administered for 3 weeks. His condition gradually improved, with resorbed lesions detected on repeat MRI. This study expanded the clinical and imaging spectra of S. pneumoniae meningitis. In healthy adults, S. pneumoniae can invade the brain, but subdural abscess is a rare neuroimaging manifestation. Early diagnosis of S. pneumoniae meningitis by high-throughput sequencing and flexible treatment strategies are necessary for satisfactory outcomes.
Introduction
Community-acquired bacterial meningitis has an annual incidence of four to six cases per 100,000 adults, resulting in approximately 135,000 deaths worldwide annually. 1 Fifty-seven percent of bacterial meningitis cases are caused by Streptococcus pneumoniae. 2 S. pneumoniae meningitis is a deadly central nervous system (CNS) infection that results in severe and long-term neurological sequelae in almost 50% of survivors. 3 Despite access to effective antimicrobial therapy, the rates of post-infection sequelae and mortality remain high. 4 S. pneumoniae meningitis has a fatality rate ranging from 19% to 37%; 1 therefore, early diagnosis and effective treatment are important for reducing death and disability.
Most patients with S. pneumoniae meningitis are children,5,6 pregnant women,1,7 and patients with cerebrospinal fluid (CSF) leakage 8 or craniocerebral trauma. 9 Otopharyngeal infection, hematogenous spread, and cranial neurosurgery continue to be the predominant sources of pneumococcal CNS infection. In recent decades, only a few cases of pneumococcal brain abscesses have been described in adults. 10 Through protection by the blood–brain barrier (BBB), healthy adults rarely develop S. pneumoniae meningitis. 11 A subdural abscess may be caused by S. pneumoniae, but the underlying mechanism is not understood. In this study, we present two cases of S. pneumoniae meningitis with a literature review to improve our understanding and clinical management of this disease.
