
Abstract
Coexistence of pulmonary embolism (PE) and arterial thrombosis in a single patient is rare. Management of such cases is challenging because there is no unified standard on how to treat this type of disease. We herein report a case involving a 73-year-old man who was admitted to the hospital because of a 2-day history of chest tightness. Pulmonary computed tomography angiography revealed a filling defect of the main pulmonary artery and bilateral branches as well as a left subclavian artery embolism. AngioJet mechanical thrombectomy (Boston Scientific, Marlborough, MA, USA) was used to treat the PE, and this was combined with left brachial artery incision and thrombectomy for treatment of the left subclavian artery embolism. The patient recovered well after the operation. The prognosis was good after 9 months of regular follow-up. AngioJet mechanical thrombectomy combined with left brachial artery incision thrombectomy may be a feasible treatment option for cases of PE combined with left subclavian artery embolism.
Keywords
Introduction
Coexistence of pulmonary embolism (PE) and arterial thrombosis in an individual patient is rare. 1 More commonly reported situations involve patients with potential arteriovenous shunts, such as patent foramen ovale, atrial septal defect, or pulmonary arteriovenous fistula. An embolus that enters the systemic circulation from the right heart system is called a paradoxical embolism. 2 Patients with acute PE combined with paradoxical embolism have critical illness and high mortality. 3 Management is challenging because there is no unified standard on how to treat this type of disease. The patient reported herein had intermediate- to high-risk PE. Moreover, the end of the left subclavian artery thrombosis in this patient extended to the aortic arch.
