
Abstract
Giant vocal cord polyps pose challenges in airway management, particularly in patients with severe obstructive sleep apnea–hypopnea syndrome. We present the case of a morbidly obese man in his 20s (body mass index: 50.8 kg/m2) with severe obstructive sleep apnea–hypopnea syndrome and a giant vocal cord polyp. He successfully underwent awake tracheal intubation using video laryngoscopy and high-flow nasal oxygen, which was administered at 30 L/min. Airway anesthesia was achieved with lidocaine, including bilateral superior laryngeal nerve blocks. A 6.5-mm endotracheal tube was placed within 30 s, maintaining the peripheral capillary oxygen saturation level at 100%. The patient remained cooperative and spontaneously breathing throughout the procedure. No complications were observed postoperatively, and the patient was discharged the following day. This case illustrates the effectiveness of awake tracheal intubation and provides valuable insights into managing complex airway cases.
Keywords
Introduction
Vocal cord polyps are benign growths causing hoarseness, with a higher prevalence observed in male smokers. 1 Although most of these polyps are small and easily treatable, giant polyps may also occur, which can cause severe airway obstruction and potentially life-threatening complications.2,3 These giant polyps or other airway-obstructing lesions may mimic the clinical manifestations of obstructive sleep apnea–hypopnea syndrome (OSAHS) or asthma, potentially leading to misdiagnosis until the actual condition is identified through laryngoscopy.4,5 This diagnostic challenge, along with the mechanical risk of obstruction, makes airway management particularly difficult in such cases.
Awake tracheal intubation (ATI) is a recommended strategy for patients at high risk of airway obstruction, 6 as it facilitates effective airway management while the patient remains conscious and spontaneously breathing. This approach is particularly beneficial in patients with severe OSAHS, as it prevents upper airway collapse that can occur after induction. In addition, the use of high-flow nasal oxygen (HFNO) during ATI reduces the risk of desaturation by providing continuous humidified oxygen and airway pressure. This decreases respiratory effort, enhances comfort, and increases the chance of successful intubation. 7 This report describes the case of a successful ATI with HFNO support in a morbidly obese patient with a giant vocal cord polyp and severe OSAHS.
Case description
A man in his 20s, who was a heavy smoker (weight: 157.4 kg, height: 176 cm, body mass index: 50.8 kg/m2), was admitted to our hospital in November 2024 because of hoarseness, snoring, witnessed apneas, and daytime sleepiness. Polysomnography confirmed severe OSAHS with an apnea–hypopnea index (AHI) of 50.31, mean oxygen saturation of 89.03%, and minimum oxygen saturation of 50.18%. Airway assessment showed a modified Mallampati grade of II, a mouth opening of 4 cm, a thyromental distance of 6.5 cm, and normal neck mobility. Flexible rhinolaryngoscopy revealed the presence of a giant cord polyp on the left vocal cord (Figure 1), and magnetic resonance imaging (MRI) revealed that the polyp measured approximately 16 mm × 18 mm (Figure 2).