Case report
Case 1
In May 2018, a 31-year-old male patient presented with fever, headache, and vomiting for 3 days. He had no history of head or spine surgeries, cochlear implants, S. pneumoniae vaccination, toxic exposure, smoking, alcoholism, or drug abuse. His father had a history of cutaneous sarcoidosis.
Physical examination revealed blood pressure of 138/96 mmHg, intermittent confusion, irritability, neck stiffness, and mildly coarse breath sounds in the lungs. Multiple skin nodules were identified on the abdomen and face, possibly consistent with those reported in neurofibromatosis. Other systemic and neurological examination findings were normal.
Blood analysis was negative for syphilis, human immunodeficiency virus, and Mycobacterium tuberculosis antibodies. Negative results were reported for the Aspergillus antigen, (1,3)-β-
Laboratory findings for Case 1.
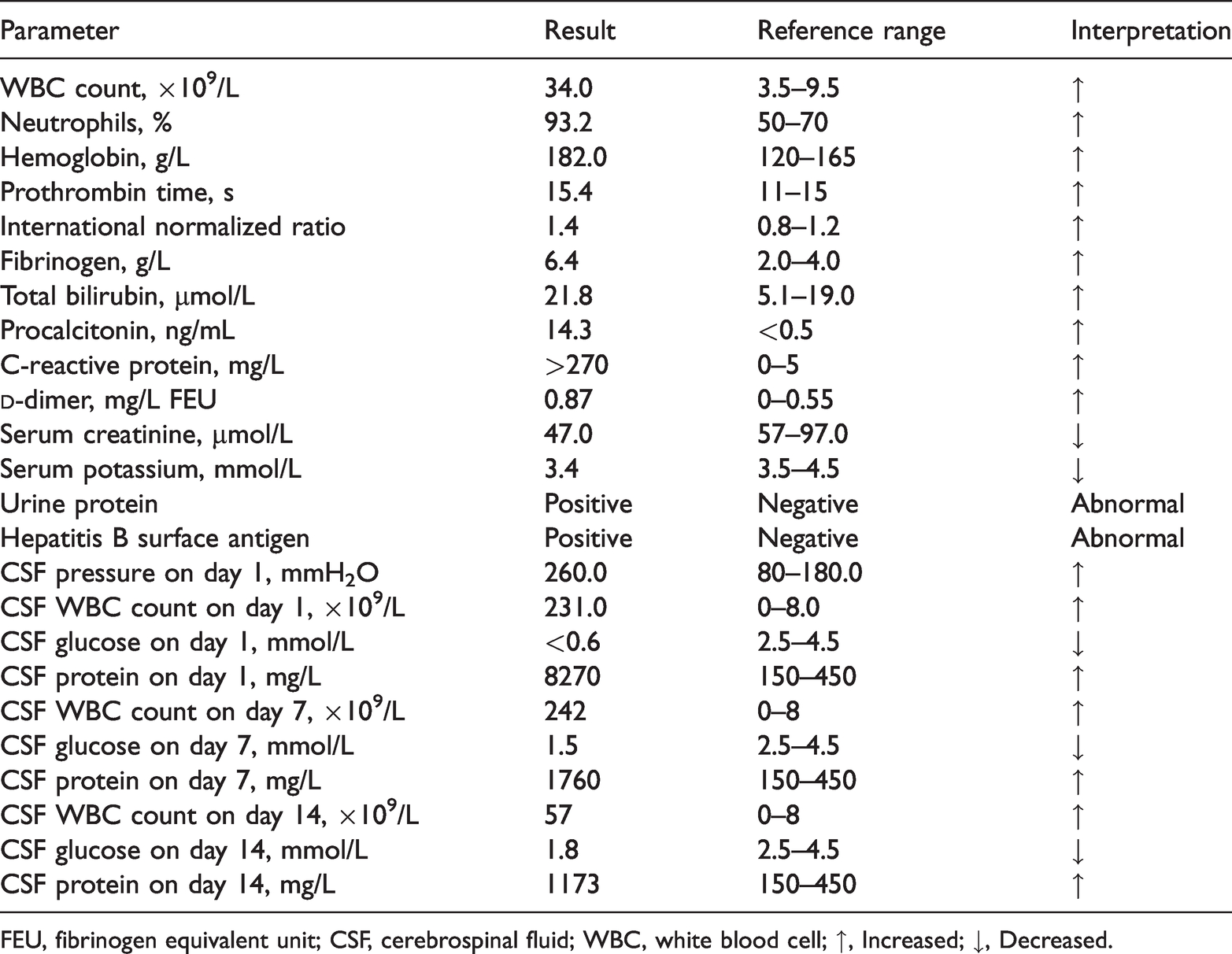
FEU, fibrinogen equivalent unit; CSF, cerebrospinal fluid; WBC, white blood cell; ↑, Increased; ↓, Decreased.
Electrocardiography, brain computed tomography (CT), ultrasonography of the urinary system, and echocardiography disclosed no obvious abnormalities. Abdominal ultrasonography revealed an accessory spleen, whereas chest CT revealed multiple inflammatory lesions in both lungs (Figure 1a). Contrast-enhanced magnetic resonance imaging (MRI) identified multiple small lesions of the bilateral frontal lobes (Figure 1b).
