
Abstract
Nodular fasciitis (NF) is a benign and self-limiting fibroblastic proliferation that originates from the superficial fascia and extends into the subcutaneous tissue or muscle. It typically manifests in individuals aged 20 to 35 years, with rare occurrences observed in patients over the age of 60 years. We herein report a case involving a 75-year-old man with NF in the right vocal cord. The patient sought medical attention at the Department of Otolaryngology of our hospital because of a 1-month history of hoarseness and breathlessness. The diagnosis was unable to be confirmed through preoperative pathological examination. After admission to our hospital, various examinations were completed and surgical treatment was performed, and the postoperative histopathological findings revealed the presence of NF in the right vocal cord. NF of the vocal cord is a rare clinical entity. Given its rapid progression and propensity for marked infiltration, it often poses diagnostic challenges because it can mimic various malignant soft tissue tumors. Therefore, thorough exclusion of other neoplastic lesions is imperative prior to confirming the diagnosis of NF through pathological examination. Local surgical resection remains the primary treatment modality.
Keywords
Introduction
Nodular fasciitis (NF) is a non-neoplastic hyperplasia originates from the superficial fascia and extends into the subcutaneous tissue or muscle. It is characterized by an isolated, well-defined, rapidly proliferating, self-limiting soft tissue mass. NF predominantly affects young adults aged 20 to 40 years, and it shows no sex predilection.1,2 The disease primarily manifests in the upper extremities, followed by the trunk. It is particularly prevalent in the head and neck region among infants and young children, who develop nodules typically measuring <4 cm in diameter.2–4 Although NF commonly arises subcutaneously or within fascial tissue, it may also involve muscles or organs. The literature indicates that the prevalence of NF in the head and neck region ranges from 13% to 24%. NF in the head and neck is predominantly observed in the cervical region, frontal area, buccal region, orbit, scalp, oral cavity, mandible, external auditory canal, and paranasal sinuses. 5 With its rapid growth, absence of signs of infection, and histological features of marked cytosis, active mitosis, and border invasion, NF often presents a diagnostic challenge because it can be misdiagnosed as various soft tissue sarcomas. Achieving timely and accurate diagnosis remains difficult.
The etiology of NF is elusive. Some scholars hypothesize a potential association with viral infection, suggesting its possible classification as a distinct inflammatory proliferative response. 6 However, this hypothesis lacks confirmation. Recent studies have proposed an alternative theory linking NF to injury-induced fibroblast proliferation and subsequent lesion formation. While some studies have suggested a potential link between NF and prior trauma, the majority of reported cases lack a clear etiology beyond such a history. 7 The occurrence of NF in the vocal cords is an infrequent phenomenon, particularly among people of advanced age. We herein present a case of NF in the vocal cords of a 75-year-old man who underwent surgical intervention at our institution.
Case report
Chief complaint
A 75-year-old man presented with a 1-month history of hoarseness, breathlessness, and a pharyngeal foreign body sensation.
History of present illness
One month before presentation, the patient had developed a foreign body sensation in the pharynx and hoarseness. He had also experienced an intermittent cough with production of white phlegm. He had no accompanying symptoms such as suffocation, difficulty breathing, or hemoptysis. Electronic laryngoscopy conducted at other medical institutions revealed a mass on the vocal cord, and subsequent surgical intervention was recommended. The patient sought further treatment at our hospital.
History of past illness
The patient had a 3-year documented history of hypertension and was undergoing oral administration of irbesartan hydrochlorothiazide tablets and lacidipine at the time of presentation. He had no evidence of prior trauma.
Personal and family history
The patient had no history of smoking, drinking, drug use, or blood transfusion. He had no family history of laryngocarcinoma.
Physical examination
Physical examination revealed pharyngeal hyperemia, grade I bilateral tonsil enlargement, and hyperplasia of lymphoid follicles in the posterior pharyngeal wall and root of the tongue. No significant swelling or elevation of the epiglottis was evident. No abnormalities were found in the external larynx, but recently developed lesions were detected on the surface of the right vocal cord during indirect laryngoscopy, resulting in glottic obstruction. Both vocal cords exhibited normal movement but poor closure. No obvious abnormalities were noted in the bilateral piriform fossae.
