
Abstract
Objective
To assess Lebanese medical students’ attitudes towards patient safety and medical error disclosure.
Methods
This was a cross-sectional study involving medical students from seven different medical schools in Lebanon. The participants completed the Attitudes to Patient Safety Questionnaire (APSQ-III) online, which consists of 26 items across nine key patient safety domains. Items were scored from 1 (strongly disagree) to 5 (strongly agree). Demographic data were also collected.
Results
Of the 549 students enrolled in the study, 325 (59%) were female and 224 (41%) were male. More than half (287, 52%) were aged between 20 and 22 years and 95% were Lebanese. The overall attitude of students towards patient safety was positive (3.59 ± 0.85) with the most positive attitudes in the domains of ‘Team functioning’ followed by ‘Working hours as an error cause’. More positive attitudes were perceived among male students in the domains of ‘Professional incompetence as an error cause’ and ‘Disclosure responsibility’ whereas more positive attitudes were seen in female students in the domain of ‘Working hour as an error cause’. Older medical students had more positive attitudes in the domain of ‘Team functioning’ than younger students.
Conclusion
Medical students in Lebanon had an overall positive attitude towards patient safety. These findings may be used to guide improvements in patient safety education and enhance patient-centred care in medical institutions in Lebanon.
Introduction
Providing patients with a safe and comfortable medical environment is a key challenge for medical institutions and healthcare organizations worldwide. 1 The culture of safety in the medical field is directly related to the ethical and moral conduct of clinicians, as evidenced by the reduction in morbidity and mortality of patients when patient safety measures are implemented. 2 Therefore, it can be inferred that fostering a culture of safety is a fundamental principle essential for attaining the best levels of patient care. 2 Patient safety is the prevention of medical mistakes and patient harm-related malpractice caused by any health care worker, 3 and can be implemented by a set of interrelated activities that focus on reduction of avertable harm and medical mistakes. 4
Data show that, in Europe, approximately one in every 10 patients is harmed during hospital care. 5 Importantly, unexpected adverse events can occur in any setting where healthcare is provided. 3 According to the Institute of Medicine (IOM), medical malpractice is one of the leading causes of death and injury; it has been estimated that preventable adverse events cause an estimated 44,000 to 98,000 hospital deaths in the USA each year. 6 The most common mistakes that occur during medical care are drug related (e.g., incorrect dosage or route of administration, or, use of a drug that may trigger an allergic reaction).7,8 The IOM has created several recommendations on a legislative level to help prevent such errors, and they specifically include the practise of consistently evaluating health care providers for proper clinical practice, and, ensuring that they have knowledge about patients’ safety. 6 All of these practices emphasise the importance of education and training for patient safety starting early in medical school. 4 The importance and integration of patient safety into medical education has been recognized by The World Health Organization (WHO) which has published a Patient Safety Curriculum Guide for medical students. 9 Including patient safety training into all medical school curricula will undoubtedly improve medical care globally and prevent avoidable mistakes. 10
With regard to Lebanon, more than 1,000 medical malpractice-related complaints were filed between 1996 and 2013, to the Lebanese Order of Physicians. 11 However, in Lebanon there is a culture of not reporting medical incidents because of fear of negative impact and consequences. It has been estimated that 60% of clinicians in Lebanon do not disclose medical mistakes or near misses. 11 A survey showed that 82% of providers were afraid that any events that occurred, even if connected to system faults, would be retained in personal files rather than being used for performance improvement. 11 In 2020, a cross sectional study involving 176 physicians and nurses working in medical centres in Lebanon was conducted by American University of Beirut. 12 Only 60% nurses and 48% physicians agreed that all medical errors should be revealed or reported, with most nurses (95%) and physicians (90%) citing the error's consequence as a critical factor that had to be considered before disclosure. 12
Worldwide, studies have been performed to assess the attitudes of medical students to patient safety and they have achieved varying results.1,4,13,14 To our knowledge, no similar studies have been undertaken in Lebanon. Therefore, we conducted a cross-sectional study across seven different medical schools in Lebanon to assess students’ attitudes towards patient safety and medical error disclosure.
