
Abstract
Objective
To systematically evaluate potential risk factors for tracheal stenosis and to provide a reference for the prevention and management of patients with this condition.
Methods
Databases were searched to identify studies of the risk factors for tracheal stenosis, from their inception to October 2023, then a meta-analysis was performed. The study was registered with PROSPERO under the registration number CRD42023428906.
Results
Ten studies of a total of 2525 patients were included. The meta-analysis showed that tracheotomy, diabetes, the duration of intubation, the duration of mechanical ventilation, respiratory tract infection, a high incision, and a ratio of intratracheal tube cuff diameter (C)/transverse diameter at the level of the clavicle (T) >150% were risk factors for the development of tracheal stenosis.
Conclusion
Measures such as shortening the duration of mechanical ventilation and intubation, reducing and avoiding tracheotomy after prolonged intubation, early tracheotomy in patients with obesity who require prolonged mechanical ventilation, appropriate choices of incision location and catheter, the maintenance of appropriate C/T, the prevention of respiratory infection, and the control of diabetes mellitus should limit the risk of tracheal stenosis.
Keywords
Introduction
Tracheal stenosis, a common respiratory condition, is often caused by tumour or tuberculosis, or is a complication of intubation or incision. 1 Because of more frequent intubation and incision and higher tumour incidence, 2 the incidence of airway stenosis has increased in recent years.3–5 Airway stenosis refers to narrowing of the trachea, the main bronchi and their distal branches. 6 Stenosis can be benign or malignant, depending on the characteristics of the lesion. 6 The reported incidence of post-tracheotomy/intubation stenosis ranges from 0.6% to 21%.7,8 Local factors, such as airway trauma from tube contact, poor cuff pressure control, poor technique and infection can contribute to the aetiology of stenosis. 7 In addition, systemic factors, such as cardiovascular disease and metabolic conditions, may also lead to tracheal wall damage and stenosis. 7 Other less common causes include trauma, autoimmune diseases, congenital abnormalities and neoplasms.7–9
Tracheal stenosis often leads to respiratory distress, which greatly impairs quality of life. Furthermore, it can be a life-threatening condition if severe. The early diagnosis of the condition and the identification of at-risk groups should facilitate the development of preventive and treatment measures, which are critical for patient outcomes. However, the aetiology of the condition remains unclear and previous studies have generated inconsistent findings in this regard. Therefore, in the present study, we aimed to systematically evaluate potential risk factors for tracheal stenosis, to inform the prevention and management of this condition.
Recent reviews have proposed measures such as the use of endotracheal tubes with protective layers and appropriate cuff-pressure monitoring to prevent stenosis. However, large-scale clinical trials have not been performed to confirm the efficacy of this approach. The novel of the present study lies in the use of a large amount of clinical data and a prospective approach to systematically identify independent risk factors. The findings should help guide the design of prevention and treatment strategies for this condition.
Patients and methods
Search strategy and selection criteria
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we conducted a systematic review of studies of tracheal stenosis. 10 The study was registered with PROSPERO under the registration number CRD42023428906, but post-registration, the Population, Intervention, Comparison, Outcomes and Study criteria, data extraction and quality assessment have been slightly modified. We conducted a systematic review of PubMed (US National Library of Medicine, National Institutes of Health), Scopus (Elsevier), EBSCOhost, CNKI, WanFang Data, VIP, Ovid and the Cochrane Library using a defined search strategy. A combination of subject headings (e.g., MeSH in PubMed) and keywords related to ‘‘Tracheal stenosis,’’ and ‘‘Risk factor,’’ was used. The PubMed search strategy was reformatted for the other databases, while maintaining similar keywords and replacing MeSH terms with appropriate subject headings when available.
The databases were searched from their inception to 21 October 2023. The inclusion criteria for studies were that they included patients undergoing tracheoscopy, that they were cohort studies or case–control studies, that the exposure factors may be risk factors for tracheal stenosis and that the outcome was a clinically or imaging-confirmed diagnosis of tracheal stenosis. The exclusion criteria were duplicate studies, publications in neither Chinese nor English, lack of information regarding the methods, poor reliability, poor quality and a lack of raw data for inclusion in a meta-analysis. We allocated patients with tracheal stenosis to an observation group and those without to a control group.
Data extraction
Data were extracted independently by two investigators, entered into an Excel (Microsoft Corp., Redmond, WA, USA) spreadsheet and any discrepancies were resolved through discussion with a third investigator. For each study, the following data were collected: first author, country, year of publication, sample size, study design, risk factors for tracheal stenosis and specific data. Risk-of-bias evaluations for the included studies were evaluated independently by two investigators and the results obtained were cross-checked. Case–control and cohort studies were evaluated using the Newcastle–Ottawa scale (NOS).
