
Abstract
Brucellosis is a common zoonotic infectious disease worldwide that can affect almost all organs in the human body. Osteonecrosis of the femoral head has numerous possible causes. Patients usually experience movement disorders, severe pain, and an extremely high disability rate. We herein describe a 32-year-old male farmer living in Shanxi, China who accidentally injured his right hip while working. After 1 month of rest, the pain in the right hip was relieved, and the patient began to walk again. However, after 2 months of walking, he developed aggravated pain and claudication in the right lower limb. Examination revealed shortening of the right lower limb. We carried out a comprehensive and systematic examination and performed total hip arthroplasty. Hip trauma with Brucella infection may progress to osteonecrosis of the femoral head in a short period of time without typical symptoms of Brucella infection. Systematic examination and treatment should be performed at an early stage to prevent the eventual deterioration of the disease and serious complications that are difficult to treat.
Introduction
Brucellosis, also known as undulating fever, is a common zoonotic disease caused by brucellosis infection worldwide.1,2 The main clinical manifestations are fever (87%), fatigue (63%), arthralgia (62%), and muscle pain (56%), and osteoarthritis is particularly common in adults. 3
Osteonecrosis of the femoral head (ONFH) is a nonspecific disease that is influenced by a variety of factors. Femoral head necrosis can be categorized into two main types: traumatic and nontraumatic. Traumatic ONFH is mainly caused by vascular destruction or mechanical occlusion secondary to hip trauma such as femoral neck fracture and hip dislocation. Nontraumatic ONFH is mostly caused by corticosteroid use, alcohol abuse, decompression sickness, sickle cell anemia, and idiopathic causes. Few reports have described ONFH caused by other factors. 4
In this paper, we report a case of total hip arthroplasty (THA) in a patient who was most likely infected by Brucella after hip trauma.
Case presentation
The reporting of this study conforms to the CARE guidelines. 5 A 32-year-old male farmer fell from an approximately 3-m height while moving fertilizer on 15 March 2020. He landed on his right hip and felt severe pain in this hip, and movement of the hip was limited. After consulting the local village doctor, he took bed rest. More than 1 month later, he was able to walk on level ground and felt slight pain and claudication in the right hip. After walking for