
Abstract
We report a case that presented as acute myocardial infarction (AMI) caused by lymphocytic myocarditis (LM), and explore the relationship between AMI and LM. We also performed a literature search to identify publications that previously reported LM-associated myocardial infarction. Coronary angiography of our patient revealed normal coronary arteries. However, a perfusion–metabolism mismatch in the apex and mid-inferior walls supported the diagnosis of AMI, and right ventricular septal endomyocardial biopsy showed LM. Extensive viral serological tests were negative for an infectious etiology. Immunosuppressive therapy may be beneficial in patients with high-risk myocarditis who are pathologically confirmed to be virus-negative.
Keywords
Introduction
Making a diagnosis of myocarditis remains relatively difficult for most clinicians. Acute myocarditis has no specific symptoms, and its clinical manifestations are diverse. While it may be asymptomatic, it can also present with chest pain, acute heart failure that mimics acute myocardial infarction (AMI), heart conduction block, and even sudden cardiac death. 1 We present a case of chest tightness misdiagnosed as AMI but referable to a lymphocytic myocarditis (LM) with an unexplained electrocardiogram (ECG) in a 63-year-old woman over 24 hours after her hospitalization. ECG findings revealed the presence of localized ST segment elevation in the high lateral (I, aVL), inferior (II, aVF), and precordial leads (V2–V6). The study was approved by Fuwai Hospital (no. 20220116), and the patient provided written informed consent for participation and publication of the study.
Case report
A 63-year-old woman was admitted to her local emergency department with tightness of the chest. Although she had risk factors for atherosclerosis, including hypertension and hyperlipidemia, she had no history of coronary artery disease, had not experienced any stressful events (except for hyperthermia 2 weeks previously), and had no fever, suspicious viral infections (Coxsackie, adenovirus, influenza virus, parainfluenza virus, measles virus, mumps virus, encephalitis virus, hepatitis virus, herpes zoster virus, human immunodeficiency virus, cytomegalovirus, or severe acute respiratory syndrome coronavirus 2), or elevated inflammation markers. Twenty-four hours before her presentation, she reported persistent chest tightness, but this complaint was not addressed at the time.
Upon arriving at the hospital, her heart rate was 88 beats/minute with an arrhythmia, her blood pressure was 124/64 mmHg, auscultation detected no heart murmurs, and she had no symptoms or indications of acute heart failure. Her ECG suggested diffuse ST elevation on the inferior, high lateral, and anterolateral leads (Figure 1a), and showed tombstone-like changes. Her troponin I level was also elevated (24.3 µg/L). Based on these test results, she was diagnosed with AMI. She received double antiplatelet therapy, including aspirin and clopidogrel. Urgent selective coronary angiography showed no obstructive coronary disease or evidence of acute plaque rupture or coronary spasm (supplementary material online, video files A–D). She had a normal left ventricular systolic function with an ejection fraction (EF) of 76%, and transthoracic echocardiography showed the disappearance of wall motion in the apical segment. Stress-induced cardiomyopathy was suspected because of her recent history of heat stroke. On the third day after admission, repeat ECG (Figure 1b) and transthoracic echocardiography showed no major changes.