Laboratory examinations
No abnormalities were found on routine blood and urine tests, liver and kidney function tests, measurement of ion levels, measurement of coagulation parameters, and infectious disease screening.
Imaging examinations
Computed tomography (CT) revealed an occult nodule on the right vocal cord extending into the laryngopharynx, measuring approximately 15 × 12 × 9 mm and exhibiting a consistent density of approximately 24 Hounsfield units. Thickening of the right vocal cord at its point of attachment had caused localized stenosis and obstruction in the larynx. Furthermore, numerous small lymph nodes were present within the bilateral submandibular and cervical regions, along with one larger node measuring approximately 6 mm (Figure 1). Magnetic resonance imaging (MRI) demonstrated thickening of the right vocal cord with an irregular nodular abnormal signal shadow, protruding into the laryngeal lumen and measuring approximately 16 × 12 × 10 mm. T1-weighted imaging (T1WI) exhibited a hypointense signal, T2-weighted imaging (T2WI) showed a hyperintense signal, diffusion-weighted imaging displayed a hypointense signal, and apparent diffusion coefficient mapping demonstrated a hyperintense signal. The lamina of the right vocal cord exhibited high signal intensity, while local attachment of the tumor to the left vocal cord had resulted in stenosis and obstruction of the laryngeal lumen. Enhanced imaging depicted continuous and uniform enhancement; a small focal area of low signal intensity was observed in delayed scans, and clear parapharyngeal space delineation was evident. Unevenly hyperintense nodules were identified on T2WI within the left lobe of the thyroid gland, and slight hypointensity was noted on T1WI without clear dispersion; cross-sectional dimensions measured approximately 14 × 12 mm. Enhanced imaging revealed significant enhancement, and multiple lymph node shadows measuring up to 6 mm in diameter were detected within the cervical region (Figure 2).

Computed tomography imaging of vocal cord nodule. Computed tomography images show a nodule (arrow) on the right vocal cord extending into the laryngopharynx, measuring approximately 15 × 12 × 9 mm with consistent density of approximately 24 Hounsfield units corresponding the larynx.
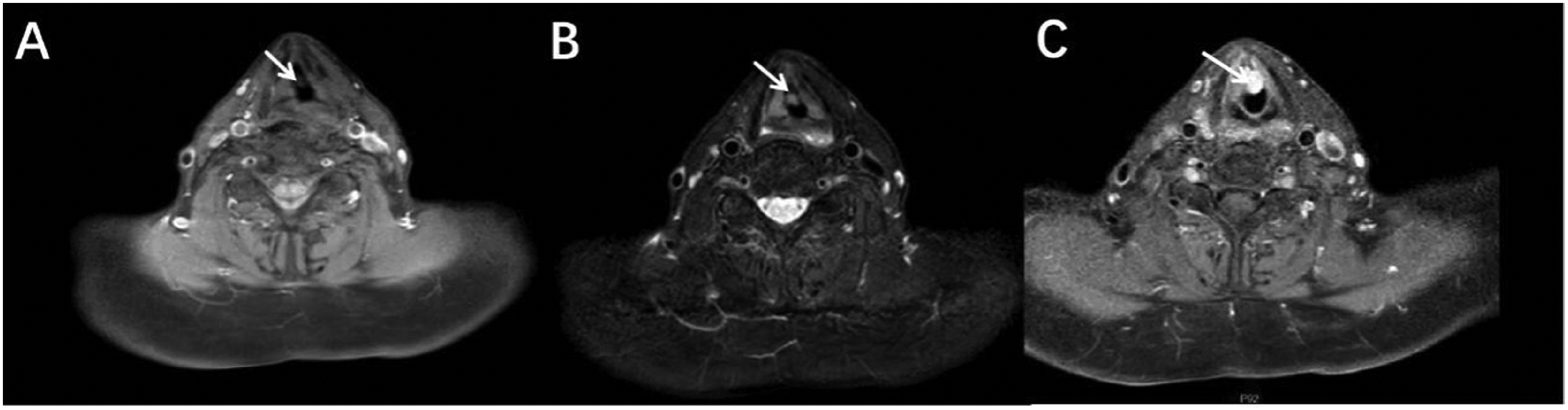
Magnetic resonance imaging of vocal cord nodule. (a) Axial fat-suppressed T1-weighted image shows hypointensity relative to muscle. (b) Axial fat-suppressed T2-weighted image shows hyperintensity and (c) axial enhanced fat-suppressed T1-weighted image shows notable enhancement (white arrow).