Methods
Study population
For this cross-sectional study, undergraduate medical students were enrolled from seven medical schools in Lebanon; Beirut Arab University (BAU); Lebanese University (LU); University Saint Joseph (USJ); University of Balamand (UOB); Lebanese American University (LAU); American University of Beirut (AUB); Holy Spirit University of Kaslik (USEK). Data were collected from November of 2021 to March 2022. With the exception of LU, USJ and USEK, which use French language, the remaining four medical schools use English as the official teaching language. The duration of teaching programs varies per medical school and ranges from four to seven years. The study was open to any undergraduate medical student in Lebanon who was enrolled in a medical program. No exclusion criteria were set.
A pilot study involving 20 students enrolled across the different universities and in different clinical years was conducted to ensure the quality and feasibility of the survey. Following this initial process, the online questionnaire was finalised. The students involved in the pilot study did not participate in the final study.
Questionnaire
For the final study, the 26-item Attitudes to Patient Safety Questionnaire (APSQ-III) was used. 10 English language was used for the questionnaire and it was self-administered and sent via email. Demographic data (i.e., sex, age, nationality, university and medical year) were also collected. An attached cover letter which explained the purpose of the study was included with the questionnaire. The APSQ-III consists of 26 items across nine key patient safety domains. The nine domains were as follows: Patient Safety Training Received; Error Reporting Confidence; Working Hours as an Error Cause; Error Inevitability; Professional Incompetence as an Error Cause; Disclosure Responsibility; Team Functioning; Patient Involvement to Reduce Error; Importance of Patient Safety Training. 10 The internal consistency of the nine domains has been reported to range from 0.64 to 0.82. 10 Participants were given four weeks to complete the questionnaire and sent a reminder email after two weeks. Items were scored using a Likert-type scale which ranged from 1 (strongly disagree) to 5 (strongly agree).
The study was approved by the Institutional Review Board of Beirut Arab University (2022-H-0111-M-R-0483). All participants were fully informed about the study's goal, and all data were collected and retained anonymously. Participants were assured that their involvement was completely voluntary, and that their decision to participate had no influence on their academic standing. The reporting of this study conforms to STROBE guidelines. 15
Statistical analysis
Using Qualtrics.com calculator with an estimated 3000 medical students in Lebanon, a confidence level of 95% and a margin error of 5%, the sample size was estimated to be 350 participants. 16 Statistical analysis was performed using SPSS software (version 26.0 for Windows®; IBM Corp, Armonk, NY, USA). A P-value <0.5 was considered to indicate statistical significance. Demographic data were described as frequencies and percentages. For each individual item and the nine key domains, the results were displayed as mean (±standard deviation).
The Overall APSQ-III Score describes overall patient safety attitudes with a maximum score of 5. This was calculated by dividing each total APSQ-Score by the total number of items and then representing this score as one mean (±SD) for all participants. 17 The reliability of the different domains was also measured using Cronbach’s alpha coefficient. Subgroup analysis was conducted using one-way ANOVA and Student’s t-test to assess associations between participants’ demographics (i.e., sex and age) and their APSQ-Score.
Results
In total, 549 medical students completed and returned the electronic questionnaire (Table 1). Of the 549 students, 325 (59%) were female and 224 (41%) were male. More than half of the students (287, 52%) were aged between 20 and 22 years. Most were Lebanese (95%) and attended Beirut Arab University (65%). The next most common medical school was Lebanese University (18%). None of the other medical schools were attended by more than 5% of the students. Approximately, two-thirds of students (329, 60%) were in years 1–3 of medical studies.
Socio-demographic characteristics of the participants.

*Includes Syria, Palestine, Iraq, Saudi Arabia, and Sudan.
Data are expressed as, n (%) or mean ± SD.
