
Abstract
Hepatic subcapsular hematoma (HSH) is an uncommon complication of pregnancy and is associated with elevated rates of maternal and foetal mortality. The rupture of an HSH is a critical situation that necessitates immediate and timely intervention to prevent loss of life. We present here, a case of a spontaneously ruptured massive HSH caused by preeclampsia. In addition, we conducted a comprehensive review of existing literature, encompassing 49 cases of HSH associated with pregnancy. If a pregnant woman with gestational hypertension experiences right upper abdominal pain with shoulder pain or radiating shoulder pain, it is crucial for her to have an urgent abdominal ultrasound because of the potential development of HSH and/or rupture. Our review of current literature suggests that opting for a caesarean section may offer notable advantages in preventing HSH rupture.
Background
Hepatic subcapsular haematoma (HSH) is a rare and potentially life-threatening complication of pregnancy and it may result in liver rupture.1–3 Its precise incidence is challenging to ascertain, but it has been estimated to range from 1 in 45,000 to 1 in 225,000 pregnancies.3,4 Maternal mortality associated with HSH ranges from 17–59%, 5 and foetal mortality ranges from 38–62%. 6 Most mothers develop HSH as a complication of preeclampsia and/or HELLP (Haemolysis, Elevated Liver Enzymes, and Low Platelets) syndrome.4,7 Hypertensive disorders during pregnancy are significant contributors to maternal and perinatal mortality rates, with a worldwide prevalence estimated to range from 2–8% of pregnancies.8,9 Although the HELLP syndrome is rare and affects only approximately 1% of pregnancies, it is observed in 10–20% of pregnant women who develop severe preeclampsia. 10
The exact underlying mechanisms leading to HSH and subsequent spontaneous liver rupture remain unclear. However, intrahepatic haemorrhage probably leads to the formation of an HSH, which may rupture because of expansion, elevated blood pressure (BP), external force, or trauma. Importantly, the haematoma and its rupture predominantly manifest in the right liver lobe, 6 and women presenting with suspected HSH typically report upper abdominal pain.11–13 In cases where the haematoma ruptures, short-term shock may ensue, posing a risk of maternal and foetal mortality.
Currently, existing literature on HSH consists predominantly of case reports and case series, without a standardized reference guide. We report here, a case of a spontaneous large liver hematoma that occurred in a woman with preeclampsia, but without the HELLP syndrome. The HSH ruptured during an emergency caesarean section. In addition, we conducted a comprehensive review of existing literature and summarised diagnostic and treatment approaches used in this condition. We hope that the findings of our study will be useful in facilitating early identification and appropriate management of HSH, thereby mitigating adverse effects on pregnant women and perinatal infants.
Case report
A 36-year-old woman (gravida 1, para 0) without any significant previous medical history, presented to the outpatient department of the Women and Children's Hospital affiliated with the University of Setif, Algeria with gestational hypertension and a diagnosis of preeclampsia. At 39 weeks gestation, she had experienced intermittent and persistent upper abdominal pain for a duration of 12 hours. She had a non-pale complexion, pulse rate 95 beats per minute, respiratory rate 18 breaths per minute, and BP 160/95 mmHg. Primary laboratory findings included: white blood cell (WBC) count, 14.2 × 109/l; haemoglobin (Hb), 12.2 g/dl; platelets (PLT), 199 × 109/l; aspartate aminotransferase (AST), 37.0 UI/l (normal, <40); alanine aminotransferase (ALT), 29.00 UI/l (normal, <35); alkaline phosphatase (ALP), 232 UI/l (normal, <240); gamma glutamyl transpeptidase (GGTP), 23 UI/l (normal, 10–40); total bilirubin (BIL), 10.9 mg/l (normal, <10); combined or direct bilirubin, 1.97 mg/l (normal, <3); free or indirect bilirubin, 8.95 mg/l (normal, <6).
Emergency ultrasound examination showed findings of a viable foetus and identification of a heterogeneous diaphragm/liver ultrasound fluid collection measuring 51.9 mm in thickness and extending approximately 16.2 cm below the membrane appearance (Figure 1(a)). The liver had normal dimensions, a regular contour, and a uniform echo structure. No stones were observed in the biliary tracts and the intrahepatic and extrahepatic bile ducts did not display signs of dilatation. The kidneys had normal dimensions, and there was no evidence of renal pelvis dilatation or kidney stones. There was no observable presence of fluid in the abdominal cavity. Subsequently, the patient's hematoma size increased to 19.2 × 52.5 cm prior to surgery, with no apparent indication of hemoperitoneum (Figure 1(b)).