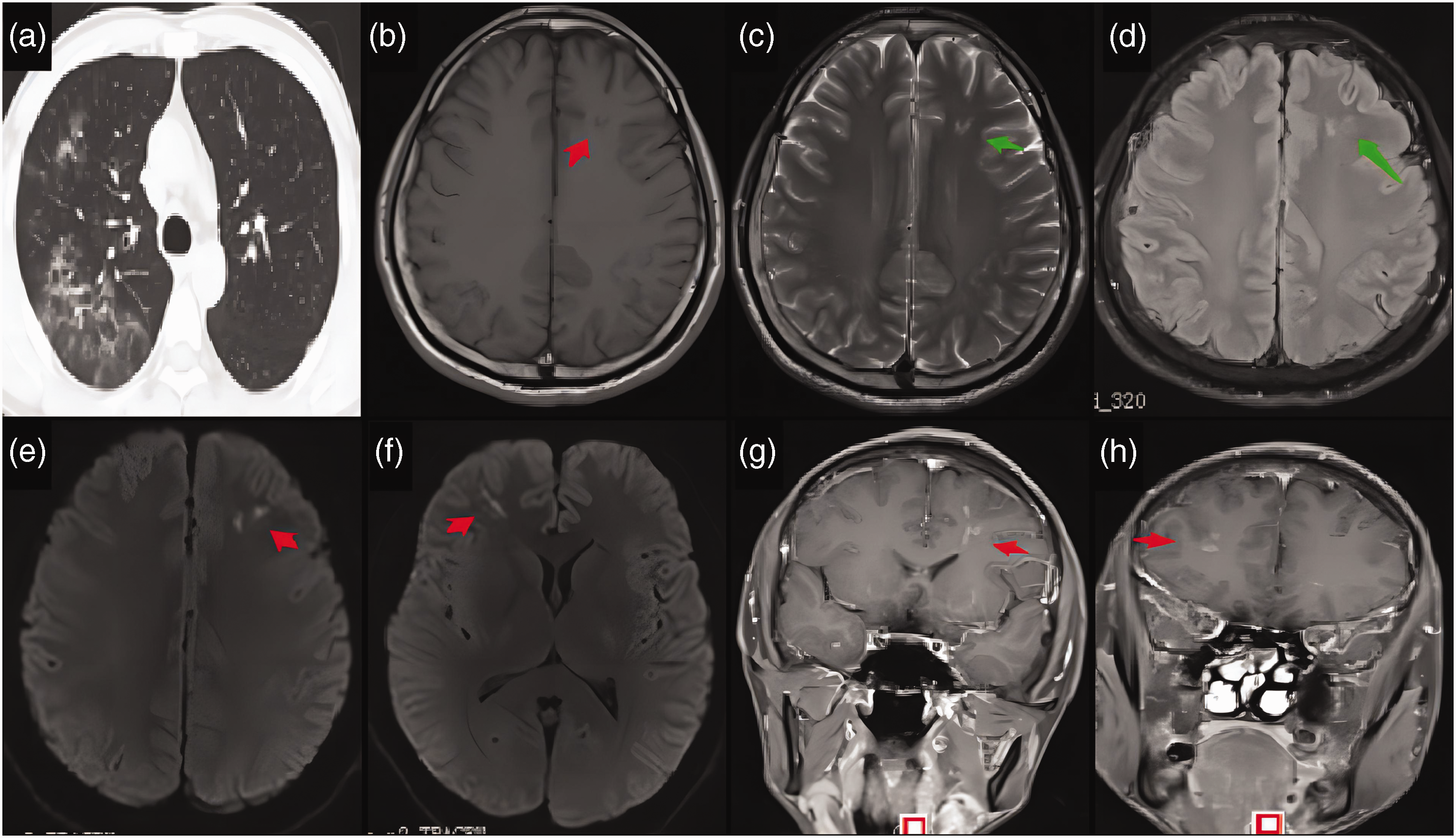
Manifestation of lesions on brain magnetic resonance imaging. (a) Chest computed tomography revealed multiple inflammatory lesions in both lungs. Brain magnetic resonance imaging revealed (b) hypointense punctate lesions (arrows) in the frontal lobe on axial T1-weighted imaging, (c) hyperintense lesions (arrows) in the bilateral frontal lobes on T2-weighted imaging, (d) fluid-attenuated inversion recovery, and (e, f) diffusion-weighted imaging and (g, h) The lesions were enhanced.
Intracranial infection was the initial diagnosis, and the patient was administered antibiotics (intravenous ceftriaxone for 3 weeks and vancomycin for 15 days simultaneously, followed by intravenous moxifloxacin for 2 weeks after the completion of intravenous vancomycin administration) and an antiviral agent (intravenous ganciclovir for 2 weeks). Intravenous mannitol was also administered to reduce intracranial pressure. Rehydration and symptomatic therapy were provided as needed. CSF cultures on days 7 and 14 were negative for bacteria and fungi. Cytologic examination of the CSF on day 14 revealed several segmented cells and lymphocytes. The patient’s symptoms were relieved while undergoing treatment, and his white blood cell (WBC) count and fibrinogen level normalized. He was discharged on day 29 without discomfort or positive neurological signs. At follow-up 3 months after discharge, he reported no discomfort.
