
Abstract
Objective
Given the extensive use of computed tomography (CT) in radiation-sensitive patients such as pregnant and pediatric patients, and considering the importance of tailoring CT protocols to patient characteristics for both the radiation dose and image quality, this study was performed to investigate the extent to which individualization of CT protocols is practiced across Norway.
Methods
This cross-sectional study involved collection of CT protocols and administration of a mini-questionnaire to obtain additional information about how CT examinations are individualized. All public hospitals performing CT to detect pulmonary embolism were invited, and 41% participated.
Results
Tailoring a standard protocol to different patient groups was more common than using dedicated protocols. Most of the available radiation dose-reduction approaches were used. However, implementation of these strategies was not systematic. Children and pregnant patients were examined without using dedicated CT protocols or by using protocol adjustments focusing on radiation dose reduction in 30% and 39% of the hospitals, respectively.
Conclusion
Practice optimization is needed, especially the development of dedicated CT protocols or guidelines that tailor the existing protocol to pediatric and pregnant patients. Practice might benefit from a more systematic approach to individualization of CT examinations, such as inserting tailoring instructions into CT protocols.
Keywords
Introduction
The substantial increase in computed tomography (CT) use1–4 despite concerns about a potential increase in the risk of radiation-induced cancer4,5 is evidence of the value of CT in medical care. An increase in CT use has also been documented in Norway. 6 Radiation doses for CT examinations vary considerably among patients, institutions, and countries,4,7 and the variation is mostly attributable to the way in which CT scanners are used (i.e., the technical parameters of the CT scanning protocols). 8 The greatest variation (15-fold) is observed in CT examinations for suspected pulmonary embolism (PE). 8
CT pulmonary angiography (CTPA) is the first-choice method for diagnosing PE because of its accuracy, speed of diagnosis, and accessibility. The threshold for referral for CT because of suspected PE is low 9 because of the high mortality (30% reported mortality when untreated, 10 and PE is the third most frequent cause of death among cardiovascular diseases after myocardial infarction and stroke11–13) and nonspecific symptoms (such as chest pain and shortness of breath, which are common in many pulmonary and cardiac conditions). The main challenge associated with the use of CT for suspected PE is its frequent use in young female patients because of the higher risk of PE associated with oral contraceptives, pregnancy, and the postpartum state. 13 The rate of CT use in pregnant patients has markedly increased during the last decade, and most of these examinations were performed for suspected PE. 14
The incidence of PE in children appears to be quite low, but it is often underestimated. 15 However, the use of hormonal contraceptives among adolescents is increasing, especially among younger adolescents (12 to 15 years old), 16 and contraceptives are prescribed to patients as young as 10 years old 17 for various medical reasons such as excessive or irregular menstruation or treatment of acne.16,17 This increases the risk of PE in pediatric patients and the use of CTPA in this patient group. Despite the quite low incidence of PE, this patient group needs special attention because radiation-induced cancer in girls is estimated to result from every 330 to 480 chest CT examinations. 18
The use of CTPA in radiation-sensitive patients such as pregnant patients and female adolescents makes tailoring the CT protocol to the patient crucial to achieve the highest cost–benefit ratio in terms of the radiation dose and amount of contrast agent needed to obtain the required image quality. This goal can be achieved by patient-centered imaging,19,20 which involves the use of patient-tailored CT scan protocols. Tailoring the imaging protocol to the patient is crucial for providing accurate information to the physician. 21 Additionally, one of the most strongly emphasized advantages of protocol tailoring is the consistency of image quality across various patient sizes. 22
CT protocols should be tailored based on patient age, size, and clinical condition,23,24 and dedicated pediatric protocols are often needed. 25 Both the International Atomic Energy Association 26 and the International Commission on Radiological Protection 27 strongly recommend that only pediatric protocols should be used in children. Increased use of CT in pediatric patients together with a variation in radiation doses 18 reinforces the need for optimization. Individualization of pediatric CT protocols can result in radiation dose reductions ranging from approximately 50% to 90% without compromising diagnostic image quality. 28 Along with pediatric patients, another group who might benefit from radiation dose reduction are pregnant patients because of the rapid cell multiplication in both the fetus and mother. 29