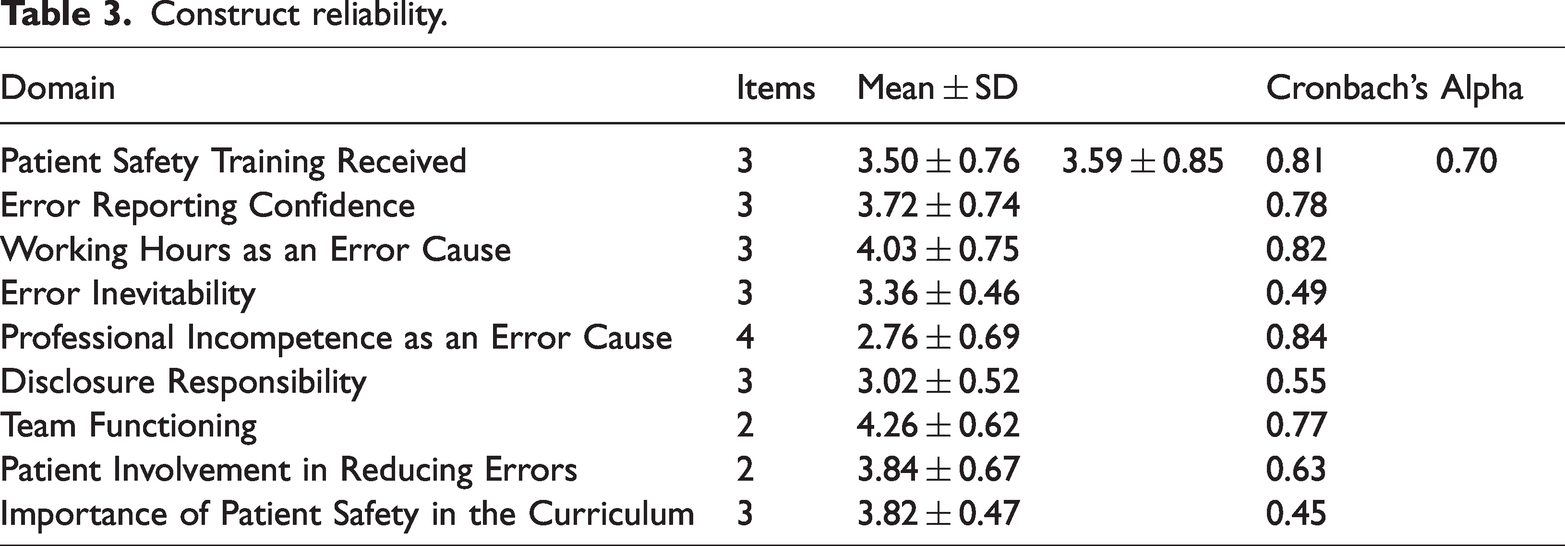
The ‘Team functioning’ score was the highest score among all nine domains (4.26 ± 0.62) followed by ‘Working hours as an error cause’ (4.03 ± 0.75) (Table 2). The ‘Professional incompetence as an error cause’ domain had the lowest score of all nine domains (2.76 ± 0.69). Of all 26 questions posed, the item ‘Teaching student about patient safety should be an important priority in medical students training’ had the highest score (4.44 ± 0.63) whereas the item ‘A true professional does not make mistakes or errors’ had the lowest score (1.87 ± 0.91). Overall, the data showed that across the Lebanese medical schools, the overview of patient safety culture among the students was positive. The mean overall APSQ score was 3.59 ± 0.85 out of a maximum of 5.0 (Table 3). The reliability coefficients of the domains ranged from 0.45 to 0.84 (mean 0.70) which indicated acceptable internal consistency (Table 3).
Attitudes of medical students towards patient safety (N = 549)

Data are expressed as mean ± SD.
APSQ, Attitudes to Patient Safety Questionnaire.
Construct reliability.
Investigating associations between sex and attitudes, statistically significantly more positive responses were observed among male students compared with female students in the domains of “Professional incompetence as an error cause” (P = 0.022) and “Disclosure responsibility” (P = 0.001) whereas statistically significantly more positive attitudes were observed among female students compared with male students in the domain of “Working hours as an error cause” (P = 0.039). (Table 4).
Correlation between Sex and APSQ scores.

Data are expressed as mean ± SD.
APSQ, Attitudes to Patient Safety Questionnaire; ns, not statistically significant.
Investigating associations between age and attitudes, showed that younger students (i.e., <20 years) had a statistically significant higher mean score than older students in the domain of “Importance of patient safety in the curriculum” (P = 0.022), whereas students >22 years had statistically significant higher mean scores than younger students in the domain of “Team functioning” (P = 0.002). (Table 5).
Correlation between Age and APSQ scores.

Data are expressed as mean ± SD.
APSQ, Attitudes to Patient Safety Questionnaire; ns, not statistically significant.