Case 2
In December 2020, a 66-year-old male patient was admitted to our hospital with a chief complaint of fever for 1 day together with confusion and abnormal behavior for 2 hours. Ten days prior to admission, he had pharyngalgia and a cough producing yellow phlegm. Three days prior to admission, he developed pain and tinnitus in the left ear with purulent drainage from the external auditory canal. He consulted an otolaryngologist, who issued a diagnosis of acute secretory otitis media and myringitis. He had a several-year history of cerebral infarction, hypertension, type 2 diabetes mellitus, and facial neuritis. He had smoked for more than 10 years, but he had no history of head surgeries, toxic exposures, S. pneumoniae vaccination, or hereditary diseases.
Physical examination revealed an elevated body temperature of 39°C, bilateral coarse breath sounds with a few moist rales in the right middle and lower lobes of the lungs, hyperemia and yellow purulence in the external auditory canal, confusion, neck stiffness, and positive right Babinski and Gordon signs.
Blood analysis revealed normal serum creatinine, homocysteine, fungal (1,3)-β-
Laboratory findings for Case 2.

CSF, cerebrospinal fluid; WBC, white blood cell; ↑, Increased; ↓, Decreased.
No bacterial growth was detected in either of the two blood cultures. Sputum culture was positive for penicillin-resistant S. pneumoniae, whereas a culture of secretions from the external auditory canal was positive for Staphylococcus aureus. No pathogenic microorganisms were cultured from the CSF. However, metagenomic analysis of the CSF, which was performed at Guangzhou Oumeng Weiyi Medical Laboratory Co., Ltd. (Guangzhou, China), detected S. pneumoniae (221 sequence numbers, reference range: <8 sequence numbers). Chest CT revealed a few inflammatory changes in the middle lobe of the right lung. Brain CT demonstrated multiple lacunar infarcts with ischemic white matter injury. The initial brain MRI showed hypointensity on T1 (Figure 2a), slight hyperintensity on T2 and fluid-attenuated inversion recovery (FLAIR; Figure 2b–c), and hyperintensity on diffusion-weighted imaging (DWI; Figure 2d–e) in the left occipitotemporal lobes and left frontotemporal-parietal-occipital meningeal thickening with subdural abscess (Figure 2f–h). Electroencephalography revealed prominent slow-wave activity in the left temporal region, with a sharp wave and sharp-slow complex waves discharged in the left temporo-parietal-occipital region. Based on these findings, the diagnosis was S. pneumoniae meningitis with a subdural abscess.

Characteristics and evolution of lesions on brain magnetic resonance imaging. (a) Magnetic resonance imaging of the left occipitotemporal lobes revealed hypointensity on T1, (b, c) slight hyperintensity on T2 and fluid-attenuated inversion recovery (arrow), and (d, e) hyperintensity on diffusion-weighted imaging (arrow). There was also sulcal narrowing or disappearance in the left parietal-occipital cortex. The occipital-parietal-temporal-frontal meninges were thickened. (f–h) There were arc-shaped lesions with T1 hypointensity and T2 hyperintensity under the corresponding inner plate of the skull on contrast-enhanced magnetic resonance imaging (arrows). At 20 days after discharge, repeat magnetic resonance imaging revealed the disappearance of the hyperintensity on (i) diffusion-weighted imaging and (j) fluid-attenuated inversion recovery, and (k, l) the lesion was completely absorbed.