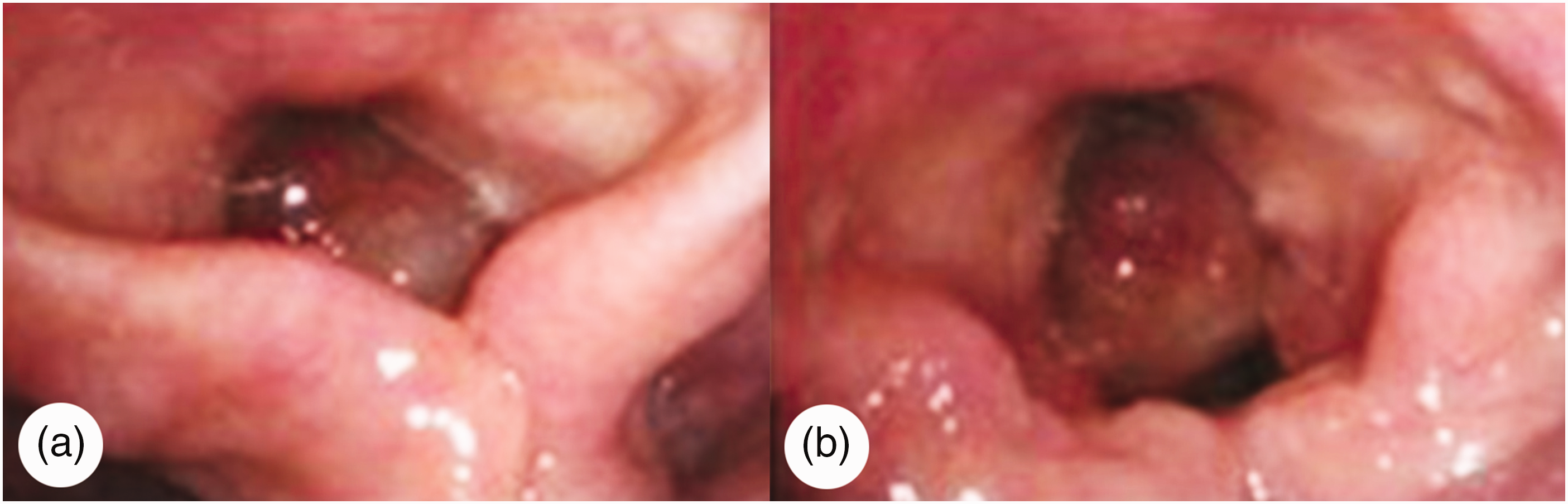
(a) The polyp almost covers the glottic area during inspiration and (b) moves away from the glottis, revealing a small gap during expiration.
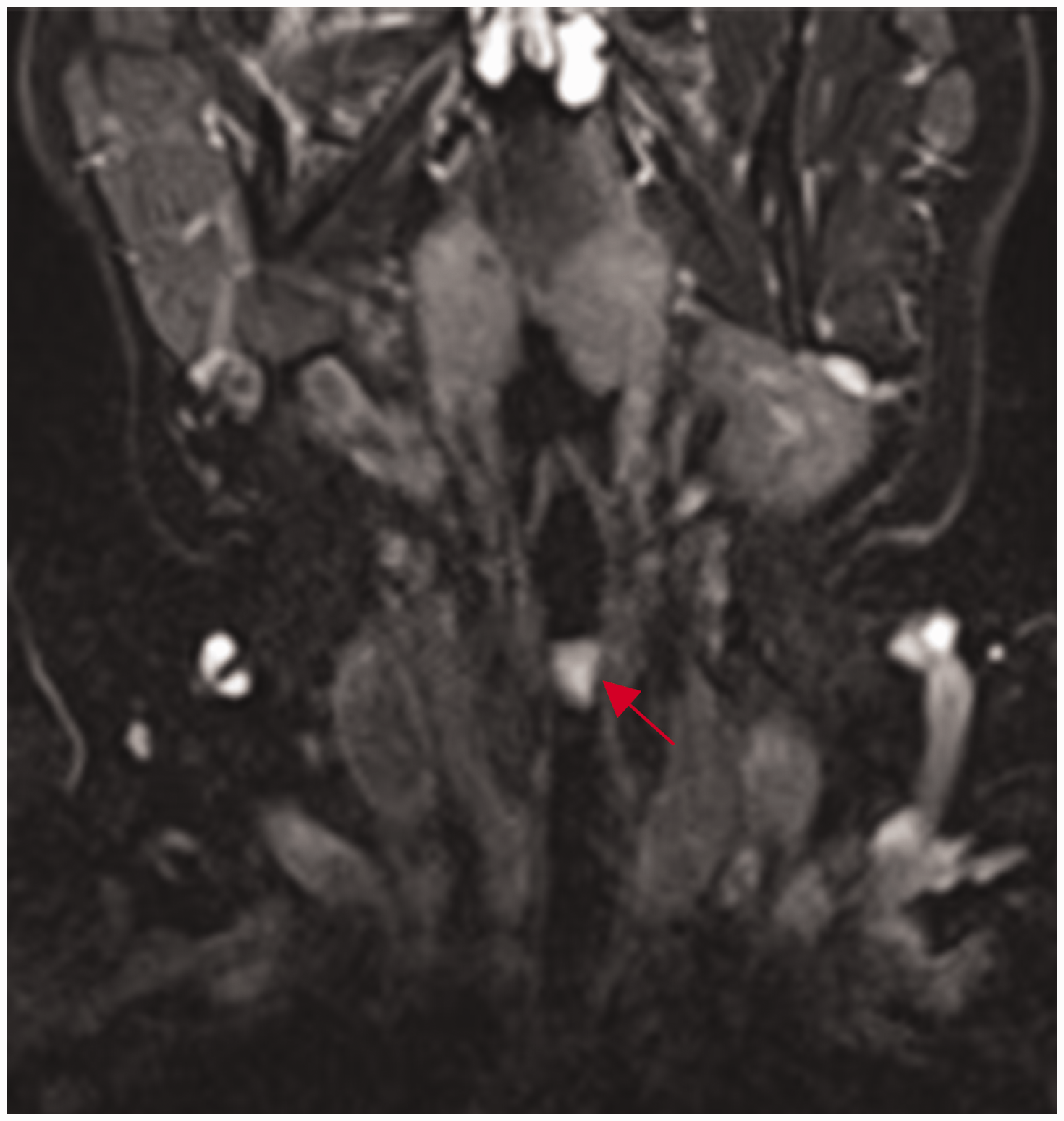
MRI of the neck revealed a giant vocal cord polyp on the left vocal cord, measuring 16 mm × 18 mm, causing significant glottic airway narrowing. MRI: magnetic resonance imaging.