more than 2 months, the patient experienced severe pain in his right lower limb and began limping; he also realized that his right lower limb was shortened. Therefore, he was admitted to Lingchuan County Hospital of Traditional Chinese Medicine on 7 August 2020. He underwent an orthographic X-ray examination of the pelvis, which indicated stage IV necrosis of the right femoral head and decreased bone density of the right femur (Figure 1(a)). Referral to a superior hospital was recommend. On 27 August, the patient was admitted to Heping Hospital for a pelvic orthographic examination, which revealed stage IV necrosis of the right femoral head, a bone-density shadow around the big rotor of the right hip, and decreased bone density of the right femur (Figure 1(b)). Considering the possibility of infection in the right hip, further examination was suggested to clarify the cause of the patient’s condition. However, the patient refused this recommendation because of its cost. On 7 September, the patient was admitted to Li Xinru Hospital in Changzhi. Anteroposterior and lateral radiographs of the right hip joint revealed the same findings as described above (Figure 1(c)). A plain computed tomography scan of the right hip joint suggested extensive necrosis of the right femoral head and osteoporosis and abscess formation of the right femur (Figure 2). Magnetic resonance imaging (MRI) of the bilateral hip joints indicated necrosis of the right femoral head and effusion and abscess formation of the right hip joint (Figure 3). On 9 September, blood culture examination results showed no bacterial growth after 5 days of culture. On 15 September, right hip abscess puncture and joint cavity fluid culture were performed. The result on 21 September revealed growth of Brucella, and Brucella infection of the right hip joint was thus diagnosed. The patient was recommended to receive standardized outpatient treatment with oral doxycycline and rifampicin (doxycycline at 100 mg twice daily on the first day and 100 mg once daily for 3 months thereafter; rifampicin at 0.60 g once daily on an empty stomach for 3 months).
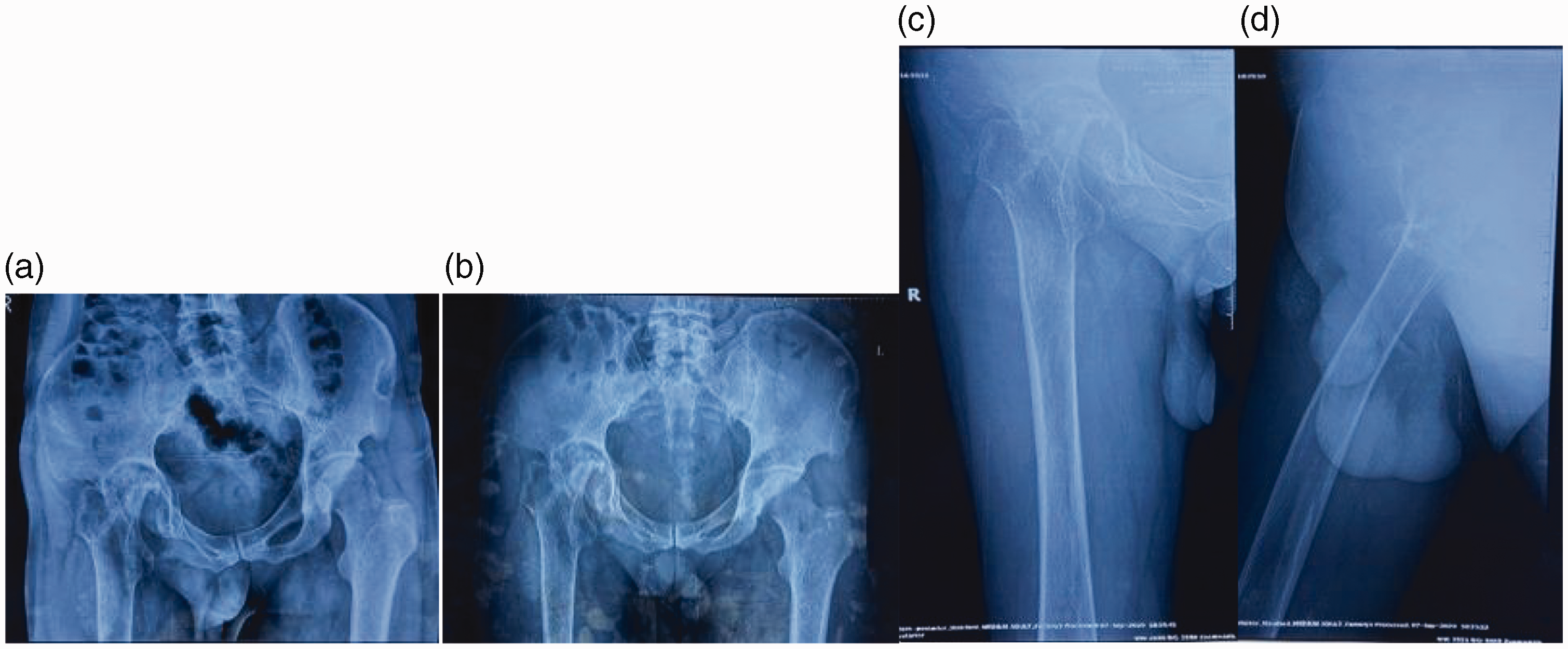
(a) Orthographic X-ray examination of the pelvis in Lingchuan County Hospital of Traditional Chinese Medicine. (b) Orthographic X-ray examination of the pelvis in Heping Hospital and (c) Anteroposterior and lateral radiographs of the right hip joint in Li Xinru Hospital. The bone of the right femoral head was destroyed, the femoral neck was significantly shortened, and the joint space had disappeared.