The patient was administered antibiotics (intravenous ceftriaxone 4 g per day for 3 weeks), an antiviral agent (intravenous ganciclovir for 4 days), and symptomatic treatment. Fever, cough, expectoration, and neck stiffness gradually improved. After 1 week, the patient was able to communicate normally. Repeat MRI on day 18 illustrated that the lesions had markedly improved. He was discharged on day 21 and prescribed oral levofloxacin (0.5 g per day for 2 weeks) at discharge. Twenty days after discharge, follow-up revealed that he had no discomfort, and a subsequent MRI illustrated the disappearance of the DWI and FLAIR hyperintensities (Figure 2i–j) and complete absorption of the subdural abscess (Figure 2k–l).
This study conforms to the CARE guidelines. 12
Discussion
In this study, we reported two exceptional cases of S. pneumoniae meningitis. One occurred in a healthy adult with a brain abscess, whereas the other patient presented with a subdural abscess. To our knowledge, reported cases such as these are sparse, and our reported cases have expanded our understanding of the clinical and imaging spectra of S. pneumoniae meningitis.
Susceptibility factors for S. pneumoniae
The most common foci of S. pneumoniae meningitis are the ears (30%), followed by the lungs (18%), sinus (8%), and other sites (2%), whereas the remaining cases (42%) involve cryptogenic brain abscesses. 13 Local extension from extracerebral infection is a common cause of S. pneumoniae meningitis. 1 Prior head or spine surgeries 11 associated with cochlear implants 14 also increase the risk for S. pneumoniae meningitis. Case 1 did not have the aforementioned risk factors, suggesting that even patients with S. pneumoniae and no obvious risk factors could have S. pneumoniae meningitis.
Case 2 had type 2 diabetes mellitus and otitis media, which may be predisposing factors for S. pneumoniae meningitis. Predisposing conditions, especially diabetes, are common among affected patients. 10 High blood glucose levels provide nutrition for the growth and reproduction of bacteria. Furthermore, they inhibit phagocytosis and sterilization by neutrophilic granulocytes, monocytes, and macrophages, ultimately reducing the body’s resistance to infection.15,16 In Case 2, identifying whether S. pneumoniae meningitis was caused by otitis media was necessary. Because sputum and external auditory canal secretion cultures tested positive for S. pneumoniae and S. aureus, respectively, we considered that Case 2 had S. pneumoniae meningitis associated with pulmonary infection.
Mechanism of intracranial invasion by S. pneumoniae
S. pneumoniae meningitis was considered to be related to an initial pulmonary infection in both patients. The specific mechanism by which S. pneumoniae enters the intracranial space through the BBB is unclear. The BBB is an important barrier to the CNS, and the destruction of BBB integrity is critical for intracranial infection caused by pathogenic microorganisms. Translocation across the BBB by S. pneumoniae is a crucial early step in the pathogenesis of meningitis. 3 For bacteria to pass through the BBB, the following conditions are required: a continuously high degree of bacteremia, bacterial adhesion and aggregation, and activation of related signal transduction pathways. 17
Pathogens adhere to the surface of microvascular endothelial cells, and they can release virulence factors that destroy the tight junctions between brain capillary endothelial cells. Alternatively, these pathogens can directly enter endothelial cells through endocytosis, which increases the permeability of the BBB and facilitates the entry of pathogens into the brain. S. pneumoniae colonizes the host respiratory mucosal epithelium, invades the bloodstream, multiplies, crosses the BBB, and proliferates in the CSF. 19 Studying the signal transduction pathway of pathogenic bacteria has great significance for the prevention and treatment of CNS infections. Through a study of meningitis models derived from bacteremia, Iovino et al. found that antibodies against polymeric immunoglobulin receptors and platelet endothelial cell adhesion molecule-1 receptors can prevent S. pneumoniae from entering the brain and thus prevent the development of meningitis. 20
Case 2 had acute secretory otitis media and myringitis. Previous evidence indicated that otitis media caused by S. pneumoniae can spread to the CNS and cause meningitis by bypassing the bloodstream. Hence, we speculated that S. pneumonia in the otitis media bypassed the bloodstream, invaded the ipsilateral cerebral cortex, and further involved the meninges to form parameningeal foci. In fact, S. pneumoniae is the leading cause of otitis media; 21 however, another interpretation is that early lumbar puncture (on day 2) and the early use of antibiotics resulted in culture-negative results. 22 The initial negative CSF culture in Case 2 could not exclude S. pneumoniae invasion into the CNS. 23 Metagenomic analysis of the CSF finally detected S. pneumoniae; therefore, S. pneumoniae in respiratory infection entering the CNS through the blood circulation could not be completely dismissed.