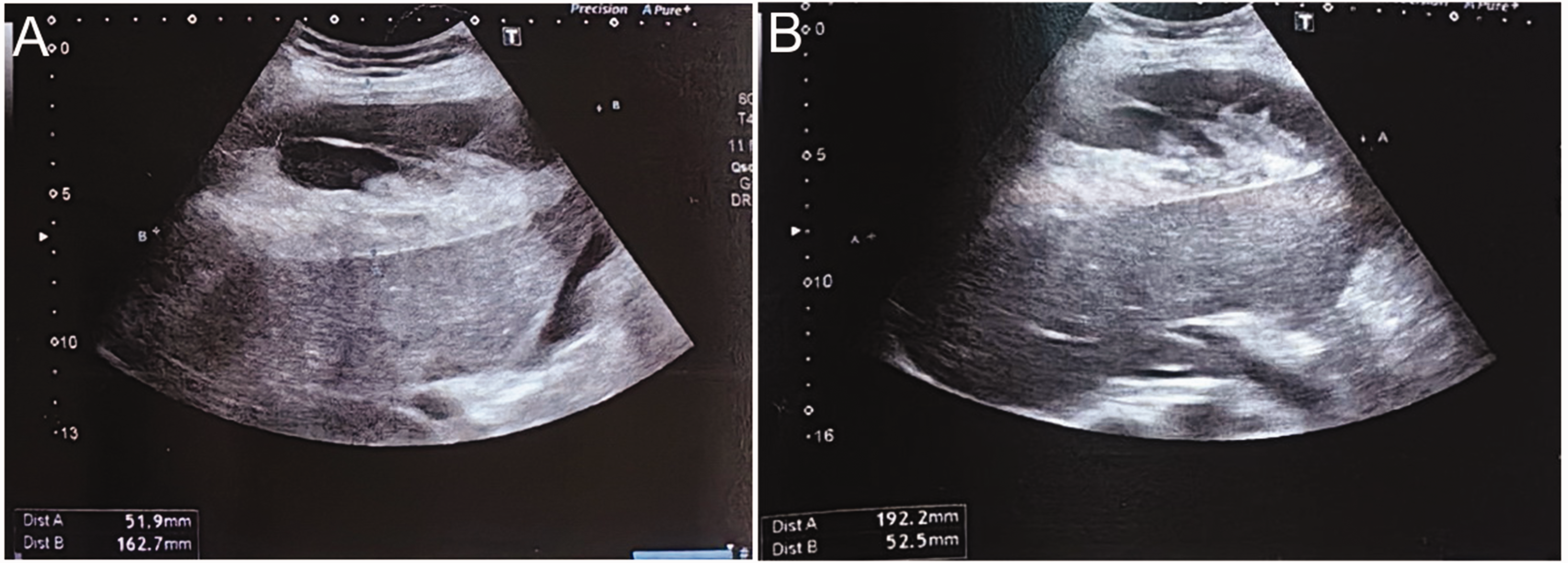
(a) Emergency ultrasound examination showed findings of a viable foetus and identification of a heterogeneous diaphragm/liver ultrasound fluid collection measuring 51.9 mm in thickness and extending approximately 16.2 cm below the membrane appearance and (b) subsequently, the patient's hematoma size increased to 52.5 cm × 19.2 prior to surgery with no apparent indication of hemoperitoneum.
An emergency caesarean section was promptly conducted. A proficient liver surgery team was prepared in the operating theatre. Surgical exploration showed a hemoperitoneum containing 3000 ml blood, that affected the entire right lobe of the liver; there was active bleeding and while the uterus remained intact, it was saturated in blood. A male foetus was delivered alive (Apgar score, 2/2/4 at 1, 3, and 5 minutes, respectively; birth weight of 4900g). Subsequently, the uterine incision was promptly sutured. An additional longitudinal incision was made beneath the xiphoid process, and showed a significant intraperitoneal haemorrhage originating from a large ruptured subcapsular hepatic hematoma encompassing the entire right lobe of the liver. Multiple evident bleeding points were observed along the right edge of the liver (Figure 2(a)). Following electrocoagulation at the bleeding site, a reduction in bleeding was observed at the wound. Absorbable gauze and three gauze packs with surgical packing were use to manage the haemorrhage effectively at the incision edge of the liver (Figure 2(b and c)). The surgical procedure involved two incisions (Figure 2(d)). Throughout the surgery, the woman received a transfusion of 12 units of red blood cells and four units of fresh frozen plasma. On the third postoperative day, a second surgery was conducted and upon removal of the compressing cotton pads from the liver, no bleeding or oozing was observed at the wound site. The patient subsequently experienced a complete recovery. A follow-up appointment with our team one month after delivery showed a reduction in the haematoma.