Given the complexity of the patient’s condition, a multidisciplinary team developed a comprehensive treatment plan and perioperative emergency protocols. ATI was performed using video laryngoscopy (VL) as an airway management strategy, supplemented with HFNO and effective airway topicalization. In the event of failed intubation or airway obstruction, cricothyrotomy or emergency tracheostomy would be immediately available.
Prior to surgery, the patient was premedicated with 30 mg of ketorolac and 0.5 mg of penehyclidine hydrochloride intravenously. In the operating room, standard monitors were applied. He was placed in the “sniff” position (Figure 3), maintaining a peripheral capillary oxygen saturation (SpO2) level of 93% while being awake and breathing room air. HFNO was administered at 30 L/min, and sedation was achieved by infusing remifentanil (0.02 mcg/kg/min) and propofol (5 mcg/kg/min) for approximately 30 min, maintaining the SpO2 level at 100%.

A morbidly obese patient is placed in the “sniff” position.
The patient was first instructed to open the mouth widely. A tongue depressor was used to apply 4 mL of 2% lidocaine sequentially to the oral cavity, oropharynx, and larynx via a spray catheter. Bilateral internal branch blocks of the superior laryngeal nerves were performed under ultrasound guidance, using a parasagittal approach and 2 mL of 1% lidocaine on each side. With the assistance of VL and a homemade simple spray pipe (Figure 4), 5 mL of 2% lidocaine was sprayed onto the base of the tongue, epiglottis, and glottis, followed by 4 mL of 2% lidocaine injected through the cricothyroid membrane. Then, VL was used to visualize the glottis, revealing a giant polyp covering 85% of the glottic area. A 6.5-mm endotracheal tube was successfully inserted during exhalation within 30 s, with the SpO2 level maintained at 100%. After confirming the correct position of the endotracheal tube, 100 mg of propofol and 60 mg of rocuronium were administered intravenously, and 1.5% sevoflurane was inhaled. To maintain anesthesia, propofol (18 mcg/kg/min) and remifentanil (0.03 mcg/kg/min) were continuously infused intravenously. The surgery was completed without complications (Figure 5). Postoperative follow-up revealed no memory of the procedure and no pharyngeal or laryngeal discomfort. The patient was discharged the following day. A 1-month telephone follow-up indicated resolution of the hoarseness, although significant OSAHS-related symptoms persisted.