The patient provided written consent for treatment. The patient also provided written consent for publication of this report. The requirement for approval by an ethics committee or institutional review board was waived because of the nature of this study (case report). The reporting of this study conforms to the CARE guidelines. 4
Case report
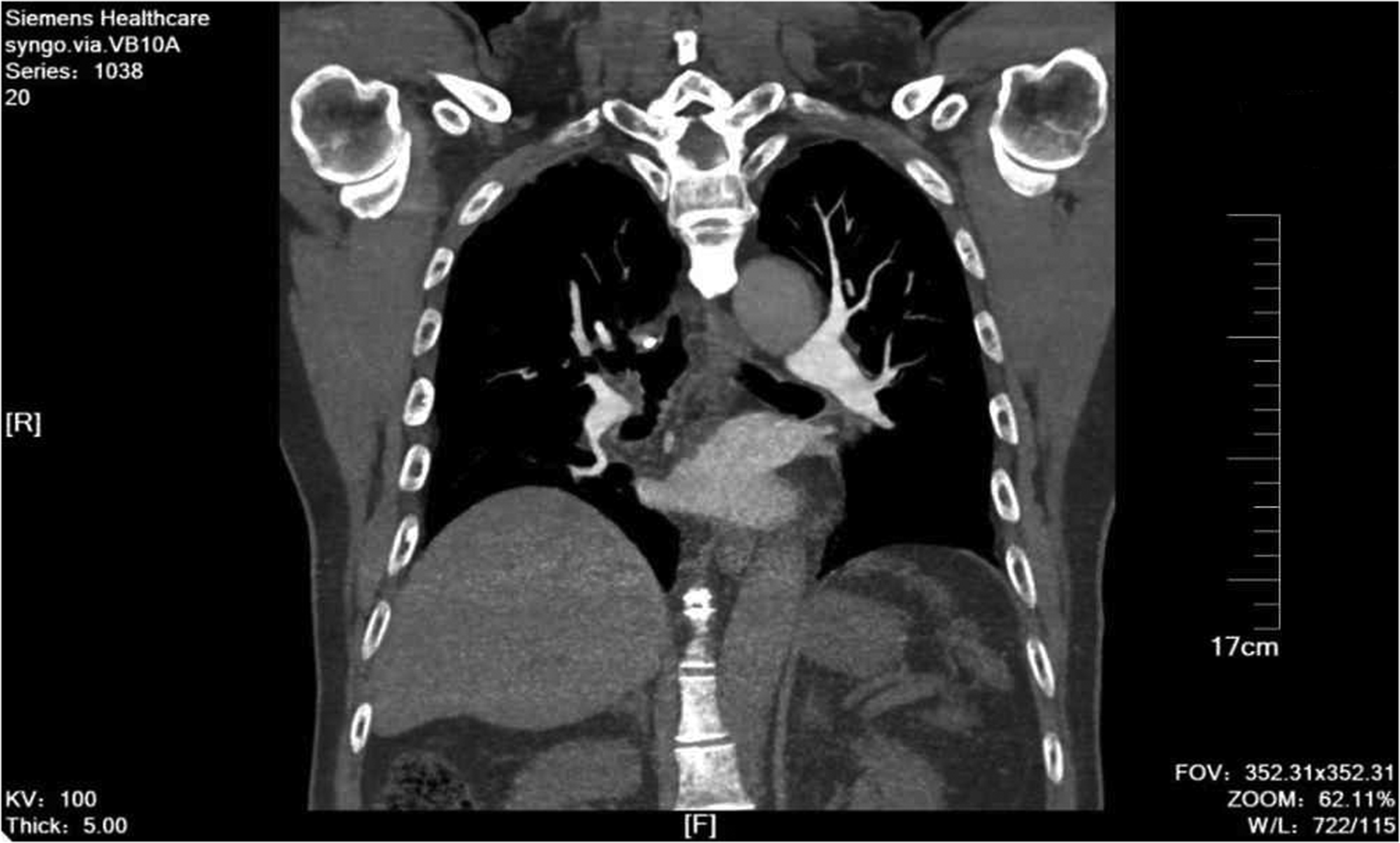
The patient was a 73-year-old man with a history of chronic obstructive pulmonary disease and atrial fibrillation. He was admitted to the hospital because of a 2-day history of chest tightness. Physical examination revealed a heart rate of 127 beats/minute, blood pressure of 184/107 mmHg, and oxygen saturation of 94%. Laboratory examination showed that his troponin concentration was 2.59 ng/mL (reference range: 0.012–0.034 ng/mL). Cardiac color Doppler ultrasound showed that the inner diameter of the right ventricle was 37 mm (reference range: 33–43 mm), the inner diameter of the right atrium was 41 mm (reference range: 29–45 mm), closure of the tricuspid valve was incomplete, the inner diameter of the left ventricle was 38 mm (reference range: 35–56 mm), the inner diameter of the left atrium was 31 mm (reference range: 19–40 mm), and the systolic pressure of the pulmonary artery was 50 mmHg. The right/left ventricular ratio was 0.97. Pulmonary CTA showed a filling defect in the main and bilateral branches of the pulmonary arteries. The left subclavian artery was occluded, with proximal extension of a strip filling defect into the aortic arch (Figure 1(a) and (b)). The patient was diagnosed with acute PE, left subclavian artery embolism, right lower limb deep vein thrombosis, atrial fibrillation, and chronic obstructive pulmonary disease.

Computed tomography angiography findings. (a) Embolism at the opening of the left subclavian artery (white arrow) and (b) main pulmonary artery embolism (white arrow).