Intra-operative findings following a spontaneously ruptured hepatic subcapsular haematoma (HSH). (a) Multiple evident bleeding points were observed along the right edge of the liver (green arrow). (b and c) Absorbable gauze and three gauze packs with surgical packing were use to manage the haemorrhage effectively at the incision edge of the liver and (d) postoperative appearance of two abdominal incisions (green arrows).
The reporting of this study conforms to CARE guidelines. 14 The woman provided written informed consent for publication of her anonymised case report and accompanying images. Ethical committee approval was not required for this case report.
Summary of literature review
HSH of the liver is an uncommon condition that can have grave implications, including patient mortality, particularly during pregnancy. Due to its infrequent occurrence, medical practitioners often fail to recognize its presence. We conducted two separate searches of the MEDLINE database to identify all relevant studies published up to January 2, 2024, which reported data on cases of HSH diagnosed during pregnancy. Search terms included, “subcapsular liver hematoma,” “HELLP syndrome,” “rupture,” and “preeclampsia”. Only articles written in English were considered for subsequent analysis. The following items, when available, were extracted: first author; publication date; country; age; gestational age; presence of preeclampsia; HELLP syndrome; rupture; diagnostic method; maximum levels of ALT and AST; platelet nadir; delivery method; time of discovery of HSH; treatment; outcome/hospitalization time; timing of rupture; symptoms.
In total, we identified 37 reports involving 49 cases of HSH diagnosed during pregnancy (Table 1).2,6,11–13,15–45 The studies were case reports or small case series. Ten reports were from the USA, four from the UK, three from Turkey, two each from Spain, France and Ireland, and one in each of the following countries/regions: Nepal; China; Australia; Poland; Denmark; Romania; Columbia; Ivory Coast; Taiwan; Canada; Morocco; Ethiopia; Portugal; Germany. The mean (SD) maternal and gestational ages at suspicion of HSH during pregnancy were 31.8 (4.8) years and 34.0 (5.3) weeks, respectively. In total, 42 (86%) had preeclampsia, 6 (12%) had normal blood pressure, and one woman had eclampsia. Additionally, 39 (80%) women were diagnosed with HELLP syndrome, of these 37 (76%) had preeclampsia/eclampsia (two cases reported no hypertension). Only 4 (8%) pregnant women with HSH had preeclampsia alone. Interestingly, four (8%) pregnant women with HSH, had normal BP and no evidence of HELLP syndrome. In total, 30 (61%) pregnant women experienced an HSH rupture. Of the 49 pregnant women, 35 (71%) had a caesarean section and 13 (26%) opted for vaginal delivery. Two women underwent hysterectomy as a result of a ruptured hematoma.
Characteristics of patients with hepatic subcapsular hematoma (HSH) from the review of 37 studies involving 49 cases.

Abbreviarions: -, data not recorded; ALT, alanine aminotransferase; AST, aspartate aminotransferase; AU, Australia; CS, caesarean section; CT, Computed tomography; E, eclampsia; GA, gestational age; HELLP, Haemolysis, Elevated Liver Enzymes, and Low Platelets; Hys, Hysterotomy; IC, Ivory Coast; intra-op, intraoperative; MRI, magnetic resonance imaging; PE, preeclampsia; PLT, platelets; Pre-op, preoperative; post-op, postoperative; PP, postpartum; US, Ultrasound; VD, Vaginal delivery.