Plain computed tomography scan of the right hip joint in Li Xinru Hospital.

Magnetic resonance imaging scan of the bilateral hip joints in Li Xinru Hospital.
Despite receiving the standardized treatment, the patient felt that the effect was poor and that his symptoms were not relieved. On 30 November 2020, he presented to Li Xinru Hospital again, and a plain MRI scan of the hip was performed. The results showed necrosis of the right femoral head and effusion and abscess formation of the right hip joint, without significant changes in the range of the abscess (Figure 4). Therefore, the patient was treated with incision and drainage of the stage I abscess of the right hip joint, followed by oral treatment with doxycycline and rifampicin for 3 months with good results (doxycycline at 100 mg twice daily on the first day and 100 mg once daily for 3 months thereafter; rifampicin at 0.60 g once daily on an empty stomach for 3 months).

Plain magnetic resonance imaging scan of the hip in Li Xinru Hospital.
On 6 May 2021, the patient presented to our hospital for stage II THA and was admitted to our department with right ONFH and Brucella infection. Examination revealed a body temperature of 36.4°C, pulse of 94 beats/minute, respiratory rate of 18 breaths/minute, blood pressure of 129/76 mmHg, height of 174 cm, and weight of 75 kg. The patient was conscious with clear speech, anxious expression, and generally high spirit. Cardiopulmonary examination showed no obvious abnormality. Two old surgical incisions of about 10 cm in length and two scar tissues of about 2 cm in length were observed on the right hip. No redness, swelling, or rupture was noted. We observed muscle atrophy of the right lower limb and approximately 2 cm shortening of the right lower limb compared with the left limb. The skin temperature of the right hip was normal. Tenderness was noted in the right groin area. The movement of the right hip joint was limited (flexion 90°, extension 5°, adduction 15°, abduction 20°, internal rotation 5°, and external rotation 5°). Special examination results were as follows: Thomas test, positive; strength of flexor hip muscle, grade III; left quadriceps muscle strength, grade IV; and no obvious abnormality in the other limbs. The dorsal arteries of both feet were palpable, and there was no obvious abnormality in the skin sensation of both lower limbs. Physiological reflexes were present, but pathological reflexes were not elicited. The patient's preoperative Harris hip score was 35.41 in the right hip, and the score in the left hip was normal.
On 7 May, we reviewed the patient's Rose Bengal plate test result and brucellosis standard tube agglutination test result. The Rose Bengal plate test was negative. The Brucella agglutination test results were 1:25(−), 1:50(−), 1:100(−), 1:200(−), and 1:400(−). Preoperative renal function tests and immunoglobulin tests were all within the reference ranges, and the results of other tests are shown in Table 1.
Preoperative laboratory examination results.

WBC, white blood cell; RBC, red blood cell; Hb, hemoglobin; PLT, platelet; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; IBIL, indirect bilirubin; TBIL, total bilirubin.
Anteroposterior and lateral radiographs of the right hip joint showed necrosis of the right femoral head and decreased bone density of the right femur (Figure 5). Plain pelvic computed tomography and three-dimensional reconstruction showed mixed-density foci in the front aspect of the femur and abnormal-density foci in the rear aspect of the iliac hip. We considered these to indicate hip arthritis and osteoporosis (Figure 6). MRI of the right hip showed ONFH with arthritis of the hip, an abnormal signal in the pectineus of the right gluteus minimus muscle and rectus femoris muscle, and possible myositis ossificans (Figure 7).

Anteroposterior and lateral radiographs of the right hip joint in Changzhi People’s Hospital.

Plain pelvic computed tomography scan and three-dimensional reconstruction in Changzhi People’s Hospital.

Magnetic resonance imaging of the right hip in Changzhi People’s Hospital.
Treatment and outcome
On 18 May, we performed THA after obtaining the patient's consent to treatment. During the operation, the joint cavity was opened and the joint fluid was found to be clear without purulent secretions. We cultured the joint fluid before and after the joint capsule incision, and the results indicated no bacterial growth after 72 hours of culture. To prevent recurrence of the Brucella infection, we used physiological saline containing gentamicin and doxycycline to soak the pulp cavity and wound surface many times during the operation. The entire operation was smoothly performed.
The 1-day postoperative laboratory examination results are shown in Table 2. Postoperative X-ray review showed that the prosthesis was well positioned and firmly fixed (Figure 8). The Harris hip score was 87.325 with slight claudication 3 months after surgery. After 1 year, the patient was able to walk normally with slightly limited abduction of the right hip joint.
Postoperative laboratory examination results.

WBC, white blood cell; RBC, red blood cell; Hb, hemoglobin; PLT, platelet; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein.