Data synthesis and statistical analysis
Statistical analysis was performed using RevMan v.5.2 (New York, NY, USA). Odds ratios (ORs) and the corresponding 95% confidence intervals (CIs) were calculated for each potential risk factor. The heterogeneity of the included studies was analysed using the χ2 test (test level α = 0.1), and the magnitude of heterogeneity was determined quantitatively using I2. If I2 was <50%, a fixed-effects model was used and if it was ≥50%, a random-effects model was used. Heterogeneity was defined as low, medium or high when I2 was <25%, 25% < I2 < 50% or I2 > 50%, respectively. 11 If there was heterogeneity, subgroup analyses of the outcomes were performed, with I2 > 50% and P < 0.1 being taken to indicate heterogeneity of the data across multiple studies, and I2 ≤ 50% and P ≥ 0.1 indicating good homogeneity. Significant clinical heterogeneity was dealt with by performing subgroup or sensitivity analyses, or by using descriptive analysis only. Subgroup analyses were performed according to the defined risk factors: tracheotomy, diabetes, obesity, duration of intubation, duration of mechanical ventilation, respiratory tract infection, high incision and C/T > 150%.
Results
A total of 4847 publications were identified in the initial search, and 10 studies of 2525 patients remained after stratification screening. The literature screening process and results are shown in Figure 1. The basic characteristics of the included studies are shown in Table 1, and the results of the risk-of-bias evaluation of the included case–control and cohort studies are shown in Table 2 and Table 3, respectively.

Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram of study selection.
Basic characteristics of the included studies.

Classification of risk factors: ① tracheotomy, ② obesity, ③ diabetes, ④ duration of intubation, ⑤ duration of mechanical ventilation, ⑥ respiratory tract infection, ⑦ position of incision too high, ⑧ ratio of intratracheal tube cuff diameter/transverse diameter at the level of the clavicle > 150%.
Results of the risk of bias evaluation for the included case–control studies (points).

(1) Appropriateness of the definition and diagnosis made. (2) Representativeness of the patients. (3) Selection of controls. (4) Definition of contrast. (5) Comparability of cases and controls. (6) Methods of investigation and assessment of exposure. (7) Methods used to identify exposure factors for cases and controls. (8) Non-response rate.
Results of the risk of bias evaluation for the included cohort studies (points).
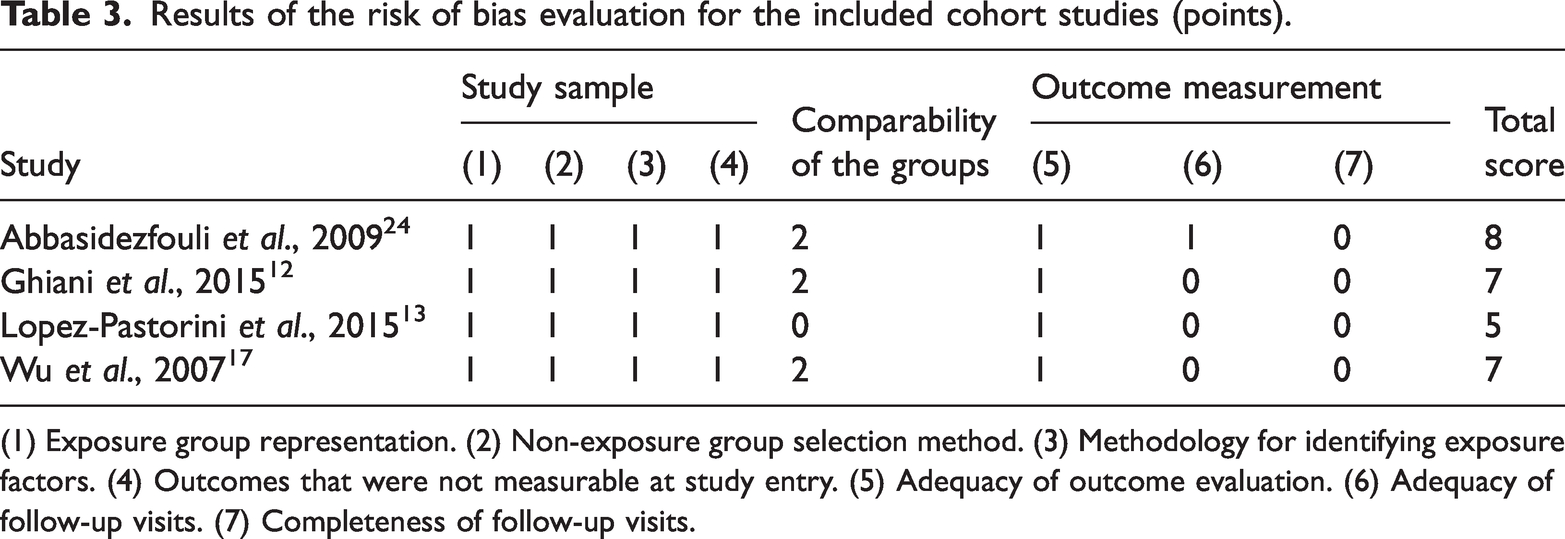
(1) Exposure group representation. (2) Non-exposure group selection method. (3) Methodology for identifying exposure factors. (4) Outcomes that were not measurable at study entry. (5) Adequacy of outcome evaluation. (6) Adequacy of follow-up visits. (7) Completeness of follow-up visits.