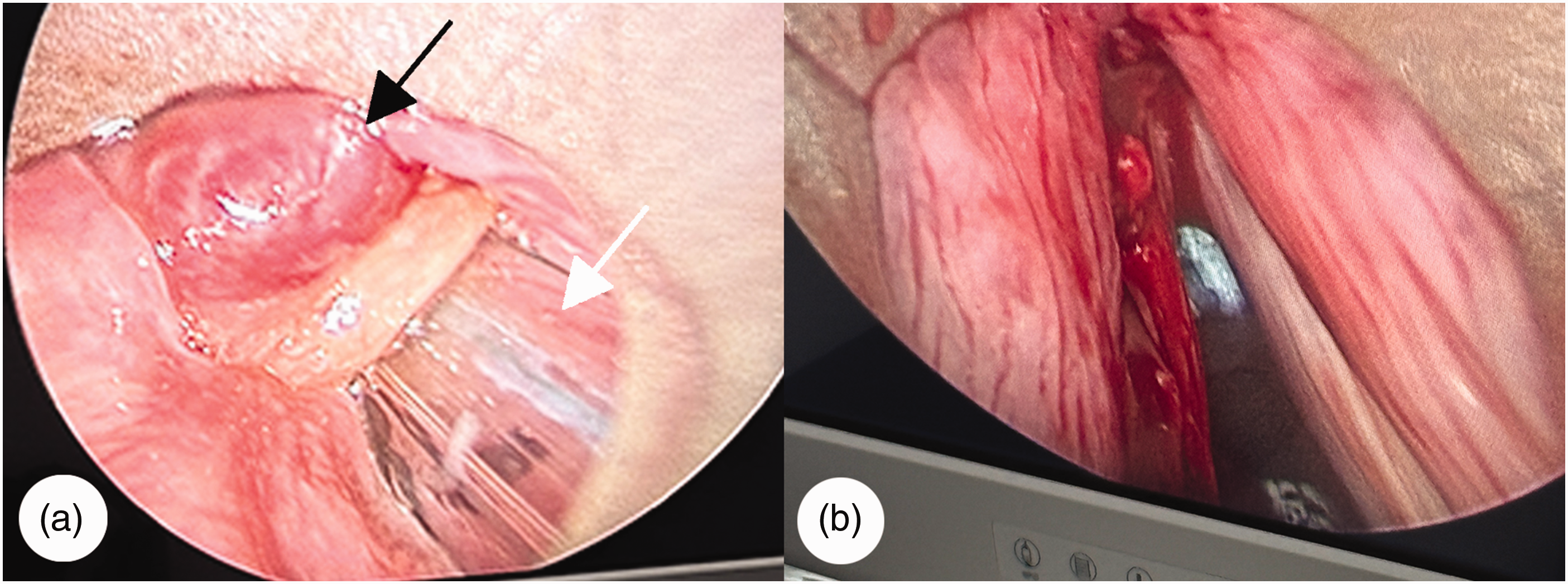
Surgical treatment of the patient. (a) Intraoperative view at the start of surgery using a video-assisted self-retaining laryngoscope. The black arrow indicates the glottic mass, and the white arrow indicates the endotracheal tube and (b) an intraoperative image captured near the end of surgery, demonstrating substantial removal of the glottic mass.
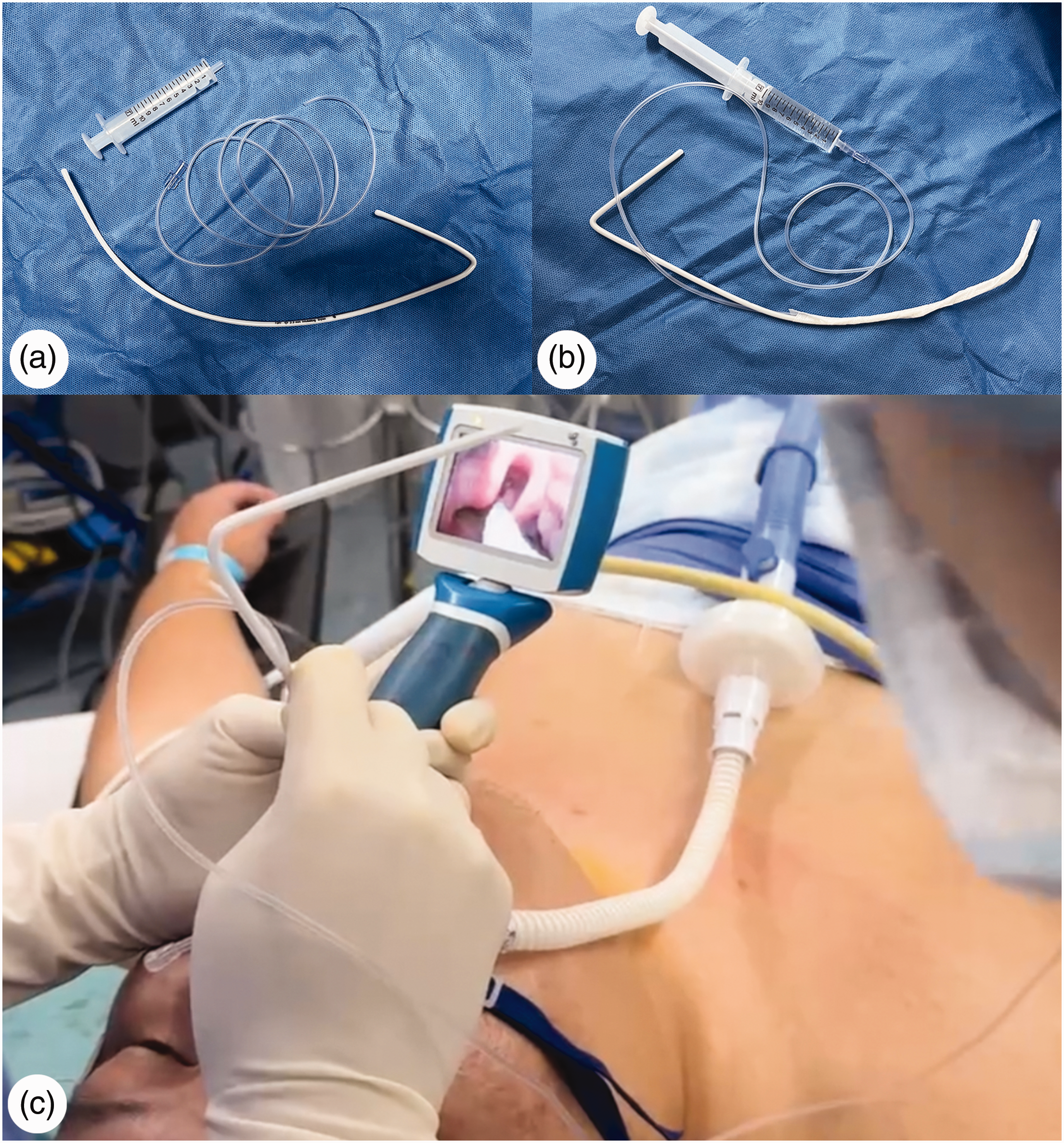
(a) A homemade simple spray pipe comprises a syringe, a stylet, and a catheter. (b) One end of the catheter connects to the syringe containing local anesthetic, while the other end of the catheter is taped to the stylet and (c) Under the guidance of a video laryngoscope, the spray pipe delivers the anesthetic spray precisely to the target airway structures.
The patient provided informed consent for publication of this case. This case report adheres to the Case Report (CARE) guidelines. 8 The patient’s data have been de-identified. Patient consent to treatment was also obtained.
Discussion
We conducted a Web of Science search using the keywords “vocal cord polyp” or “mass” and “OSAHS” or “obesity” in relation to ATI case reports. No studies were found that address the combination of severe OSAHS, morbid obesity, and vocal cord polyps. To the best of our knowledge, this is the first report focusing on airway management in such a patient.