Emergency surgery was performed under general anesthesia. First, an Aegisy filter (LifeTech Scientific, Shenzhen, China) was placed 1.0 to 1.5 cm below the opening of the renal vein. Next, a 4 F pigtail catheter was placed into the main pulmonary artery for angiography to determine the location and scope of the thromboembolism. A 6 F AngioJet mechanical thrombus removal catheter (Boston Scientific, Marlborough, MA, USA) was inserted into the main left pulmonary artery, and the thrombus was removed in thrombus suction mode. During the operation, the heart rate decreased to 40 beats/minute and the blood pressure was 200/100 mmHg. The thrombus clearance was immediately stopped. At this time, the thrombus clearance volume was approximately 50 mL. Without special treatment, the patient’s heart rate and blood pressure returned to normal and remained stable after 5 minutes of observation. Finally, the pigtail catheter was replaced for angiography (Figure 2). A balloon catheter with a diameter of 7 mm and length of 60 mm was advanced into the right femoral artery to the opening of the right external iliac artery. A balloon catheter with a diameter of 6 mm and length of 40 mm was advanced into the left femoral artery to the superior mesenteric artery, and a balloon catheter with a diameter of 7 mm and length of 60 mm was placed at the opening of the left external iliac artery (Supplementary Figure S1). The left brachial artery was incised, and a catheter sheath was inserted into it. A 4 F Fogarty double-lumen balloon catheter was used for thrombectomy, and numerous old and secondary fresh thrombi were removed. At this time, the left brachial artery spurted blood well, and pigtail catheter angiography was performed (Supplementary Figure S2).

Pulmonary artery angiography after thrombus removal. AngioJet imaging shows the main pulmonary artery after thrombus removal, with unobstructed blood flow and no significant remaining thrombus.
After 5 days, anterograde venography of the lower extremity showed a filling defect in a deep vein of the right lower extremity. Anticoagulant treatment was performed by administration of low-molecular-weight heparin calcium injection at 5000 U every 12 hours for 13 days. Oral warfarin combined with low-molecular-weight injection was administered for 5 days. After 13 days, the inferior vena cava filter was removed. The patient developed transient hemoglobinuria after the operation, which improved after symptomatic treatment. No other complications occurred. The patient’s symptoms significantly improved after the operation. His oxygen saturation was 97%, heart rate was 98 beats/minute, and troponin concentration was 0.041 ng/mL (reference range: 0.012–0.034 ng/mL). Warfarin was administered orally after the operation, and the international standardized ratio was maintained between 2.0 and 3.0. After 1 month, the patient’s treatment was changed to oral 20-mg rivaroxaban tablets daily for anticoagulation treatment to prevent deep venous thrombosis of the lower limbs and cardiac thrombosis. Computed tomography angiography 3 months after surgery showed small patchy filling defects in the arteries of the lateral segments of both lungs (Figure 3). After 9 months of follow-up, the patient had no chest tightness or wheezing, and his left radial artery pulsation was strong.
Three-month follow-up computed tomography angiography. No thrombus was present in the main pulmonary artery.
Discussion
Studies have shown that paradoxical embolism will occur when PE leads to pulmonary hypertension combined with a right-to-left shunt channel. 5 Our patient had intermediate- to high-risk PE. Preoperative echocardiography showed that the systolic pressure of the pulmonary artery was 50 mmHg, but there was no opening of the foramen ovale. However, the patient had atrial fibrillation and was not receiving regular anticoagulant treatment. Therefore, the left subclavian artery embolism was thought to have been caused by dislodgment of the left atrial thrombosis secondary to the atrial fibrillation. Studies have shown that the incidence of right atrial thrombosis in patients with atrial fibrillation is 0.4% to 2.6% and that the thrombus diameter ranges from 12 to 35 mm (average, 22 mm). Once the thrombus has become dislodged, it will cause severe PE.6,7 In our case, lower extremity venography showed deep venous thrombosis of the right lower extremity. Therefore, dislodgment of the deep venous thrombosis in the right lower limb was thought to have led to PE, rather than dislodgment of the right atrial thrombosis induced by atrial fibrillation. It is very rare for PE and systemic arterial embolism to independently and simultaneously form thrombi. We did not collect sufficient evidence to prove that this case involved independent thrombosis of these two systems.
The conventional treatment for PE is anticoagulation. Catheterization thrombolysis is reportedly safe and effective in patients with massive PE who have undergone failed systemic thrombolysis. 8 However, this method cannot quickly remove the thrombus and rapidly alleviate the symptoms of pulmonary hypertension. The elevated troponin concentration in this patient indicated that the condition was critical, and the risk stratification was intermediate- to high-risk PE. Moreover, the patient’s left subclavian artery was embolized, and the tail end of the thrombus extended to the aortic arch. Thrombolysis with urokinase or mechanical thrombolysis with the AngioJet device was associated with a risk of the thrombus dislodging, resulting in cerebral artery, visceral artery, or lower limb artery embolism.