The meta-analysis revealed that tracheotomy (OR = 1.99, 95% CI 1.20–3.30 P = 0.008), diabetes (OR = 3.54, 95% CI 1.76–7.10, P = 0.0004), obesity (OR = 3.06, 95% CI 1.17–8.04, P = 0.02), the duration of intubation (OR = 5.39, 95% CI 2.22–13.09, P = 0.0002), the duration of mechanical ventilation (OR = 8.53, 95% CI 4.89–14.91, P < 0.00001), respiratory infection (OR = 5.42, 95% CI 3.87–7.59, P < 0.00001), a too-high incision (OR = 7.08, 95% CI 1.71–29.41, P = 0.007) and C/T > 150% (OR = 2.02, 95% CI 1.20–3.41, P = 0.008) were all risk factors for the development of tracheal stenosis (Table 4).
Results of the meta-analysis.
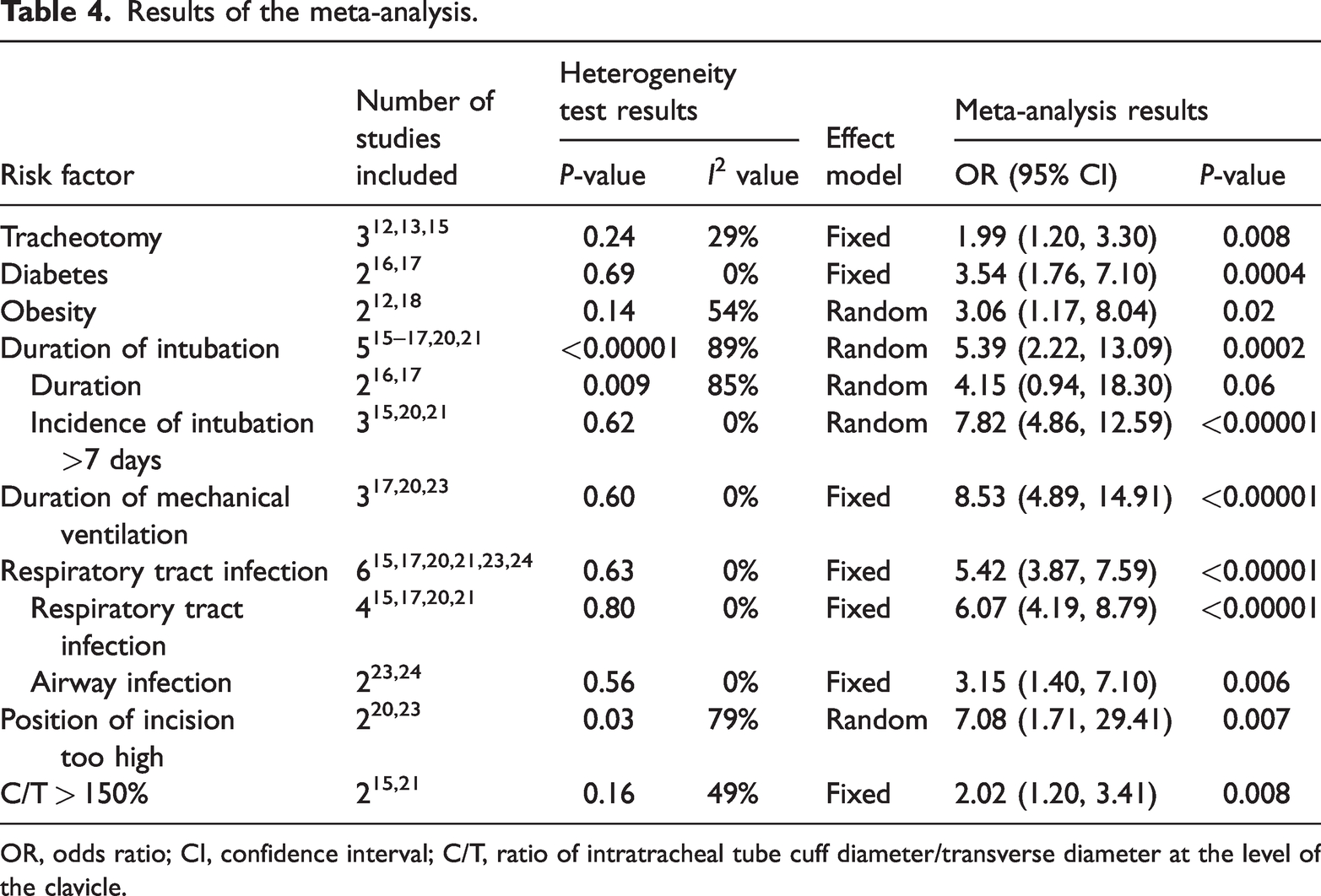
OR, odds ratio; CI, confidence interval; C/T, ratio of intratracheal tube cuff diameter/transverse diameter at the level of the clavicle.
Tracheotomy
Four papers12–15 mentioned the effect of tracheotomy on the incidence of tracheal stenosis in patients. However, because some patients with laryngeal stenosis were included in the article by Lukáš et al., 14 this was excluded, and therefore three studies were finally included. The data were not heterogeneous (I2 = 29%, P = 0.24), and therefore a fixed-effects model was used, and the meta-analysis revealed an OR of 1.99 [95% CI 1.20–3.30, P = 0.008] and a significant association of tracheotomy with stenosis (Figure 2(a)).

Forest plot of risk factors for tracheal stenosis. (a) Effect of tracheotomy on the risk of tracheal stenosis. (b) Effect of diabetes on the risk of tracheal stenosis. (c) Effect of obesity on the risk of tracheal stenosis and (d) effect of intubation time on the risk of tracheal stenosis.