In morbidly obese patients with a giant vocal cord polyp, the risk of airway management complications during the perioperative period increases significantly. Guidelines recommend ATI when a difficult airway is present. 6 To ensure successful ATI, the “sTOP” approach, comprising sedation, topicalization, oxygenation, and performance, 9 plays a crucial role. This approach was effectively applied in this case.
Sedation is not essential for performing ATI, but it can be a valuable adjunct to facilitate the procedure. Studies on nonsedated volunteers have shown that ATI can be tolerated satisfactorily without sedation. 10 However, in clinical practice, sedation is often employed to reduce patient anxiety and improve tolerance of the procedure. 11 In morbidly obese patients with airway complications, such as OSAHS, sedation during ATI may pose several risks, including rapid oxygen desaturation and respiratory depression. 12 Therefore, the choice of sedative agents is critical to managing these risks. Both propofol and remifentanil are well-established, effective, and safe sedatives for ATI.13,14 Remifentanil, in particular, was selected due to its potent analgesic and antitussive properties as well as its rapid onset and quick recovery, which are essential for controlling airway reflexes during ATI. 15 Given the patient’s morbid obesity and severe OSAHS, continuous monitoring of respiratory parameters, including oxygen saturation and airway patency, was conducted throughout the sedation process. We carefully titrated the doses of both agents, ultimately using a low-dose combination of remifentanil and propofol, which safely and successfully facilitated the ATI procedure.