Various approaches have been used to reduce radiation doses,19,23,29–33 such as reducing the scan length, lowering the kilovoltage peak settings, using automatic tube current modulation (ATCM), and using iterative reconstruction. ATCM is a widespread dose-reduction measure30–33 that allows the use of different tube currents (mA) along the z-axis depending on patient size and different attenuations depending on body regions. Organ dose modulation is a more advanced technique that reduces the tube current over the anterior aspect of the body and reduces the irradiation of the breast tissue. This technique was shown to be more efficient than ATCM in reducing the total radiation dose. 34 A simple and highly effective dose-reduction approach is scan range reduction. A mean scan range reduction of 30% to 33% in the CTPA protocol can result in a 23% to 27% effective dose reduction.23,29 This benefits pregnant patients by allowing an 83% estimated radiation dose reduction to the fetus (explained by the increased distance between the fetus and the scanned volume). 29 Another effective dose-reduction measure that is especially suitable for CTPA is the use of a lower tube potential.19,23,30–33 Previous studies have shown the feasibility of reducing the tube potential to 80 kVp.35–38 Reducing the tube potential also provides the possibility of lowering the amount of iodinated contrast agent.31,38 Automatic kilovoltage peak selection in relation to patient size is an available function on newer CT scanners and has been shown to reduce the radiation dose.31,32,39 In one study, the use of this function in CTPA resulted in a selected tube potential of 70 to 90 kVp (80 kVp in most cases). 29 The use of dual energy in CTPA reportedly provides similar image quality at lower radiation doses. 40
Considerable differences among CT scanners (geometry, filtration, detector efficiency, and reconstruction algorithms) result in considerable differences in image quality obtained at given exposure parameters on different CT scanners. 42 Both the possibility for use of iterative reconstruction and the adapted dose shield stand out among the scanner-related features because of their notable radiation dose-saving potential.31,32 Radiology departments quite commonly have two or more CT scanners of different models, and the choice of the CT scanner used for a clinical indication and/or a particular patient group might also be employed as a dose-reduction strategy.
Regularly reviewing CT protocols is essential to ensure that all protocols are correctly configured so that the image quality and dose are being optimized.25–27,42–46 Protocol reviewing and optimizing requires a team-based approach, and the team should comprise a radiologist, physicist, and radiographer.44–46
Given the extensive use of CT in radiation-sensitive patient groups such as pregnant and pediatric patients, and considering the importance of tailoring CT protocols to patient characteristics in terms of both radiation dose and image quality, this study was performed to determine to what extent individualization of currently used CTPA protocols is practiced. The investigation focused on how CT protocols are tailored when examining radiation-sensitive patients such as pediatric and pregnant patients and what radiation-saving approaches are used to tailor the protocols to those patients across hospitals in Norway. Our hope is that a review of current practices will be valuable for identifying any optimizing potential.
Methods
This cross-sectional study involved collection of the CT protocols used to investigate PE from Norwegian hospitals along with administration of a mini-questionnaire to obtain additional information about the departments’ practices regarding individualization of CT examinations. All public hospitals that perform CTPA examinations were invited to participate (n = 41). An email was sent to each hospital’s senior CT radiographer and included free text response questions focusing on routines for tailoring the CT examination to different patient groups and routines for CT protocol optimization along with a request to send us all the protocols they use for PE. Because of the limited number of replies after the first mailing round, a second mailing round was conducted 3 weeks later.
Triple rule-out (a protocol used for simultaneous examination of the coronary arteries, thoracic aorta, and pulmonary arteries) and other combined protocols used to assess other conditions in addition to PE were excluded from the study.