Diabetes mellitus
Two papers16,17 mentioned the effect of diabetes on the incidence of tracheal stenosis in patients, The data were found not to be heterogeneous (I2 = 0%, P = 0.69), and therefore a fixed-effects model was used. An OR of 3.54 was calculated [95% CI 1.76–7.10, P = 0.0004], and there was a statistically significant association between diabetes and tracheal stenosis (Figure 2(b)).
Obesity
Two papers12,18 mentioned the effect of obesity on the incidence of tracheal stenosis in patients. Moderate heterogeneity was identified (I2 = 54%, P = 0.14), and therefore a random-effects model was used. An OR of 3.06 was obtained [95% CI 1.17–8.04, P = 0.02], and the meta-analysis showed a statistically significant association between obesity and tracheal stenosis (Figure 2(c)).
Intubation time
Six papers15–17,19–21 mentioned the effect of intubation time on the incidence of tracheal stenosis in patients, but in one of these 19 , it was mentioned in the text that the measurement was not rigorous and that there may have been patients with laryngotracheal stenosis in the control group. In addition, the follow-up attrition and treatment outcomes were influenced by chronic obstructive pulmonary disease. Therefore, data from five articles were included in the analysis. Significant heterogeneity was identified (I2 = 89%, P < 0.00001), and an OR of 5.39 (95% CI 2.22–13.09) was obtained using a random effects model. The meta-analysis showed that the association between intubation time and tracheal stenosis was statistically significant. Two of the studies16,17 showed an effect of long intubation time on tracheal stenosis, with a combined OR of 4.15 (95% CI 0.94–18.30), but there was heterogeneity between the studies (I2 = 85%, P = 0.009). The other three studies15,20,21 showed an effect of a duration of intubation of >7 days on the incidence of tracheal stenosis, with a combined OR of 7.82 (95% CI 4.86–12.59) and no significant heterogeneity (I2 = 0%, P = 0.62). Thus, the duration of intubation was a significant risk factor for tracheal stenosis (Figure 2(d)).
Duration of mechanical ventilation
Four papers17,20,22,23 mentioned the effect of the duration of mechanical ventilation on the incidence of tracheal stenosis in patients. However, Hang et al. 22 included patients with central airway stenosis, and the inclusion of patients with supraglottic stenosis was not fully compatible with the inclusion criteria of the present analysis; therefore, this study was excluded and the data from the other three studies were studied. An OR of 8.53 was obtained (95% CI 4.89–14.91) using a fixed-effect model, because heterogeneity testing showed that the data were homogeneous (I2 = 0%, P = 0.60). Thus, the meta-analysis showed that there was a significant association between the duration of mechanical ventilation and tracheal stenosis, and this represented a substantial risk for tracheal stenosis (Figure 3(a)).
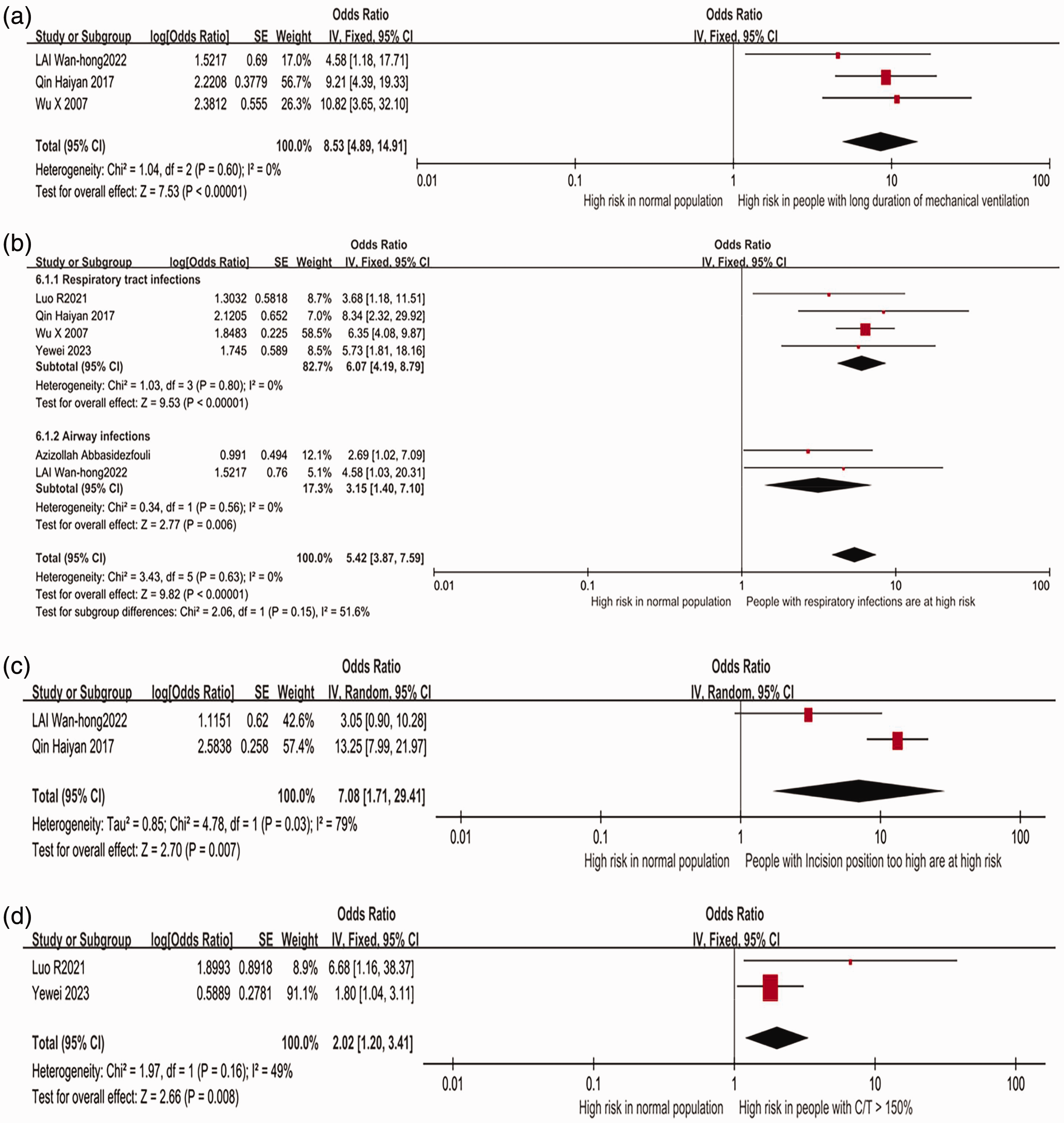
Forest plot of additional risk factors for tracheal stenosis. (a) Effect of the duration of mechanical ventilation on the risk of tracheal stenosis. (b) Effect of respiratory tract infection on the risk of tracheal stenosis. (c) Effect of a too-high incision on the risk of tracheal stenosis and (d) effect of ratio of intratracheal tube cuff diameter/transverse diameter at the level of the clavicle >150% on the risk of tracheal stenosis.