Electronic nasopharyngoscopy and pathological examination
Electronic laryngoscopy revealed hyperemia of the bilateral ventricular bands and vocal cords. Recently developed lesions were observed on the anterior middle third of the right vocal cord and the anterior commissure. No abnormal vasodilation was detected in the narrow band (Figure 3). Preoperative biopsy was performed using an electronic laryngoscope; the precise location of the biopsy is shown in Figure 3. The preoperative pathological examination revealed absence of a multilayered epithelium in the submitted tissue, along with surface necrosis, interstitial porosity and edema, mucoid strands, and chronic inflammatory cell infiltration. Immunohistochemical examination demonstrated negative staining for cytokeratin and P40, positive staining for CD34 in blood vessels, and positive staining for CD68 in histiocytes (Figure 4).

Laryngoscopic views and biopsy site. (a) Conventional laryngoscopy. (b) Narrow-band imaging electronic laryngoscopy and (c) biopsy site.

Histopathological and immunohistochemical findings. (a) Absence of multilayered epithelium in the submitted tissue, along with surface necrosis, interstitial porosity and edema, mucoid strands, and chronic inflammatory cell infiltration (hematoxylin–eosin staining, 10×) and (b) iImmunohistochemical staining of cytokeratin (−) and P40 (−), CD34 ((+) in blood vessels), and CD68 ((+) in histiocytes) (CD34 stain, 20×).
Treatment
After completing all examinations and excluding contraindications, we proceeded with preventive tracheotomy and plasma-assisted resection of the laryngeal masses using a supportive laryngoscope. Intraoperative findings revealed gray and white morular masses on the anterior two-thirds of the right vocal cord. These masses extended into the subglottis, laryngeal compartment, and anterior commissure and were characterized by a rough surface.
Postoperative pathology
On postoperative pathological examination, the epithelium on the tissue surface exhibited necrosis accompanied by an inflammatory exudate, fibrous tissue deposition, hyperplasia of small vessels, interstitial mucous braid formation, microcystic structure development, and extravasation of erythrocytes. In addition, scattered histiocytes and plasma cells were observed. The tumor was identified as a benign mesenchymal tumor with abundant mesenchyme content. Immunohistochemical analysis revealed positive staining for CD34 (in small vessels), smooth muscle actin (SMA), Ki67 (index: 10%), CD68 (a histiocytic marker), CD38 (a plasma cell marker), and CD99; negative staining for cytokeratin; and no expression of epithelial membrane antigen (EMA), STAT-6, Bcl-2, and S-100 proteins. Considering the clinical findings along with the immunohistochemical results, NF was suspected (Figure 5).

Postoperative pathological findings. (a) Hematoxylin–eosin staining, 10× and (b) hematoxylin–eosin staining, 10×.
Conclusive diagnosis and prognosis
The definitive diagnosis was laryngeal NF based on the patient’s medical history, physical examination, preoperative evaluation, and postoperative pathology. Laryngoscopic re-examination conducted 2 weeks postoperatively revealed mild bilateral vocal cord congestion with a smooth surface, indicative of postoperative changes. The movement of the vocal cords appeared normal, albeit with slightly compromised closure (Figure 6). The patient was still undergoing follow-up at the time of this writing.

Postoperative conventional laryngoscopy.