The results of the EXTRACT-PE Trial suggested that use of an indigo aspiration system for treatment of PE was safe and effective. 9 Unfortunately, our center did not have such thrombus aspiration equipment at the time of this report. Research has shown that the AngioJet mechanical thrombus removal device can quickly remove an iliac femoral vein thrombus, compensate for the deficiency of catheter thrombolysis, and reduce the use of urokinase. 10 The AngioJet device was used in our patient to quickly remove the thrombus. The patient’s symptoms were rapidly alleviated and the use of urokinase was avoided, thus reducing the risk of thrombus shedding in the aortic arch. During mechanical thrombectomy, the patient’s heart rate decreased. This may have been caused by the high-pressure jet fluid stimulating the stretch receptor in the pulmonary artery wall, causing the vagus reflex and arrhythmia. We suggest shortening the durations of both single continuous aspiration and continuous stimulation of blood vessel walls by high-pressure jet fluid puncture. Because the tail end of the left subclavian artery thrombus extended into the aortic arch and floated with the blood flow, we chose to directly cut and remove the thrombus to avoid dislodgment. To prevent thrombosis of the superior mesenteric artery caused by thrombus shedding, a balloon catheter was used to block the superior mesenteric artery during the operation. A balloon catheter was also used to block the bilateral external iliac arteries during the operation. If the thrombus dislodged, it would enter the internal iliac artery with the blood flow, avoiding serious complications. The main goals in this case were to quickly remove the pulmonary artery thrombosis, alleviate the pulmonary hypertension, and reduce the risk of right heart failure. The thrombus of the left subclavian artery was thereafter quickly removed to prevent the thrombus from dislodging, and the blood supply of the left upper limb was restored to avoid the need for amputation.
Conclusion
In this case, AngioJet mechanical thrombectomy combined with left brachial artery incision thrombectomy was a feasible treatment option for PE combined with left subclavian artery embolism.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241258141 - Supplemental material for AngioJet thrombectomy in the treatment of pulmonary embolism complicated with left subclavian artery embolism: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605241258141 for AngioJet thrombectomy in the treatment of pulmonary embolism complicated with left subclavian artery embolism: a case report by Qiang Zhang, Yang Li, Guangfeng Zheng, Chuanyong Li, Zhichang Pan, Shuming Shi and Jianjie Rong in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241258141 - Supplemental material for AngioJet thrombectomy in the treatment of pulmonary embolism complicated with left subclavian artery embolism: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605241258141 for AngioJet thrombectomy in the treatment of pulmonary embolism complicated with left subclavian artery embolism: a case report by Qiang Zhang, Yang Li, Guangfeng Zheng, Chuanyong Li, Zhichang Pan, Shuming Shi and Jianjie Rong in Journal of International Medical Research
Footnotes
Authors’ contributions
Qiang Zhang and Yang Li carried out the studies, participated in collecting the data, and drafted the manuscript. Guangfeng Zheng, Chuanyong Li, and Zhichang Pan performed the statistical analysis and participated in its design. Shuming Shi and Jianjie Rong participated in the acquisition, analysis, or interpretation of data and drafted the manuscript. All authors read and approved the final manuscript.
Data availability statement
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Science and Technology Development Plan Project of Suzhou City (Grant Nos. SKY2021011 and SKJYD2021125), the Science and Technology Development Plan Project of Suzhou City (Grant No. SLJ2022024), and the Special Project of Diagnosis and Treatment Technology for Key Clinical Diseases in Suzhou in 2022 (Grant No. LCZX202214). The funding bodies had no role in the design of the study; the collection, analysis, or interpretation of the data; or the writing of the manuscript.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.