Respiratory infections
Six papers15,17,20,21,23,24 mentioned the effect of respiratory tract infection on the incidence of tracheal stenosis. Heterogeneity testing indicated homogeneity of the data (I2 = 0%, P = 0.63), and an OR of 5.42 (95% CI 3.87–7.59) was obtained using a fixed-effects model. Thus, the meta-analysis showed that there was a significant association between respiratory tract infection and tracheal stenosis. Four of the studies15,17,20,21 mentioned the effect of respiratory tract infection on tracheal stenosis, and the combined OR for these data was 6.07 (95% 4.19–8.79], with no significant heterogeneity in the data (I2 = 0%, P < 0.00001). The two other studies23,24 showed an effect of airway infection on tracheal stenosis, and there was a combined OR of 3.15 (95% 1.40–7.10), with no significant heterogeneity in the data (I2 = 0%, P = 0.0006). Thus, respiratory infection was a substantial risk factor for the development of tracheal stenosis (Figure 3(b)).
Too-high incision position
Two papers20,23 mentioned the effect of an incision that was too high on the incidence of tracheal stenosis. The studies showed significant heterogeneity (I2 = 79%, P = 0.007), and a random-effects model yielded an OR of 7.08 (95% CI 1.71–29.41). In the study by Wan-Hong et al. 23 , the incision position was too high, above the second cartilage ring, while Haiyan et al. 20 did not specify the exact position of the incision, but she quoted Chunyan et al. 25 in their discussion, pointing out that tracheotomy is usually performed between the second and third or third and fourth cartilage rings, and that if the surgical site is too high, damage is caused to the first tracheal cartilage ring, resulting in tracheal tenderness and stenosis. The meta-analysis showed that a too-high incision was a risk factor for tracheal stenosis (Figure 3(c)).
Intratracheal tube cuff diameter/transverse diameter at the level of the clavicle ratio >150%
Two papers15,21 mentioned the effect of C/T > 150% on the incidence of tracheal stenosis. There was significant heterogeneity of the data (I2 = 49%, P = 0.16), and a fixed-effects model yielded an OR of 2.02 (95% CI 1.20–3.41). Thus, the meta-analysis showed a statistically significant association between C/T > 150% and tracheal stenosis (Figure 3(d)).
Results of the descriptive analysis
Six papers studied whether age is a risk factor for tracheal stenosis, but owing to the different inclusion and stratification criteria used in these studies, the patients could not be stratified by age for a combined analysis. For example, the study by Wu et al. appeared to meet the nadir criteria, but the diagnostic criteria regarding tracheal stenosis were missing, and only the diagnostic criteria for bronchial stenosis were available. Qin et al. and 20 Wu et al. 25 found that age ≥60 years was a risk factor for tracheal stenosis after tracheotomy. However, the study by Wu et al. was not included in the combined analyses because the inclusion criteria differed from those of the present study. Kanlikama et al. and 26 Samuel et al., 27 found that age <30 years was the only risk factor for recurrent tracheal stenosis, whereas Um et al. 28 found that age >45 years was an independent predictor of persistent tracheal stenosis. Finally, Koizumi et al. 29 found that younger age and prolonged tracheostomy tube placement were associated with peristomal granulation.