Women with suspected HSH manifest various symptoms, of which, pain is the most common. From our literature search, pain was reported in 43 (88%) of cases. The specific types of pain included: right upper quadrant pain (22, 45%); epigastric pain (16, 33%); upper abdominal pain (7, 14%); shoulder tip pain/radiating to shoulder (10, 20%); lower abdominal pain (1, 2%); back pain (3, 6%); neck pain (2, 4%); right subcostal pain (1, 2%); perineal pain (1, 2%) (Figure 3). In addition, vomiting was observed in 11 (22%) of cases, while nausea was reported in 4 (8%) cases. Furthermore, jaundice, fever, and diarrhoea were experienced by three separate women.

Common symptoms of hepatic subcapsular haematoma (HSH) from the review of 37 studies involving 49 cases.
Discovery of the hematoma occurred at the following times: prenatally, 3 (6%) cases; preoperatively, 13 (27%); intraoperatively, 8 (16%) cases; postoperatively, 11 (22%) cases; postpartum 14 (29%) cases (Figure 4). Interestingly, six of the 13 women who had a vaginal delivery experienced rupture of the hematoma rupture all detected post-partum (Table 1). Furthermore, 10 of the 35 women who underwent caesarean section were diagnosed with hematoma rupture prior to surgery. Additionally, during surgery, 8/35 cases were found to have ruptured hematomas, while 5/35 were diagnosed with hematoma rupture after the surgical procedure.

The timing of the discovery of the hematoma from the review of 37 studies involving 49 cases.
Several methods were used for treatment management and included: conservative treatment (22, 45%); liver packing (18, 37%); liver transplantation (2, 4%). Other treatment approaches included: hepatic vessels block; hepatorrhaphy; partial hepatectomy; blood clots removed; interventional radiology. For the 30 cases with hematoma rupture, 23 (77%) underwent various surgical interventions including liver packing (14, 47%), conservative treatment (7, 23%) and liver transplantation (2, 7%). For the 19 cases with unruptured hematoma, 15 (79%) received conservative treatment, 3 (16%) underwent liver packing treatment and the remaining case had blood clots removed (Table 1). For the 27 women who were hospitalised mean (SD) hospital stay was 23.3 (22.8) days (range 6–120 days). Five (10%) women died. For 10 (20%) cases, details of outcome were not provided, 6 (12%) cases were lost-to-follow-up and the hematoma of the remaining case show gradual decrease at 6-month follow-up.
The aetiology of HSH in relation to preeclampsia and/or HELLP syndrome remains inadequately understood. Vascular endothelial injury appears to exert a significant influence, as neovascularization has been observed within the affected parenchyma, and renders the newly formed vessels increasingly susceptible to haemorrhage during hypertensive episodes. 46 Some investigators have suggested that vasospasm serves as a primary catalyst for HSH. 47 They also suggest that fibrin deposition may induce platelet activation, thrombus formation, hepatic sinusoidal obstruction, capillary occlusion, and subsequent hepatic hemorrhage. 47 In addition, its pathogenesis is thought to encompass additional mechanisms, including the upregulation of inflammatory factors to activate the complementary system, thrombotic microangiopathy and microthrombosis, as well as endocytic injury leading to hepatic sinusoidal obstruction.8,48
As our review of current literature showed, symptoms associated with HSH include right upper abdominal pain, epigastric pain, severe right shoulder pain, nausea, and vomiting. Indeed, most patients present with right upper abdominal pain, 1 and the right lobe of the liver is affected in 75% cases.19,49 These symptoms may be mistaken for other conditions such as pulmonary embolism, acute fatty liver, acute cholecystitis, or pancreatitis. Consequently, it is imperative for healthcare professionals to exercise heightened caution when encountering pregnant women who present with upper right abdominal pain accompanied by shoulder pain, as this may indicate the presence of HSH.
The use of portable ultrasound for diagnosis of women with possible HSP is expedient, particularly for patients exhibiting signs of hematoma rupture and unstable vital signs.5,21 Moreover, the implementation of follow-up 3 D ultrasonography offers numerous advantages over conventional ultrasound in the diagnosis of ruptured HSH. 28 Furthermore, it is a useful method for post-treatment monitoring following HSH. Although computed tomography (CT) has demonstrated increased sensitivity and accuracy in diagnosing HSH, rupture, and active bleeding, it is not recommended for cases involving women with hemodynamic instability, intra-abdominal haemorrhage, or shock.33
Currently, there is a paucity of data comparing the likelihood of hematoma rupture between caesarean section and vaginal delivery. 50 However, caesarean section has been suggested to be the optimal approach for pregnant women with HSH, as it can effectively prevent the progression of HSH into severe hematoma rupture and bleeding. 25 Indeed, this literature review of 37 studies shows that 6/13 women who had vaginal delivery experienced haematoma rupture subsequent to childbirth. During the process of parturition, uterine contractions have the potential to augment abdominal pressure or exert compression on the abdomen, thereby potentially resulting in the rupture of a hematoma. Therefore, diminishing the provocation of heightened abdominal pressure that could potentially lead to hematoma rupture is obviously advisable. However, studies are required to confirm these suppositions.