Among the collected material, we analyzed the number of protocols the hospital uses to detect PE, to which patient groups these protocols are dedicated, differences between the standard protocols and the protocols used for pediatric or pregnant patients in the same hospital, and the presence or absence of radiation dose-reducing approaches (e.g., the use of automatic kilovoltage peak, dual energy, iterative reconstruction, and other approaches). The data were first registered in an Excel file (Microsoft Corp., Redmond, WA, USA) and then exported to SPSS version 24 (IBM Corp., Armonk, NY, USA). The collected data were analyzed using descriptive statistics.
Ethical considerations
The participants were informed about the aim of the study and received the research protocol, which had been approved by the university. They were also informed that participation in this study was voluntary and that an email reply containing attached CT protocols would be regarded as implied consent to participate. Moreover, the participants were informed that the name of the person replying to the email would not be registered at all and that the name of the hospital would not be disclosed. The need for approval from the Regional Committee for Medical and Health Research Ethics and the Norwegian Centre for Research Data was waived because the project did not involve any health-related or personal information.
Results
Response rate
The overall response rate after the two emails were sent was 41% (17 of 41 hospitals). The participating hospitals represented 13 of the 20 health trusts in Norway from all four regional health authorities in the country. The total number of protocols used solely for PE was 41, and seven combined protocols were excluded. All participants answered the mini-questionnaire completely.
Protocol individualization practices
The data showed variation in the number of protocol variants used for PE. The most common situation was having solely a standard protocol (41%), followed by two protocols (29%). Other hospitals had four, six, or even eight protocols (6% each).
Almost all hospitals (with only one exception) reported tailoring their protocols using various criteria (Figure 1). The respondent who reported using the standard protocol without any adjustments stated that the use of ATCM was sufficient for tailoring the examination to different patient characteristics. The routines for tailoring protocols differed among the hospitals, and most of them used more than just one method (Figure 2).

Protocol-tailoring practices at different hospitals. The results are expressed as percentages, and most participants reported more than one alternative.

Protocol-tailoring methods at different hospitals. The results are expressed as percentages, and most participants reported more than one alternative.
ATCM was used in all CTPA protocols; 35% also used automatic kilovoltage peak selection, while 29% used dual energy. All hospitals that did not use automatic kilovoltage peak selection used a tube potential of ≤100 kVp except for one hospital that used a tube potential of 120 kVp in their standard CTPA protocol. Iterative reconstruction was used in 41% of the hospitals.
Protocol individualization practices for pediatric patients
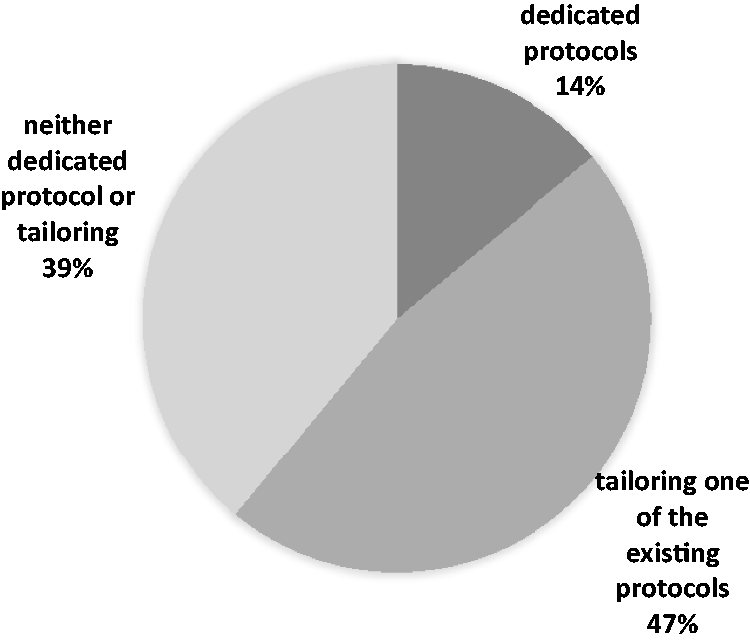
In total, 24% of the hospitals reported that they never examined pediatric patients suspected to have PE and that these patients were transferred to larger hospitals with dedicated pediatric departments. The data showed that it was more common to tailor one of the existing CT protocols to children than to have a dedicated pediatric CTPA protocol, while some of the radiology departments had neither pediatric CTPA protocols nor routines for tailoring the existing protocols to children (Figure 3). Some of the participants who did not report the existence of pediatric protocols or tailoring routines for children stated that they tailored the CT examination based on the patient’s age. The radiation dose-reducing approaches used by the participants to tailor the protocol to pediatric patients were using lower kilovoltage peak settings and automatic kilovoltage peak selection as well as using the newest CT scanner.