(a) Orthographic X-ray examination of the pelvis in Changzhi People’s Hospital and (b, c) Anteroposterior and lateral radiographs of the right hip joint in Changzhi People’s Hospital.
Discussion
Brucellosis is a natural epidemic disease with various clinical manifestations. Typical symptoms are fever, hyperhidrosis, arthralgia, and enlargement of the liver, spleen, and lymph nodes. However, if bone and joint pain is the only local clinical manifestation of this disease, misdiagnosis and missed diagnosis readily occur because of its nonspecific manifestations in the musculoskeletal system. 6 In the present case, the patient’s father was a shepherd and was regularly in contact with sheep. However, the patient did not have a typical repeating fever; he only had pain and shortening of the right lower limb. These symptoms alone were relatively rare and made the diagnosis quite difficult.
The patient had a clear history of severe trauma-induced pain in the right hip, and he stayed in bed for 1 month. We considered that the patient might have developed a fracture of the right femoral neck at that time, but he had not undergone an imaging examination, resulting in an unclear diagnosis. A review of the relevant literature showed that Brucella infection can lead to ONFH.7,8 However, the patient in this case had a short course of ONFH with basic dissolution of the femoral head, obvious osteoporosis at the proximal end of the femur, and a huge abscess around the hip joint; thus, his condition was more serious than the ONFH mentioned in previous reports.7,8 We also noted that the patient had no known history of Brucella infection before the trauma, and the conservative treatment for the trauma was initially effective. The right hip pain thereafter worsened, and the right lower limb became shortened. Therefore, we believe that the ONFH in this case may have been caused by the combination of trauma and Brucella infection and that the trauma preceded the Brucella infection. This may have been related to a decrease in immunity during the injury.
The ONFH in this case developed over the 5-month period from the patient’s injury in March 2020 to the first imaging examination in August 2020. The disease course was rapid, similar to the temporal characteristics of rapidly progressive femoral necrosis and rapidly destructive hip arthritis. 9 However, the etiology of the patient’s condition in this case is relatively clear. Therefore, the correlation among these three pathological mechanisms remains to be further studied.
Throughout the diagnostic procedures, the patient did not have a typical fever. When the hip pain recurred, both the patient and the local doctor thought that it was the sequela of previous trauma. Therefore, they did not seek medical treatment, resulting in delayed diagnosis of the patient’s condition. The patient was diagnosed with a huge abscess of the right hip joint, and the effect of treatment with doxycycline and rifampicin was unsatisfactory for more than 2 months. However, after the patient underwent incision and drainage of the abscess, the treatment effect was good for 3 months. Brucella, as an intracellular parasitic bacterium, has a strong ability to resist phagocytosis by macrophages, and its proliferation and replication also reduce its phagocytosis by macrophages to a certain extent. 10 Therefore, for better treatment efficacy, drugs need to be delivered into the infected cells first. We believe that the reason for the ineffective drug treatment in this case may have been related to compression of the surrounding tissues after formation of the hip abscess and interruption of blood to the femoral head, which prevented drugs from reaching the site of infection. Therefore, we suggest that patients with Brucella hip arthritis should undergo debridement and drainage in the early stage if the imaging examination indicates obvious abscess formation; otherwise, the effect of drug therapy may be poor. In terms of the choice of surgical prosthesis for such patients, the current literature 11 confirms that an ultra-short anatomical cementless stem (Proxima Stem; DePuy Synthes, Warsaw, IN, USA) can retain more bone mass in the proximal femur and that it is more consistent with the physiological and mechanical structure of the proximal femur, thus prolonging the service life of the prosthesis and reducing the possibility of revision. The patient in the present case had been informed in advance that the Proxima Stem could be used. However, because of his financial limitation and the lack of experience with Proxima Stem replacement in this region, a standard cementless stem system was finally chosen.
Our patient exhibited slightly limited abduction of the right hip joint and mild claudication after right THA, which may have been related to the myositis ossificans of the adductor muscle group caused by the healing of the abscess around the hip before surgery. Therefore, for this patient, combination treatment involving stage I abscess debridement, THA, and standardized anti-Brucella therapy may have been a better choice. 12
Conclusions
Hip trauma with Brucella infection may result in ONFH in the absence of typical symptoms of Brucella infection accompanied by the formation of a large abscess around the hip. After the abscess has formed, drug treatment may not be effective. Additionally, the formation of myositis ossificans around the hip joint after abscess removal may also affect the stage II post-THA outcome. The history of trauma and Brucella infection in this patient were relatively clear. However, which of these two factors (or both) is responsible for his clinical course remains unclear. This case provides a research direction for future clinical work, but more in-depth research is still needed to support our conclusions.
Research Data
Research Data for Rapidly progressive femoral head necrosis due to post-traumatic Brucella hip infection: a case report
Research Data for Rapidly progressive femoral head necrosis due to post-traumatic Brucella hip infection: a case report by Wei-Yang Hu, Guang-Zong Ren, Jia-Jin Lv and Gui-Yue Chen in Journal of International Medical Research
Footnotes
Acknowledgements
We are grateful to the patient and all the researchers, including the physicians, pathologists, and technicians, who participated in this case.
Author contributions
The manuscript has been carefully read and approved by all the authors. Each of the authors contributed greatly to the manuscript. Wei-Yang Hu and Guang-Zong Ren were the main authors of the manuscript, and Jia-Jin Lv provided guidance for the literature search. Gui-Yue Chen reviewed the manuscript and contributed a great deal of knowledge to its creation.
Data availability statement
The datasets used for the current case report are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the work reported in this paper.
Ethics statement
All procedures performed involving human participants were in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The requirement for ethical permission was waived because of the nature of the study (case report). Written informed consent was obtained from the patient on admission.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.