Clinical features
On admission, fever and an altered mental status are the most frequent findings (in 93% and 94% of cases, respectively), whereas back rigidity, headache, and seizures are found in 57%, 41%, and 11% of cases, respectively. 13 The most common symptoms of S. pneumoniae meningitis in the elderly are fever, headache, and vomiting, accompanied by coma, neck rigidity, and positive Kernig’s and Babinski signs. 24 Both cases had fever, headache, confusion, and seizures, which are common symptoms as previously mentioned. Acute urinary retention24,25 and diabetes insipidus 26 can occasionally occur secondary to pneumococcal meningitis.
Intracranial subdural abscess is a rare condition, accounting for 15% to 20% of localized intracranial infections.27,28 Case 2 had an S. pneumoniae subdural abscess, which has expanded our understanding of the imaging spectrum of S. pneumoniae meningitis. To our knowledge, reports on similar cases are lacking. An intracranial subdural abscess is a loculated collection of pus in the subdural space between the dura mater and arachnoid. 29 After S. pneumoniae invades the brain, it produces large amounts of fibrin and inflammatory exudates on the surface of the brain, which can quickly result in tissue adhesion and encapsulated abscesses. 30 Because the subdural space is continuous and has no anatomic barrier, subdural abscesses can spread over the convexity of the brain between both cerebral hemispheres, and extensive subdural abscesses were also detected in Case 2. In addition, subdural abscesses are considered a dangerous but treatable entity, and prompt diagnosis and adequate treatment can result in better outcomes. 29 Interestingly, there have been reports of spinal epidural abscess 6 caused by S. pneumoniae.
CSF analysis and culture are crucial for diagnosing S. pneumoniae meningitis. Typical findings of low glucose levels, elevated protein levels, and pleocytosis with polymorphonuclear cell predominance are characteristic of S. pneumoniae meningitis. 4 These features were present in Case 1. However, Case 2 had diabetes mellitus; therefore, it was difficult to verify low glucose levels in the CSF. Findings such as low glucose and high protein levels should alert the clinician to the possibility of bacterial meningitis, and empirical antimicrobial therapy should be considered. However, there is a previously reported case of a patient with pneumococcal meningitis without CSF pleocytosis. 22 Whole-genome sequencing for identifying pathogens in the CSF played a key role in the diagnosis of Case 2. In addition, the polymerase chain reaction-based assay for amplification of the pneumolysin gene proved useful in the identification of S. pneumoniae. 31
Treatment and prognosis
Third-generation cephalosporins are the antibiotics of choice for the treatment of S. pneumoniae meningitis. 32 Ceftriaxone treatment in Case 2 led to good results. Intravenous ceftriaxone and vancomycin were administered to Case 1 based on the drug sensitivity results, and a good treatment effect was initially achieved. However, the patient presented with recurrent fever and an appreciably increased blood WBC count 2 weeks later. Based on the possibility of S. pneumoniae resistance to antibiotics, we empirically replaced vancomycin with moxifloxacin given that moxifloxacin is a second-line treatment for bacterial encephalitis.33,34 Subsequently, the fever resolved, and the WBC count returned to normal. With the worldwide increase in the prevalence of penicillin-resistant pneumococci, combination therapy with vancomycin plus a third-generation cephalosporin has become the standard approach for empirical antimicrobial therapy.35,36 The emergence of resistant strains might create a therapeutic challenge in the future, and there are already penicillin- and cephalosporin-resistant strains of S. pneumoniae. 35 Vancomycin plus levofloxacin could be a treatment option for bacterial meningitis attributable to penicillin- and third-generation cephalosporin-resistant strains of S. pneumoniae. 37 The combined use of meropenem, ceftriaxone, and vancomycin has been reportedly successful in the treatment of S. pneumoniae meningitis. 38 Based on our experience, the timely adjustment of antibiotics according to the treatment effect and based on the results of drug sensitivity tests is essential. The choice of appropriate antibiotics should be made according to the in vitro antimicrobial susceptibilities and careful monitoring of the therapeutic effect.