Presently, there is a lack of definitive guidelines or consensus regarding the management of HSH. However, the two main approaches are conservative management and surgical intervention. The choice of the appropriate treatment plan should be based on several factors, including the stability of the patient's vital signs, abdominal indicators, foetal well-being within the uterus, the prevailing conditions within the hospital setting, availability of treatment modalities, and the preferences of the patient's family. Moreover, it is imperative to underscore the significance of multidisciplinary consultation to facilitate a comprehensive assessment of the patient's condition and enable informed decision-making. Several studies promote the use of conservative management in unruptured HSH cases, provided that haemodynamics remain stable and imaging shows minimal intra-abdominal fluid and absence of active bleeding.11,12,22,42 This approach entails actively addressing any anaemia, rectifying coagulation function, and administering liver protection treatment, while closely monitoring vital signs and hematoma size. Monitoring hemodynamic parameters and regular ultrasound or CT examinations are crucial for tracking alterations in the size of the HSH. Moreover, it is important to minimize symptoms such as vomiting and actively manage BP while avoiding convulsions. Conservative management is also advised in cases where surgical access to the area of the HSH is challenging. 30 In cases of hemodynamic instability and shock, immediate emergency exploratory laparotomy is necessary to ensure the survival of both the mother and baby. During the process of delivering the foetus, it is important to refrain from applying pressure on the abdomen to prevent inadvertent compression and rupture of the hematoma. Surgical interventions encompass a spectrum of techniques, ranging from liver tamponade or liver packing, to ligation of the portal vein or hepatic artery, as well as partial hepatectomy. 51 Additionally, liver transplantation is regarded as a viable approach for patients experiencing intractable liver haemorrhage or acute liver failure.6,32 From our literature review, we noted a mortality rate of 10% across the 49 cases. The deaths probably occurred due to ruptured hematoma, primarily attributable to complications such as disseminated intravascular coagulation, pulmonary edema, hepatic infarction, or acute renal insufficiency. 7 Therefore, it is crucial to identify HSH promptly to mitigate the mortality risk associated with hematoma rupture.
Discussion
In our current case, the pregnant woman with preeclampsia but without HELLP syndrome, exhibited right upper abdominal pain. Emergency ultrasound showed a viable foetus and a large HSH. The patient experienced a ruptured HSH during an emergency caesarean section. Haemostatic packs were used to stop the bleeding which ultimately proved successful. At follow-up one month after the birth, mother and baby were progressing well.
In conclusion, the significance of prompt diagnosis of HSH cannot be overstated, because it enables physicians to avert life-threatening intra-abdominal haemorrhage resulting from hematoma rupture and mitigate the risk of organ failure. In instances where pregnant women manifest upper abdominal pain, particularly with radiation to the shoulder, it is advisable to undergo abdominal ultrasound examination to exclude hepatic and other visceral pathologies. If feasible, CT imaging may be considered as an alternative diagnostic modality. In the event of upper abdominal pain or indications of upper abdominal issues and hemoperitoneum, caesarean section may be prioritized to mitigate the potential rupture of hematoma caused by heightened contractions or exertion during delivery. Additionally, surgery can facilitate exploratory purposes. Importantly, it is crucial to avoid compressing the upper abdomen during caesarean section because external force may lead to hematoma rupture. In cases of intra-abdominal haemorrhage, medical professionals should remain vigilant for upper abdominal pathologies and, if necessary, coordinate multidisciplinary treatment within the operating theatre.
Footnotes
Acknowledgements
We thank Ghoul Maroua (Department of Obstetrics and Gynecology, the Women and Children's Hospital affiliated with the University of Sedift, Algeria) for assistance in data collection.
Declaration of conflicting interests
The authors declare there are no conflicting interests.
Funding
This work was supported by the National Natural Science Foundation of China (81572563).