The endotracheal tube size was considered to be a potential risk factor for tracheal stenosis, but this could not be analysed because of differences in the criteria used in the studies. Elkerbout et al. 30 found that the intubation tube diameter had an effect on tracheal stenosis, and that with the use of appropriate intubation tubes, the incidence of acquired tracheal stenosis was lower. 31 In addition, Li et al. 18 stated that the size of the tracheostomy tube was a potential risk factor. Hui et al. 32 found that laryngotracheal stenosis is more likely to occur after tracheotomy, especially in younger people because they have a soft trachea, and a tracheotomy that is too small or the use of too large a tracheostomy tube can cause the trachea to collapse or cause damage to the tracheal mucosa, resulting in granulomatous hyperplasia, ischemia, necrosis, infection and scarring, resulting in stenosis.
Underweight is also considered to be a risk factor for tracheal stenosis, but this could not be analysed in the present study, because of incomplete data in the reports and differences in study design. Koizumi et al. 29 concluded that underweight (body mass index <18.5 kg/m) was significantly associated with the incidence of tracheostomy-related stenosis, and Elkerbout et al. 30 concluded that low birth weight (<1500 g) was a significant risk factor.
Sensitivity analysis and evaluation of publication bias
Sensitivity analysis was performed using a study-by-study exclusion approach and showed that the ORs after each exclusion did not substantially differ from the initial results, suggesting that the results of the present study were robust. In the sensitivity analysis of the effect of the duration of intubation, the combined OR (95% CI) became 2.22 (2.07–2.37) (P < 0.00001) when one of the papers 19 was excluded. This finding was quite different from that obtained in the initial meta-analysis. Owing to the small number of studies included for each outcome, no test of publication bias was performed.
Discussion
Data from a total of six case–control studies and four cohort studies of largely older patients who had undergone tracheal intubation were included in the present study. We aimed to identify risk factors for the development of tracheal stenosis in older patients after intubation. We identified multiple risk factors, and these findings may help inform patients regarding their prognosis. These risk factors were tracheotomy, obesity, diabetes, the duration of intubation, the duration of mechanical ventilation, respiratory tract infection, a too-high position of the incision, and a C/T > 150%.
The invasion or metastasis of malignant tumours or external pressure on the airway of another aetiology may cause narrowing of the tracheal lumen, leading to malignant tracheal stenosis. 33 Compression of the trachea and the resulting dyspnoea may be caused by the tumour itself or degenerative necrosis of the tracheal cartilage. 34 The studies by Rou et al., 15 Songu et al. 16 and Wei et al. 21 excluded malignant tracheal stenosis caused by tumours, whereas those by Ghiani et al. 12 and Haiyan et al. 20 included a small number of patients with tumours, but the results showed that tumour was not a risk factor. The study by Wan-Hong et al. 23 did not determine whether or not tumour was a risk factor, and Wu et al. 17 and Abbasidezfouli et al. 24 did not mention whether patients with tumours were included or not and the issue was not discussed. As a consequence of the small number of such patients included in these studies, malignant tracheal stenosis caused by tumours was not explored in depth in the present study.
It has been shown 28 that an age of >45 years is an independent predictor of persistent bronchial stenosis, but it is unclear how age would influence bronchial stenosis. Although there are published findings demonstrating a higher incidence of restenosis in patients of <17 years, there is no obvious explanation for this. 27 Furthermore, the study by Jianjun et al. 35 showed that age >75 years is a risk factor for airway stenosis after percutaneous dilatation tracheostomy. Thus, the various studies of this issue have yielded inconsistent results and no firm conclusions can be drawn.
In the present study, we have shown that tracheotomy, the duration of intubation and the duration of mechanical ventilation are risk factors for tracheal stenosis. A common cause of airway stenosis is trauma or inflammation, and the performance of multiple tracheotomies causes substantial mechanical injury to the trachea. The resulting mucosal inflammation has a deleterious effect on the mucociliary layer, and prolonged inflammation leads to mucosal oedema, necrosis or softening of the cartilage, ciliated cell apoptosis, mucosal epithelial metaplasia and the proliferation of granulation tissue, leading to tracheal stenosis. 17 Accidental injury to the cricoid cartilage during cricothyrotomy or prolonged compression of the cricoid cartilage by the trocar after cricothyrotomy increases the probability of subsequent laryngotracheal stenosis. 17 When the stenosis is extensive and necessitate substantial excision, it may be difficult to remobilise the trachea. 36 However, because it is a multifactorial condition, some patients with stenosis may have to undergo tracheotomy, which may relieve the symptoms of the stenosis. Esteller-Moré et al. 37 stated that tracheotomy after prolonged intubation should be avoided, and that it must be performed promptly in patients who have a poor general condition and in those admitted because of non-surgical and non-neurological conditions. In addition, Li et al. 18 showed that early tracheotomy reduces the incidence of ventilator-associated pneumonia and shortens the stay of patients in the intensive care unit and the duration of mechanical ventilation.