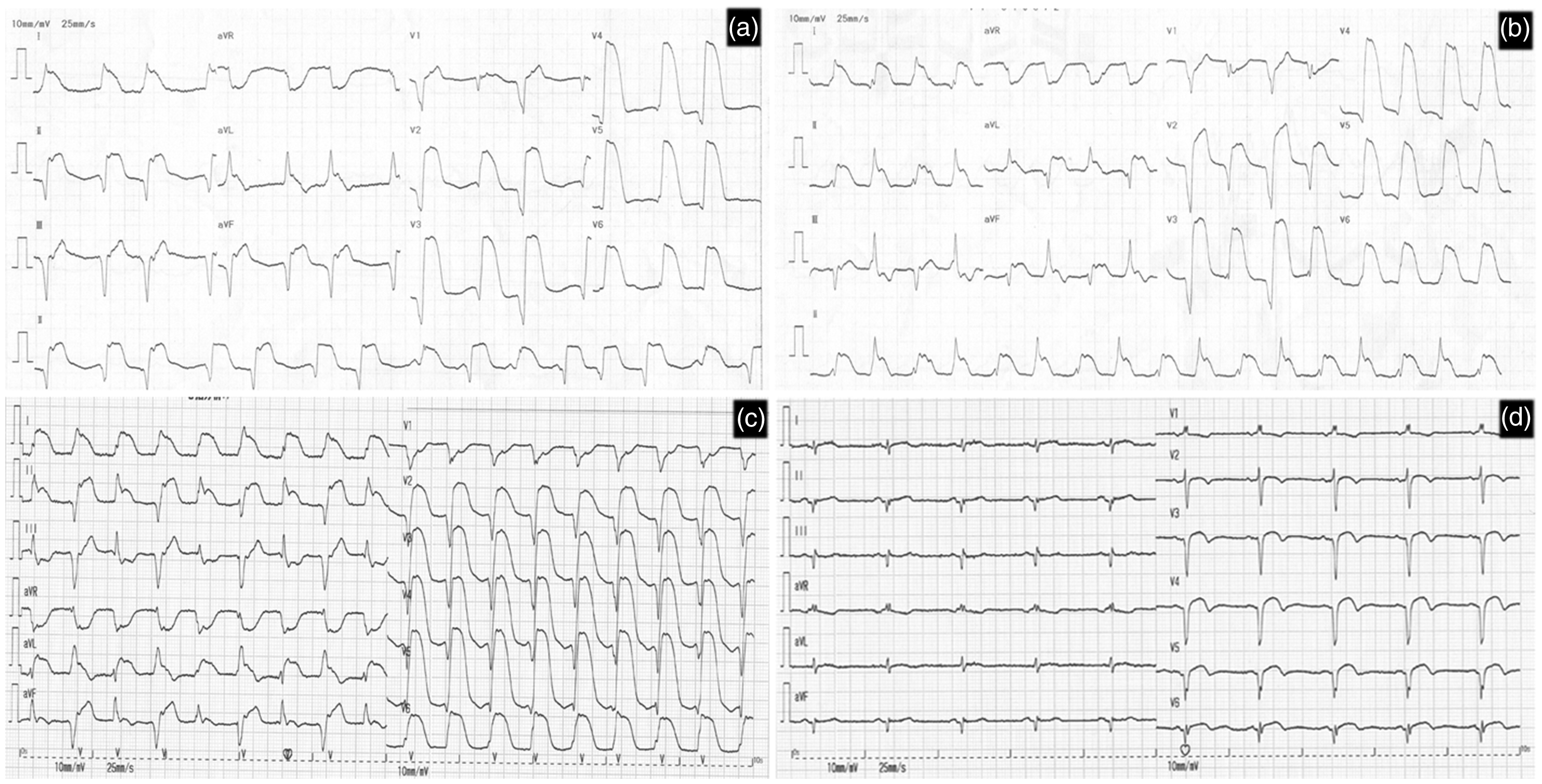
Echocardiography at the first visit to a local hospital (a), on the third day at a local hospital (b), on admission to our hospital (c), and at the time of discharge (d).
At that point, the patient was transferred to our hospital. She still had arrhythmia with a heart rate of 100 beats/minute and her blood pressure was 115/67 mmHg, although there were no other symptoms. Her ECG remained similar to the previous one (Figure 1c), and troponin I levels were elevated (9.19 ng/ml). She had normal hepatic transaminase and renal functions; her pro-brain natriuretic peptide level was 1395 ng/L, her erythrocyte sedimentation rate was 11 mm/hour, and C-reactive protein levels were 10.8 mg/L. Because she was stable, we promptly performed an electrophysiological evaluation of tachycardia using transesophageal pacing and recording which revealed accelerated idioventricular rhythms accompanied by premature ventricular beats. Cardiac magnetic resonance imaging (MRI) showed a reduction of the anterior wall and apical perfusion in the myocardial first-pass perfusion, obvious transmural enhancement in delayed imaging, and an oval-shaped low signal in the left ventricular apical region (Figure 2). Although she had suffered heat stroke 2 weeks previously, cardiac MRI did not support Takotsubo cardiomyopathy. Repeat echocardiography suggested no change in her left ventricular function, but a new thrombus was found in the apex; thus, low molecular weight heparin was administrated. AMI was confirmed by radionuclide cardiac imaging (Figure 3). Based on these findings, it was suspected that myocarditis was causative of AMI. Histopathological examination of the endomyocardial biopsy of the right ventricle (RV) showed active LM, with mainly CD3+ lymphocytes, and no eosinophils or giant cells (Figure 4). Evaluation for infectious etiology, including a serum virus test, was negative. The patient did not receive antiplatelet therapy after admission to our hospital because her AMI was not caused by coronary atherosclerosis. Three days after admission, her ECG had not improved much, so methylprednisolone 2 mg/kg/day (120 mg/day) was initiated. During the following 2 days, she recovered sinus rhythm and, subsequently, the persistent ST segment elevation gradually declined to a normal level. However, the R wave on the surface ECG (precordial leads) did not recover (Figure 1d).

CMR myocardial perfusion displaying low perfusion of the anterior wall and left ventricular apex. Gadolinium-enhanced findings show obvious transmural reinforcement in the left ventricular apex and right ventricular apex. An elliptical low signal is attached to the left ventricular apex without reinforcement.