Protocol-individualization practices regarding pediatric patients. The statistic does not include the participants who reported that they never examine pediatric patients suspected to have pulmonary embolism.
Protocol individualization practices for pregnant patients
In total, 12% of the hospitals reported that they never examine pregnant patients suspected to have PE. Similar to the situation regarding pediatric patients, it was more common to tailor one of the existing protocols than to have protocols dedicated to pregnant patients (Figure 4). Radiation-saving approaches used to tailor the protocol to pregnant patients were reducing the scan length, lowering the kilovoltage peak settings, and using the newest CT scanner. Additional practices were tailoring the amount of contrast agent and tailoring the injection flow rate.
Protocol-individualization practices regarding pregnant patients. The statistic does not include the participants who reported that they never examine pregnant patients suspected to have pulmonary embolism.
Practices for protocol reviewing and optimizing
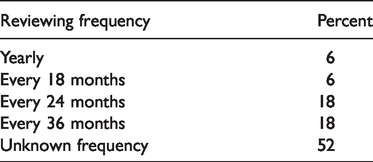
Most hospitals had no established procedures for CT protocol updating. Half of the senior CT radiographers reported that the date of the last protocol update was unknown, and the remaining radiographers reported that they reviewed the protocols periodically (every 18, 24, or 36 months). In contrast, almost all the departments updated the protocols when needed; in some cases, this was performed in addition to the periodic protocol review (Table 1). The hospitals that updated their protocols yearly reported using an electronic system to remind them when the time for the periodic protocol review is approaching.
Protocol-reviewing frequency.
The lead radiologist and the lead CT radiographer shared the responsibility for protocol reviewing and optimizing, and only 30% reported participation of a physicist in the process.
The mini-questionnaire included a question asking which resources are used to optimize the CT protocols. The results showed that the participants used multiple resources to optimize their protocols. The most common were protocols used by colleagues from other hospitals (88%), scientific publications (peer-reviewed journals and textbooks) (88%), courses (82%), and manufacturers’ recommendations (82%) followed by local protocol testing (53%). Many respondents specified that protocols recommended by the manufacturer were used as a starting point and that those protocols were later optimized by performing small changes based on small-scale testing.
Discussion
The present study showed that the most common situation among Norwegian hospitals was using a single standard protocol and tailoring this standard protocol based on different patient characteristics. Using the standard protocol in all patients without any adjustments was an exception. Relying solely on ATCM even when having optimized protocols (as in one of the cases in this study) still does not ensure that the examination is tailored to different patient groups, especially pediatric patients. As emphasized by the International Commission on Radiological Protection, 42 the use of ATCM does not totally free the operator from selection of scan parameters. The various approaches to reduce radiation doses mentioned in the literature19,23,29–33 were used to different extents in the participating hospitals. The use of a lower tube potential was the most commonly used approach, with almost all hospitals using a tube potential of 100 kVp or even lower, probably because of the high number of studies confirming the effectiveness of this method in dose reduction without compromising image quality.23,35–38 The choice of the CT scanner was actively used as a radiation dose-reduction strategy by scanning radiation-sensitive patients such as pregnant and pediatric patients with the newest CT scanner, which usually has radiation dose-reducing features such as iterative reconstruction, dual energy, and automatic kVp selection.