Discussion
The concept of NF, also known as pseudosarcomatous fibromatosis, was introduced by Konwaler et al. 8 in 1955. It is widely acknowledged as a self-limiting, reactive, and proliferative tumor-like lesion resulting from excessive growth of fibroblasts and myofibroblasts. 8 The occurrence of NF is predominantly observed in the upper extremities, followed by the trunk. However, there are reports of cases involving the head and neck region, including the eyelids, face, neck, mouth, parotid region, and other anatomical sites. In rare instances, NF may also manifest in uncommon locations such as the bladder, mammary gland, vulva, nerves, or joints; however, its occurrence in the vocal cords remains rare. We searched the literature regarding NF in the upper respiratory tract, and a summary of our findings is presented in Table 1. NF is commonly treated by local surgical excision. In some cases, observation of the lesions is adequate. With the exception of an 82-year-old woman with tracheal NF who was treated with symptomatic medical support for airway obstruction, 9 all other cases summarized in Table 1 were treated by surgical resection, and all had a favorable prognosis. NF occurring in the throat and respiratory tract is more suitable for surgical resection than NF in other locations.
Demographic characteristics and manifestations of six cases of nodular fasciitis in the throat and respiratory tract.
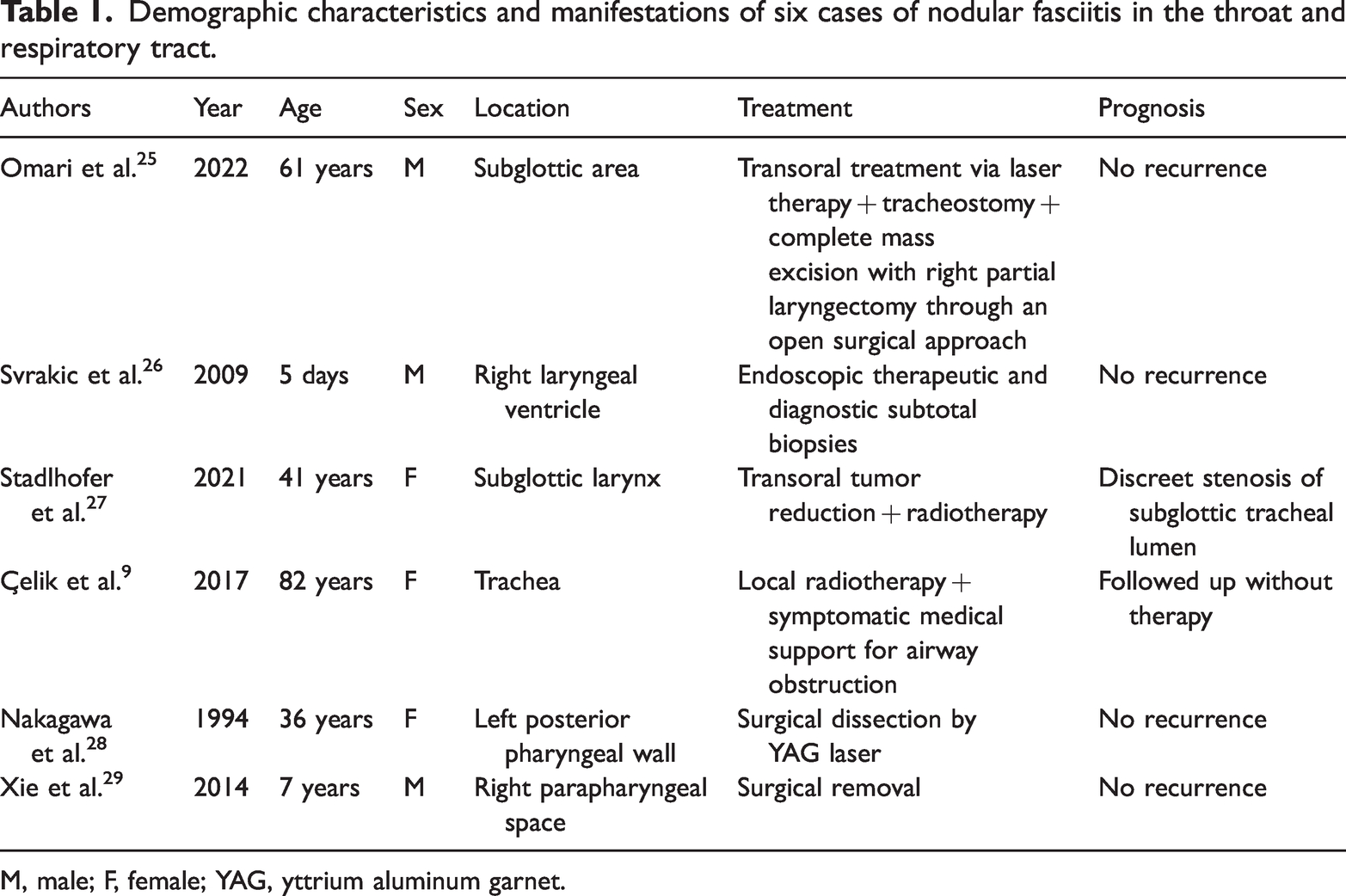
M, male; F, female; YAG, yttrium aluminum garnet.