Myocardial nuclear imaging revealing perfusion–metabolism mismatch in the apex and mid-inferior wall.

Histopathological examination of the endomyocardial biopsy. Positive T lymphocytes shown by CD3+-positive staining (a) and (b) CD68+-positive staining (b); original magnification ×20. Diffuse inflammatory cell infiltrates and myocyte necrosis shown by hematoxylin–eosin staining; original magnification ×50.
Discussion
The diagnosis of myocarditis remains a challenge because of its diverse clinical manifestations, 2 and the possible differential diagnosis of AMI. Myocarditis is often associated with chest pain; however, patients may also experience angina-like symptoms, although there is no coronary stenosis. Elevated serum creatine kinase and troponin are common, along with ECG changes (ST segment elevation in precordial leads, T wave inversion, and pathologic Q waves) which mimic AMI. Additionally, some patients who present with AMI with a typical history and ECG changes have normal coronary arteries, and are differential diagnoses of severe aortic stenosis, hypertrophic obstructive cardiomyopathy, Takotsubo cardiomyopathy, or vasculitis.3,4 Under these circumstances, it is difficult for clinicians to make a precise diagnosis. Clinicians should suspect acute myocarditis in patients who present with chest pain but whose ECG localization diagnosis is not compatible with AMI, and when there is no abnormal segmental wall motion on echocardiography.
We report an interesting case that met both the diagnostic criteria for AMI and those for active, virus-negative, immune-mediated myocarditis proposed by the World Health Organization.5,6 The AMI was focal in nature and there was no obvious enhancement in the RV wall. Hence, the RV endomyocardial biopsy yield was low, as expected, and could not rule out myocarditis. Such biopsies may be negative for selective bias. The exact etiology of AMI is still unclear; however, a recent study indicated that LM can cause AMI by promoting atherosclerotic plaque instability. 7 This hypothesis is supported by observations of increased lymphocytes in the atherosclerotic plaques of patients with LM diagnosed with AMI. Additionally, lymphocytes have been associated with the destabilization of plaque.8,9
In the present case, in contrast to previous studies, urgent selective coronary angiography showed no plaque in the coronary artery, and ST segment elevation lasted more than 1 week. Moreover, the observed ECG changes have rarely been seen before. McCully et al. reported that a 40-year-old woman diagnosed with LM had co-occurring AMI caused by coronary vasospasm. 10 The presence of intravascular thrombi in LM patients with AMI suggests the involvement of hypercoagulability. In our case, we postulate that the coronary artery spasm and/or thromboembolism resulted in AMI. This case is a reminder to clinicians that LM and AMI can co-occur, and that LM can play a key role in the pathogenesis of AMI.
The role of immunosuppressants in the treatment of myocarditis is still controversial, especially in terms of indications, timing of application, and duration of treatment. One study suggested that immunosuppressants should not be used routinely in myocarditis. 11 However, most European researchers who specialize in myocarditis believe that immunosuppressants can be considered on an individualized basis if there are no contraindications, especially for refractory infection-negative myocarditis. 2 In the current case, after 1 week of standard treatment, ongoing tombstone-like electrocardiographic changes indicated AMI. Glucocorticoid treatment was then initiated, and electrocardiography greatly improved soon after. Although we cannot rule out the possibility of self-healing, persistent ST segment elevation did not improve following administration of the optimal treatment. We followed up with the patient by telephone at 3 and 6 months after discharge, and determined that she had no major symptoms when performing daily activities. After that, her contact details changed and we were unable to reach her.
The reporting of this study conforms to CARE guidelines. 12
Conclusion
Current evidence does not support the routine use of immunosuppressants for patients with myocarditis. However, for those high-risk patients who are virus-negative, a combination of immunosuppressants is likely to be beneficial. In the current case, it was not clear whether the patient should have received dual antiplatelet therapy and for how long. Therefore, more evidence is needed regarding when, how, and for how long immunosuppressive therapy should be used for patients with AMI. Future research should focus on the translation of these problems into clinical outcomes.
Supplemental Material
sj-jpg-1-imr-10.1177_03000605221108933 - Supplemental material for Lymphocytic myocarditis presenting as acute myocardial infarction: a case report and review of the literature
Supplemental material, sj-jpg-1-imr-10.1177_03000605221108933 for Lymphocytic myocarditis presenting as acute myocardial infarction: a case report and review of the literature by Zhiwei Huang, Guangxun Feng and Yan Liang in Journal of International Medical Research
Footnotes
Acknowledgements
We acknowledge Dr. Yue Tian for the echocardiography evaluation, Dr. Minjie Lu for the magnetic resonance evaluation, and Dr. Yuehong Wang for help with pathological analysis.
Declaration of conflicting interest
The authors report no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.