Although the results of this study show knowledge of most of the available radiation dose-reduction approaches, implementation of these strategies was not systematic. Protocol tailoring based on ad-hoc assessment performed by the radiographer alone or in collaboration with the radiologist was still very common (Figure 2), even when more systematic approaches (such as the inclusion of tailoring instructions in the protocol) might be more efficient in providing consistency with best practice standards. 46 A concerning finding of this study is that children might be examined using adult CT protocols without any adjustment in 30% of the hospitals, which is totally against the existing recommendations.26,27,42 Additionally, 39% of the pregnant patients were examined without using dedicated protocols or specific adjustments focusing on radiation dose reduction in this particular radiation-sensitive patient group. Using protocol tailoring based only on body weight categories might be detrimental to pregnant patients because they will be scanned with a higher radiation dose protocol because of gestational weight gain. Increasing the radiation dose by placing the pregnant patient in a higher weight category is totally unnecessary because only a low percentage of gestational weight gain is caused by breast enlargement or fat deposition in the upper body. 47 Use of the pregestational weight as a criterion for choosing the protocol might be a better alternative. 35
The lack of systematic routines for protocol reviewing and optimizing in half of the hospitals indicates a need for practice improvement because regular reviewing is essential to ensure a correct balance between the radiation dose and image quality.25–27,42–46 Even in hospitals with systematic protocol-reviewing routines in the present study, the reviewing frequency was lower than the recommended yearly frequency.44,46 Another necessary improvement in some hospitals is the inclusion of a physicist in the protocol review and optimization team as recommended by most sources.26,42,44
Most of the participants reported use of scientific publications as a source of knowledge when optimizing their protocols. However, academic publications offer little general information on practical approaches for reviewing and optimizing protocols 46 and no guidance on how to best apply the results to a particular CT scanner. 45 Protocols cannot simply be transferred between different scanner models. 42 The results of the current study confirm that staying up to date with the literature is beneficial but is not sufficient; this is because half of participants who declared using scientific literature had no established procedures for protocol updating and optimizing, and some of them tailored the examinations to only a small extent. Previous studies have shown that clinical practice improves when all radiographers are involved in auditing and optimizing processes.29,48 Feedback on doses used in CT examinations performed at the department might also be an effective measure because it was proven to cause significant dose reduction especially in combination with education on dose-reduction strategies. 48 Practicing patient-centered imaging will require substantial changes in the current imaging culture, with key components being greater emphasis on implementing radiation dose-optimization strategies 20 and support from the administration, especially allocation of sufficient amounts of dedicated time and resources.44,46
To the best of our knowledge, this is the first study to analyze practices regarding CT protocol individualization. The study included 41% of public hospitals representing all four regional health authorities in Norway, and it is therefore reasonable to consider the results as representative of the country.
The study has several limitations. First, the percentage of hospitals that perform CT examination of children with neither pediatric CTPA protocols nor routines for tailoring the existing protocols to children might have been overestimated because we cannot be sure that this was the case for all departments in which children were not examined (the mini-questionnaire did not include a specific question about what patient groups they examine). This might also apply to pregnant patients. Second, only the senior CT radiographer of the department answered the questions, and he or she might not have had extensive knowledge of all the ad-hoc protocol adjustments made by the other radiographers. As noted in a previous study, clinical practice is largely subjective and ad-hoc. 49 The extent to which the scanning parameters of the CT protocol are adjusted when examining children or pregnant patients might therefore be higher than reported in the current study.
Conclusion
This study provides an overview of how CTPA examinations are tailored to different patient characteristics at Norwegian hospitals. The results reveal the need for practice optimization, especially with regard to developing dedicated CT protocols for pediatric and pregnant patients or inserting tailoring instructions into the existing standard CT protocols. Practice might benefit from a more systematic approach to reviewing and optimizing the CT protocols (based on quantitative evaluation of the patient dose and image quality) and from formalizing the role of the protocol-optimizing team, which should always include a physicist. We anticipate that the present assessment of current practices reported by the participating hospitals will prove the interim value of future research on implementing patient-centered imaging.