NF is typically classified into three types depending on the site of occurrence: subcutaneous, fascial (intermuscular), and intramuscular. 10 Fascia-type lesions originating from the epimuscular membrane, which is located in close proximity to the skin, can be clinically classified as subcutaneous. The concept of superficial NF, as proposed by Lee et al., 11 refers to the occurrence of NF deep in the dermis and superficially in the muscles, encompassing subcutaneous and partial fascial forms. 11 Subcutaneous fasciitis is the most prevalent, occurring 3 to 10 times more frequently in the adipose layer of the dermis than in other regions. Most cases of subcutaneous NF are superficial, and they are treated by prompt resection of the lesion following clinical palpation. NF commonly manifests in musculoskeletal areas such as the forearm and lower extremities. 7 Intramuscular NF is characterized by the presence of large-diameter lesions located in deep tissue, often resembling soft tissue tumors. Fascial (intermuscular) NF manifests as an irregularly bounded lesion in the fascial plane, typically attached to the fascia and exhibiting an irregular growth pattern that extends into the subcutaneous fat. In some cases, the lesion originates from the fibrous septa of the subcutaneous fat and is solely associated with the fascia. The lesion is generally well-defined and lacks a distinct envelope. The pathogenesis of NF remains elusive. Its etiology has been linked to prior trauma in 5% to 10% of cases and is thought to involve a hyper-responsive mechanism that triggers an upregulation of mitotic activity in susceptible individuals. 7 The case presented herein involved a 75-year-old man with glottic involvement, which is an uncommon presentation in terms of both age and location. The patient denied any history of injury. The disease duration was 1 month, consistent with previously documented cases.
The diagnosis of NF is straightforward when the lesion is located in a common anatomical site and exhibits typical histological features. However, clinical misdiagnosis becomes more likely when the lesion occurs in an uncommon anatomical site. The primary clinical manifestations observed in this case were dysphonia, dyspnea, and a foreign body sensation in the pharynx. Diagnosis solely based on clinical manifestations and basic auxiliary examinations, such as electronic laryngoscopy, poses challenges and may lead to misdiagnosis of other neoplastic diseases. The occurrence of NF in the vocal cords is a rare phenomenon that presents cytological features similar to both benign and malignant tumors as well as granulomatous and inflammatory cytological features, resulting in difficult diagnosis. In this case, a preoperative biopsy was conducted using local anesthesia and an electronic laryngoscope. The pathological examination revealed necrosis, edema of the loose connective tissue, mucoid transformation, and chronic inflammatory cell infiltration on the tissue surface. However, a definitive diagnosis of NF could not be established. The preoperative pathological diagnosis was thus determined to be a vocal cord ulcer. We identified the following two factors that contributed to this pathological outcome. First, the patient exhibited poor cooperation during the biopsy procedure conducted under local anesthesia and electronic laryngoscope guidance, resulting in an unlabeled biopsy site that failed to penetrate the tumor substance. Second, few tissue samples were obtained, posing challenges for accurate pathological diagnosis. In addition, nodular granuloma of the