Discussion
Patient safety education and training for undergraduate medical students should be a priority for all universities. 1 The more we expose our future physicians to safety practices and training programs, the more they become capable of avoiding medical errors. Therefore, screening medical students’ cognizance of key areas of patient safety, provides a chance to improve their clinical acumen and future practices. 1
The findings of this study involving 549 medical students in Lebanon, showed an overall high APSQ III score and so indicated that patient safety culture among the students was positive. In this respect, our results were consistent with those observed in cross-sectional studies conducted in China, Pakistan and Palestine, where the medical students’ attitudes to patient safety were also positive.1,13,17 We found that ‘Team functioning’ had the highest score among all domains. Similar results have been found in studies conducted in Pakistan and Saudi Arabia.13,18 Accordingly, medical students do recognize the importance of teamwork in preventing mistakes, and, it appears that team functioning is an important subject in medical school curricula in other countries. Interestingly, we found that the more senior students in our study (i.e., >22 years) had a significant understanding of the importance of team work. These findings were similar to those seen in a study from Tunisia. 19 We suggest that the better understanding of team work in more senior students is likely to reflect the increased exposure they have had to clinical rotations, where students have had the chance to witness collaboration among different members of hospital teams to ensure best patient care.
We also observed high APSQ III scores for ‘Working hours as a cause of error’; these results were similar to those from a study conducted in Malaysia where students were convinced that long shifts were associated with an increase in medical errors. 20 These data suggest that medical students do recognize the importance of short shifts and proper rest during shifts. Results from a systematic review and meta-analysis of 10,072 studies concluded that an increased risk of medical errors was associated with working >20–24 hours/day. 21 Recently, in Lebanon, as the economic crisis deepens and physician shortages increase, medical staff have had to increase their workload and work for extended hours. In addition to increased psychological distress, Lebanese physicians have been reported to experience significant burnout. 22 Importantly, studies suggest that doctors who are burned out have 44–48% greater odds of self-reported medical errors. 23
We found that the lowest mean score out of all nine domains was for ‘Professional incompetence as an error cause’. These findings are consistent with those from other studies conducted in China, Pakistan and Tunisia.1,13,19 Therefore, we suggest that medical students regard errors as individual failures, which reinforces the importance of ensuring they are aware that even the most competent doctors may commit unintentional mistakes.
Similar to data from Pakistan, we observed that the second lowest scoring item was ‘Disclosure responsibility’. 10 These results suggest that medical students do not believe that reporting medical errors is necessary, probably because they may fear punitive action. Although undeclared, a culture of blame among medical professionals is undoubtedly present. Although stressing the importance of disclosure of medical errors in the curriculum is crucial, the most significant element in improving error disclosure is ending the practice of penalising the informant. Moreover, it should be emphasized to the students that recognising faults in the system will certainly prevent further errors in the future.
Interestingly, our male students had significantly more positive attitudes towards the domains, “Professional incompetence as an error cause” and “Disclosure responsibility” compared with our female students. These results are consistent with studies from Palestine and Tunisia, which also found positive attitudes of male students for the domain of disclosure responsibility.17,19 These results suggest that perhaps female students may fear punishment more than male students. More research is required outside the Arab world to determine if this finding is demonstrated in other countries.
Within the domain of ‘Importance of patient safety in the curriculum’ the question ‘Teaching student about patient safety should be an important priority in medical students training’ received the highest mean score compared to all other questions. These results are concordant with those from a study conducted in Germany, 24 and emphasize that patient safety cannot be taught by diffusion in the workplace, but must be a mandatory requirement for all medical school curricula. While errors are inevitable, medical schools should instil the concept of patient safety and prevention of medical errors by comprehensive integration of patient safety teachings within the students’ education. 25
The study had some limitations. For example, we used a questionnaire-based design which rendered the study subject to recall bias. In addition, we noted that the response rates of the students varied among the universities, which may have reflected differences in the teaching of knowledge and attitudes towards patient safety among the universities. However, we believe that this study provides good baseline data that can assist curricular reforms. Importantly, it is the first study concerning this topic conducted in Lebanon. Moreover, the participants belong to various medical schools in Lebanon, which reflects the diversity of the participants. Furthermore, we used a validated questionnaire developed specifically for medical students.
In summary, our research explored the attitudes of medical students in Lebanon towards patient safety culture. Lebanese students had an overall positive attitude towards patient safety while misperceiving some domains, particularly those related to error causality and importance of disclosure of errors. Students should be encouraged to view errors as learning opportunities and should be taught about the importance of disclosing errors to learn from mistakes and prevent future errors from occurring. Our results can be used to guide improvements in medical curricula, but reform will not change current attitudes unless hospitals take the initiative and deal with medical errors as cornerstones for improvement without undue blame or punitive action for medical personnel.
Footnotes
Acknowledgements
The authors of this study would to thank all study participants for their valuable role in this study.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.