A consensus is developing regarding the negative effects of prolonged intubation followed by tracheotomy. The Laryngotracheal Stenosis Committee of the European Laryngological Society stated that prolonged tracheal intubation and delayed tracheotomy may increase the risk of post-intubation laryngotracheal stenosis in patients with COVID-19.38,39 In addition, a previous study showed 37 that the development of injury is more likely to be influenced by the duration of intubation than by the tracheotomy itself. We believe that it is advisable to avoid delaying tracheotomy after intubation: it should be performed promptly, especially in patients in poor general condition and in those admitted because non-neurological and non-surgical conditions. Esteller-Moré et al. 37 found that the longer the duration of intubation before tracheotomy, the more likely it is that tracheal stenosis will occur. This may be because prolonged intubation causes compression of the tracheal wall and mucosal damage, which is further exacerbated by tracheotomy, and leads to tracheal stenosis. 17
There is still considerable controversy regarding the importance of the duration of intubation with respect to the risk of tracheal stenosis. A previous study 40 has shown that laryngeal changes, such as oedema and mucosal ulceration, can occur within the first few hours of intubation. However, these sequelae usually resolve spontaneously in most patients, without additional clinical symptoms developing. Another study 16 has shown that patients who are intubated for >48 hours are significantly more likely to develop stenosis than those who are not. Furthermore, it has been shown 17 that intubation for >7 days results in post-intubation tracheal injury in 94.5% of patients and significant injury resulting in tracheal stenosis in 9%. Consistent with this, we have shown that intubation for >7 days is associated with a significantly higher risk of stenosis. Papuzinski et al. 41 found that patient age, chronic lung disease, a ratio of arterial oxygen partial pressure to fractional inspired oxygen <200 and hypernatraemia are predictors of prolonged intubation.
A previous study 17 has also shown that patients who remain on mechanical ventilation for a long time following tracheotomy are predisposed towards tracheal stenosis. Patients who undergo tracheotomy and are mechanically ventilated for a long period of time are at a high risk of mechanical trauma to the tracheal mucosa, owing to the movement of the cannula when swallowing and the positive pressure associated with mechanical ventilation, or the need to replace the cannula with another cannula of the same type or larger size to maintain good airway pressure because of airway leakage after prolonged use of the original cannula. Thus, the longer is the duration of mechanical ventilation, the greater is the risk of tracheal stenosis. Thus, for patients who must be mechanically ventilated for a prolonged period of time, measures should be taken to improve the care of tracheostomy tubes and to avoid factors that may damage the airway mucosa. 23 A previous study showed 23 that prolonged postoperative mechanical ventilation (≥7 days) is an independent risk factor for the development of tracheal stenosis after tracheotomy.
Previous studies have shown that tracheotomy is generally performed between the second and third or third and fourth cartilaginous rings, but if the surgical site is too high there will be damage to the first tracheal cartilaginous ring, resulting in tracheal softening and stenosis.20,42 A too-high incision will result in damage to the overall structure of the trachea, softening, collapse and stenosis. 23 Therefore, careful palpation, the choice of the appropriate incision site and the avoidance of damage to the cartilaginous rings should reduce the risk of tracheal stenosis. 23
It is now well established 16 that obesity is associated with a chronic inflammatory state characterised by the excess production of pro-inflammatory markers. Patients with a chronic inflammatory state such as obesity may be more susceptible to laryngotracheal injury. Li et al. 18 showed that obesity is associated with prolonged mechanical ventilation and respiratory failure, both of which are associated with a high risk of stenosis, and are indications for tracheotomy. Therefore, to reduce the incidence of post-tracheostomy tracheal stenosis, clinicians should perform tracheotomy early in patients with obesity who are expected to require prolonged mechanical ventilation. 18 A previous study has shown 16 that patients with diabetes are particularly vulnerable to airway injury, and Ettema et al. showed that the presence of diabetes is associated with more severe stenosis. Poor wound healing in patients with diabetes is principally caused by an inadequate supply of glucose for normal cellular aerobic metabolism, resulting in poor wound fibroblast function, lower collagen fibre deposition during epithelial proliferation and inadequate tensile strength of the wound. 17 It has been shown that the lack of platelet-derived growth factor during wound healing in patients with diabetes predisposes toward infection in addition to delayed healing because of impaired humoral and cellular immunity, which permits bacterial overgrowth on the wound surface, leading to the formation of large amounts of granulation tissue and subsequently scar tissue. In addition, patients with diabetes tend to have atherosclerosis, which involves a narrowing and thinning of the arterial lumen, low blood flow and poor oxygen supply, which has a negative effect on the healing of tracheal wounds after tracheotomy. 16
Using an animal model, Sasaki et al. demonstrated that respiratory infections increase the risk of tracheal stenosis. 43 Furthermore, after tracheotomy, there was a significantly higher incidence of concomitant tracheal stenosis in animals with a respiratory tract infection than in those without. 43 Respiratory infection significantly increases the incidence of tracheal stenosis, and trauma to the mucosa can lead to bacterial inflammation, localised oedema and granulomatous proliferation, resulting in narrowing of the trachea, and therefore a higher risk of tracheal stenosis. Therefore, measures should be taken to prevent or treat respiratory infections to reduce the risk of tracheal stenosis. 16
Regarding the size of the endotracheal tube, the studies by both Luo et al. 15 and Wei et al. 21 showed that C/T > 150% is a risk factor for tracheal stenosis, and we believe that the diameter of the endotracheal tube affects the risk of tracheal stenosis and that when the diameter is too large, the tube may compress the tracheal wall, causing ischemic damage to the wall and inflammation, which can lead to granulomatous tissue hyperplasia and subsequent stenosis. In the study by Su et al., 44 when the tracheal diameter, cuff pressure and duration of intubation were kept constant, it was found that tracheal wall pressure was higher when larger tubes (7.5-mm and 8.0-mm internal diameter) were used, and tracheal stenosis could be successfully modelled in animals intubated with larger tubes, which suggests that excessive tube size is a risk factor for tracheal stenosis. Furthermore, Ming et al. 45 showed that a tube of diameter ≥8 mm is a risk factor for tracheal stenosis, and Li et al. 42 also showed that tube size is a risk factor.