vocal cord is a rare condition that can be easily overlooked during pathological examination. Therefore, NF of the vocal cords cannot be confirmed through puncture cytology. The diagnosis in this case was ultimately confirmed by the postoperative pathologic examination. The pathologic examination of NF revealed a significant presence of actively proliferating fibroblasts on a mucoid matrix in the central region, as well as localized capillary hyperplasia. Additionally, characteristic pathological features included the presence of wide ribbon-like or vortex arrangement of collagen fibers, deep nuclear staining, prominent nucleoli, and the absence of pathological nuclear division despite the occurrence of nuclear division. 12 The aforementioned pathological characteristics were confirmed in our case through light microscopy. However, distinguishing cases with infiltration and abundant cell and nuclear division from malignant tumors can present a challenge, leading to an incomplete diagnosis. Confirmation of the diagnosis requires additional immunohistochemistry in such cases. The expression of muscle-specific actin, SMA, and vimentin is typically positive, whereas the expression of S-100 protein, desmin, trypsin, factor VIII, macrophage-specific antigen, and HLA-DR1 is generally negative. Negative CD34 expression can be helpful in ruling out a sarcomatous nature of the lesion. NF may show positivity for CD-68 or KP-1, which are histiocyte-specific markers.7,13 In this case, immunohistochemical analysis revealed positive staining for CD34 (in small vessels), SMA, Ki67 (index: 10%), CD68 (histiocytic marker), CD38 (plasma cell marker), and CD99; negative staining for cytokeratin; and no expression of EMA, STAT-6, Bcl-2, and S-100 proteins. Immunohistochemistry is indispensable for confirmation of the diagnosis. Previous studies have documented instances of misdiagnosed cases of NF, attributing the main cause of misdiagnosis to the absence of immunohistochemistry during the pathological examination. 14 Although not explicitly specified, imaging findings play a pivotal role in the preoperative assessment of NF and other conditions, including neurogenic tumors, small salivary gland tumors, sarcoidosis, hemangioma, invasive fibromatosis, cutaneous fibroma, and malignant fibrous histiocytic cells. Tuberous fasciitis located on the surface is typically visualized as a well-defined soft tissue mass on CT and MRI. Intramuscular deep lesions often exhibit large dimensions with indistinct margins.15,16 MRI of NF exhibits a certain degree of correlation with histopathological types. Previous studies suggest that the MRI signal characteristics and enhancement patterns of NF are associated with the cellular composition, mucin content, collagen deposition, extracellular fluid distribution, and vascularity within the lesion. The myxoid and cellular lesions demonstrate equivalent signal intensity on T1WI, significantly high signal intensity on T2WI, and heterogeneous enhancement on contrast-enhanced scans. Fibrous lesions exhibit similar signal intensity on T1WI, slightly higher signal intensity on T2WI, and mild homogeneous enhancement on contrast-enhanced scans. However, because of the complex tissue composition of NF, these three components often coexist within the same lesion, posing certain challenges in MRI diagnosis. 17 In the present study, the pathological findings indicated the presence of myxoid NF. MRI typically exhibits a hypointense signal in T1WI and a hyperintense signal in T2WI, and enhanced imaging depicts continuous and uniform enhancement.