Effective localization is crucial to the success of ATI. Lidocaine is the most commonly used local anesthetic drug for airway management, with a recommended dose not exceeding 9 mg/kg based on lean body mass. 16 To enhance the efficacy of the anesthesia, we developed a simple yet efficient homemade spray pipe for precise lidocaine application. This homemade device can be easily constructed using commonly available materials. In addition, ultrasound-guided bilateral superior laryngeal nerve block reduces intubation time and improves intubation conditions. 17
HFNO is the preferred oxygenation method for ATI. Studies have shown that under low-flow oxygen (<30 L/min), the incidence of desaturation (SpO2 level ≤90%) ranges from 12% to 16%, whereas under HFNO (30 L/min), the desaturation rate decreases to 0%–1.5%.11,18 Given the patient’s severe OSAHS, a giant vocal cord polyp, along with an SpO2 level of only 93% while awake, we chose to administer HFNO at 30 L/min. As anticipated, the SpO2 level remained at 100% during the procedure, and successful intubation was achieved on the first attempt.
Flexible bronchoscopy (FB) is commonly regarded as the preferred modality for difficult airway management due to its distinct advantages. 19 FB is independent of mouth opening limitations and offers flexibility in using both nasal and oral routes, which generally enhances patient tolerance.20–22 However, FB has several limitations. It requires greater technical skill and a longer learning curve, with proficiency typically achieved after 25 intubations. 23 Additionally, FB can be challenging when dealing with large laryngeal lesions or complex airway anatomy. 24 In contrast, VL is more widely used in clinical practice, as it is simpler to operate and has a shorter learning curve. The VL blade is particularly effective in displacing large laryngeal lesions and overcoming airway navigation challenges that may be encountered with FB. Furthermore, VL provides direct visual guidance for ATI, unlike FB, which typically relies on blind tube advancement. VL also offers comparable first-attempt success rates to FB. 20 In this case, we performed ATI using VL, considering the patient’s excellent cooperation and favorable laryngoscopic view following proper airway anesthesia. The procedure was successful on the first attempt. However, the potential risks of VL should be considered, particularly the mechanical traction exerted on the tongue and supraglottic structures. This traction can increase pharyngeal stimulation, potentially provoking a gag reflex, emesis, or laryngospasm, which may compromise intubation success. 25 In cases where these complications arise, alternative strategies such as conversion to asleep VL intubation, awake fiberoptic intubation, or other airway management techniques should be considered. 26 Maintaining spontaneous ventilation and oxygenation is crucial during such transitions. In anticipated difficult airway scenarios, the choice of intubation equipment should be individualized based on patient factors and operator expertise. 19 Recent reports, such as the study by Yang et al., 27 have demonstrated the successful use of a Disposcope endoscope for ATI in older patients with large vocal cord polyps, highlighting the need for personalized airway management strategies.
An emergency airway management plan should always be established prior to anesthesia induction, even when the procedure is anticipated to proceed smoothly. In the event of glottic obstruction, mask ventilation difficulty, or failed intubation, emergency airway access (e.g. cricothyroid puncture or tracheotomy) should be promptly performed, with an otolaryngologist available for intervention and tube ventilation.
In conclusion, this case highlights the successful use of ATI, HFNO, and a homemade spray pipe in a morbidly obese patient with OSAHS and a giant vocal cord polyp, expanding the options available for similar challenges.
Footnotes
Acknowledgements
We sincerely thank the patient who participated in this study.
Authors’ contributions
Tieshuai Liu collected the data and wrote the manuscript; Du Zheng participated in the treatment and management of the patient; Ziming Zhang polished the manuscript; and Qing Qiao conceptualized the idea and revised the manuscript. All authors have read and approved the final version of this manuscript.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images.
Declaration of conflicting interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study received ethical approval from the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine (approval No.2025-0304), and adhered to the Declaration of Helsinki principles. Participant consent was obtained prior to data collection.
Funding
This report was supported by grants from Zhejiang Province Medical and Health Science and Technology Plan Project (2021455433).