Regarding the cuff pressure of the endotracheal tube, the intra-cuff pressure is not proportional to the pressure exerted on the tracheal wall by the cuff. Instead, the tracheal wall pressure is related to the size of the cuff, the degree of expansion of the trachea and the size of the contact area between the cuff and the tracheal wall, as well as the intra-cuff pressure. 44 Li et al. 18 showed that a tube cuff pressure >30 cm H2O is a risk factor for tracheal stenosis, and Qin et al. 20 showed that balloon pressure is a risk factor for tracheal stenosis, but all of these studies showed that the tube cuff pressure or balloon pressure is only one of the risk factors, and it is not an independent risk factor.
Kim et al. 46 found that the degree of tracheal stenosis increases in proportion to the cuff pressure and the duration of tracheal intubation. In addition, another study showed that 31% to 95% of patients in intensive care develop ischaemic injury to their tracheal walls after intubation and that this injury is positively associated with the cuff pressure. 44 Therefore, we believe that high intra-cuff pressure is a risk factor for tracheal stenosis after intubation.
If the tracheal cuff pressure is too high it can cause varying degrees of damage to the patient's tracheal mucosa, which can lead to inflammation and tissue hyperplasia, and subsequently tracheal stenosis, and therefore the tracheal cuff pressure should be monitored regularly in patients who are undergoing long-term mechanical ventilation. 20 Moon et al. 2 showed that tracheal stenosis may result when the pressure of the balloon exceeds the recommended 20 to 30 cm H20, but the tracheal cuff pressure often exceeds the recommended range and the pressure is often only measured only after placement of the tube, rather than throughout the period of intubation. This is important, because the cuff pressure varies with body position, neuromuscular relaxation, temperature, altitude, nitrous oxide administration and positive pressure ventilation. Thus, we agree with Moon et al. 2 that cuff pressure may be a risk factor for tracheal stenosis, that there is a need to regularly monitor cuff pressure throughout the period of intubation and that there is a need to develop a more practical tool for the measurement of cuff pressure.
During the COVID-19 pandemic, there was an increase in the incidence of post-mechanical ventilation-associated stenosis, owing to the impairment in visualisation associated with the use of personal protective equipment, cuff overinflation and trauma associated with prolonged intubation. 47 It has been reported that up to 40% of the patients who were chronically intubated had COVID-19 infection at this time. 48 In addition, the SARS-CoV-2 virus exacerbates the ischaemic tracheal mucosal injury by inducing a prethrombotic and antifibrinolytic state, secondary to microvascular injury and necrosis, and because of the need for the prolonged systemic use of high-dose steroids.49,50 Tracheal epithelial changes caused by the SARS-CoV-2 virus itself is considered to predispose towards tracheal stenosis in patients with COVID-19.51–53
There were a number of limitations of the present study. Firstly, most of the risk factors identified in the study, although being associated with statistically significant findings, were identified in a small number of studies with relatively small samples sizes. Therefore, the results should be interpreted with caution. Secondly, there was a risk of bias, owing to the few studies included. Thirdly, the data obtained from some of the included studies were highly heterogeneous, but owing to their small number, subgroup analyses could not be performed, which may have affected the accuracy of the results. Finally, there may have been publication bias, but owing to the small number of included studies, this could not be tested for.
Conclusion
Current evidence suggests that tracheotomy, obesity, diabetes, the duration of mechanical ventilation, the duration of intubation, an incision positioned too high and respiratory infection are risk factors for tracheal stenosis, but further research is needed to identify any remaining risk factors. The findings of the present study have important implications for future research and clinical practice, but to date, only a few relatively small studies have evaluated the effects of the proposed risk factors on tracheal stenosis, and therefore further high-quality studies are needed.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241275884 - Supplemental material for Risk factors for patients with tracheal stenosis: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241275884 for Risk factors for patients with tracheal stenosis: a systematic review and meta-analysis by Siqi Hong, Xiaobing Wu, Haihuan Feng, Qing Zhang, Xiaohan Wang, Minmin Chang, Xiuli Chen and Weijuan Liu in Journal of International Medical Research
Footnotes
Author Contributions
SH contributed to the design and conduct of the study, the data analysis, and the drafting of the manuscript. XW performed the systematic review, critically revised the manuscript, and approved the final version of the manuscript. HF assisted with the generation of the systematic search strategy, critically revised the manuscript, and approved the final version of the manuscript. QZ critically revised the manuscript and approved the final version. XW critically revised the manuscript and approved the final version. MC critically revised the manuscript and approved the final version. XC critically revised the manuscript and approved the final version. WL contributed to the design and conduct of the study, data analysis, and critical editing of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The study was funded by The First Affiliated Hospital of Guangzhou Medical University under the Outcome and Clinical Translation Nursery Programme (grant no. zh202114).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.