Previous evidence indicated that dexamethasone treatment is associated with lower mortality in adults and fewer neurological and auditory sequelae in adults and children from high-income countries, particularly in adults suffering from pneumococcal meningitis. By contrast, studies conducted in developing countries yielded less favorable results. 39 Previous findings support the use of corticosteroids for patients with bacterial meningitis in high-income countries. Conversely, there was no beneficial effect of corticosteroid therapy in low-income countries. 40 China remains a developing country, and the expert consensus in China does not explicitly recommend the use of dexamethasone for improving neurological sequelae. 41 In addition, our patients responded well to the treatment. Hence, we did not actively use dexamethasone.
Few S. pneumoniae brain abscesses require surgery. S. pneumoniae meningitis has a high mortality rate if left untreated. 42 In patients who survive the initial insult, neurologic sequelae, including seizures, hearing loss, and impaired mental status and/or cognition, may occur in as many as 30% of cases. 36 The independent prognostic factor associated with fatal outcomes was seizures, whereas the presence of an otogenic focus was independently associated with improved survival. 13 Both patients in this report were satisfied with the treatment received and their recovery.
The mechanism by which S. pneumoniae passed the BBB and caused meningitis in Case 1 is unclear. Further research using humanized animal models to study the mechanism of the penetration of pathogenic bacteria through the BBB must be conducted.
In conclusion, this study expands the clinical and imaging spectra of S. pneumoniae meningitis. Clinicians must recognize that even in healthy adults without predisposing factors, S. pneumoniae can invade the brain. Additionally, subdural abscess of the brain is a rare neuroimaging finding in S. pneumoniae meningitis. Early diagnosis by high-throughput sequencing, close observation of the therapeutic effect of antibiotics, and flexible treatment strategies are critical for achieving a good outcome. Further study of the mechanisms by which S. pneumoniae passes through the BBB is necessary to develop targeted interventions.
Research Data
Research Data for Healthy adults with Streptococcus pneumoniae meningitis and Streptococcus pneumoniae subdural abscess: two case reports and a literature review
Research Data for Healthy adults with Streptococcus pneumoniae meningitis and Streptococcus pneumoniae subdural abscess: two case reports and a literature review by Fanxin Kong, Liling Li, Daxue Zhang, Baorong Lian, Xudong Liu, Shuqun Ren, Yu Zhang, Liming Cao in Journal of International Medical Research
Footnotes
Author contributions
FK, LL, and DZ were responsible for data collection and writing of the first draft. BL, XL, SR, and YZ provided constructive discussion and translated the manuscript. LC conceived the study and translated and critically revised the manuscript. All authors have read and approved the manuscript.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The study was approved by the ethics review board of the First Affiliated Hospital of Shenzhen University (No. 202204133006, approval date: 5 May 2022). We obtained informed consent for treatment from both patients and written consent to publish these findings.
Funding
The authors disclosed receipt (pending publication) of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shenzhen Medicine and Hygiene Sanming Project (No. SZZYSM202111011), Guangdong Administration of Traditional Chinese Medicine Project (No. 20221357), Shenzhen Second People’s Hospital Clinical Research Fund of Guangdong Province High-level Hospital Construction Project (No. 20223357021), Research Project of Teaching Reform in Shenzhen Second People’s Hospital (No. 202209), “3030 project” of Clinical Research Program in Shenzhen Traditional Chinese Medicine Hospital in 2021 [No. G3030202132], and Teaching Quality and Teaching Reform Project in Guangzhou University of Traditional Chinese Medicine in 2021 [No. 84]).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.