Clinically, tuberous fasciitis is frequently misdiagnosed as sarcoma or other malignant tumors because of its rapid growth, abundant cellular proliferation, and active mitotic activity. Several characteristic features of NF aid in its diagnosis, including its small size, well-defined margins, presence of mucoid stroma, and scattered red blood cells and lymphocytes. 12 The histologic differential diagnoses in the present case encompassed a range of both benign and malignant entities in the vocal cords. Differential diagnoses for benign tumors containing spindle cells include fibrous histiocytoma, pyogenic granuloma, postoperative/post-traumatic spindle cell nodule, myofibroma, and peripheral nerve tumor. Malignant tumors that must be ruled out include Kaposi sarcoma, spindle cell carcinoma, and spindle cell melanoma. 18 The typical histologic finding of NF is a haphazard arrangement of pleomorphic spindle cells in a myxoid matrix. Despite the high number of mitotic figures, atypia is rare. Immunohistochemically, NF is positive for vimentin (a fibroblast marker), actin (a smooth muscle marker), and histiocyte markers. In addition, NF shows a heterogenous appearance with myxoid, cellular, and fibrous areas. 19 Low-grade malignant myofibroblastoma sarcoma (LGMS) of the larynx is difficult to distinguish from nodular fasciitis of the vocal cords based on clinical features alone. Thus, both clinical features and pathological findings should be considered. Generally, LGMS cells exhibit atypia with less well-defined cytoplasmic borders and often thin filaments, which mainly run under the membrane and are parallel to the cell’s long axis. The nuclei of LGMS cells tend to be longer than those of smooth muscle cells and sharpened at both ends, often with pseudoneural-like curves (which reflect the contractile properties of the cells), finely granular chromatin, and frequently prominent nucleoli. The tumor cells of LGMS show a diffuse fascicular or storiform growth pattern and infiltrate surrounding tissues. As in NF cells, S-100 protein, laminin, desmin, and epithelial markers such as pan-cytoadhesin or EMA are not stained in LGMS cells. 20
The cases highlighted in this article serve as a poignant reminder: NF should be considered in patients with sudden onset of an isolated, rapidly proliferating mass or nodule on the vocal cord, typically measuring an average of 2 cm and rarely exceeding 4 cm in diameter. Preoperative pathology of biopsy specimens reveals ulceration, necessitating consideration of nodular granuloma of the vocal cord. The objective of this case report is to enhance clinicians’ comprehension of the infrequent incidence of NF in the vocal cords. With a more comprehensive understanding of this clinical entity, it is possible to prevent the delay caused by misdiagnosis or even avoid misidentifying the lesion as sarcoma, thereby minimizing unnecessary or debilitating surgical damage. As a benign hyperplastic lesion, NF only requires local surgical resection following diagnosis and does not necessitate additional treatments such as enlargement or radical surgery. The literature also suggests that nodular granuloma is a self-limiting condition that does not require surgical resection. Instead, it only necessitates regular follow-up observations, and spontaneous resolution can be expected within 4 to 8 weeks.21,22 The present case has also provided us with the following two insights. First, the possibility of NF should be considered in cases of solitary masses on the vocal cords with a brief duration of symptoms. Second, the management of NF in the vocal cords differs from that of other types of NF. Because of the rapid growth of NF and its potential to obstruct the glottis when manifesting as a large mass, acute dyspnea and even asphyxia can occur, making early resection of vocal cord masses under supportive laryngoscopy imperative. In addition, a watchful waiting treatment strategy may not be suitable for patients presenting with vocal cord NF. The previous literature reveals a recurrence rate of 1% to 2% for NF following surgical resection. 23 However, in this case, there was no evidence of postoperative recurrence in the present case, and the patient was still being monitored at the time of this writing.
Conclusions
NF of the vocal cords is a rare clinical entity that may manifest in older patients. This case report aims to enhance otolaryngologists’ comprehension of NF located within the vocal cords. The sole therapeutic approach for NF of the vocal cords is surgical resection.
The reporting of this study conforms to the CARE guidelines. 24
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241259764 - Supplemental material for Laryngeal nodular fasciitis in a 75-year-old man: a rare case report and review of the literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605241259764 for Laryngeal nodular fasciitis in a 75-year-old man: a rare case report and review of the literature by Yu Wen, Shufeng Ye, Cuiping Liu and Yiming Zhu in Journal of International Medical Research
Footnotes
Acknowledgements
We thank all individuals who participated in this study.
Author contributions
SY analyzed and interpreted the data. CL and YW performed operation and patient management. YZ consulted the relevant literature.
Data availability statement
All relevant data are within the manuscript and its additional files.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Ethics statement
This case report was approved by the Second People’s Hospital of Gansu Province Ethics Committee (approval no. 2023KYXM024), and the patient provided informed consent for treatment. The patient also provided written informed consent for publication of this case report in accordance with our institutional guidelines. A copy of the written consent can be made available upon request from the corresponding author. All identifiable patient details were removed before publication.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.