
Abstract
Pylephlebitis, which is a type of septic thrombophlebitis of the portal vein, is a rare and life-threatening complication that commonly occurs following appendicitis. However, nonspecific abdominal complaints and fever can impede the diagnosis of pylephlebitis. Timely use of appropriate antibiotics and anticoagulants is paramount for treating this condition. We present a case of pylephlebitis and septic shock caused by acute nonperforated appendicitis. A 32-year-old man presented with migratory right lower abdominal pain. Blood cultures showed the presence of Escherichia coli. Blood test results showed increased bilirubin concentrations and coagulation factor abnormalities. A computed tomographic abdominal scan showed that the portal vein had a widened intrinsic diameter. After intensive care treatment with antibiotics, antishock therapy, anticoagulants, and other supportive treatments, the infection was monitored, the abdominal pain disappeared, and the jaundice subsided. Laparoscopic appendectomy was performed. Histopathology showed acute suppurative appendicitis, and no abnormalities were observed during the follow-up period after discharge. A multidisciplinary approach is mandatory for the decision-making process in the presence of pylephlebitis caused by appendicitis to obtain a correct diagnosis and prompt treatment. Similarly, the timing of appendectomy is important for minimizing intra- and postoperative complications.
Introduction
Pylephlebitis is septic thrombophlebitis of the portal vein system. Pylephlebitis is an uncommon but life-threatening complication of an intra-abdominal infection. This condition usually occurs following diverticulitis or appendicitis. Acute appendicitis is one of the most common surgical emergencies. 1 The most common pathogens are Bacteroides species and gram-negative bacilli, such as Escherichia coli, Klebsiella, and Enterobacter. 2 In cases of perforated or purulent appendicitis, spillage of infected and faecal matter into the peritoneal cavity may result in septic shock, and bacteria entering the portal vein circulation lead to pylephlebitis. Nonspecific symptoms and clinical findings of pylephlebitis often make its diagnosis difficult. We describe the case of a man who presented with pylephlebitis secondary to nonperforated appendicitis. He was successfully treated with appendectomy following antibiotics and anticoagulants. This case report was prepared in accordance with the SCARE criteria. 3 The reporting of this study conforms to the CARE guidelines. 4
Case description
A previously healthy 32-year-old man without any surgical history presented to the Emergency Department with a 2-day history of high fever/chills, severe abdominal pain, and nausea/vomiting. Additionally, his symptoms were accompanied by dizziness, oliguria, and dark urine. His highest body temperature was 40°C, and after taking medication, his body temperature gradually returned to normal. However, the abdominal pain did not resolve. He denied having any diarrhoea, constipation, haematemesis, or melena. He denied having any prior similar symptoms and had no prior abdominal imaging, such as ultrasound or computed tomographic (CT) scans. The patient also denied any family history or surgical history.
On admission to the Emergency Department, the patient had a high temperature (39.5°C), low blood pressure (90/65 mmHg), a high heart rate (115 beats/minute), and high respiratory rate (22 breaths/minute). A physical examination showed that his abdomen was slightly tense but diffusely tender with point tenderness and rebound pain at McBurney’s point in his lower right abdomen.
The patient’s blood test results were abnormal, with increased white blood cells (31.49 × 109/L) and neutrophils (96.3%), a prolonged prothrombin time-international normalized ratio (1.71 s), increased D-dimer concentration (6734 ng/mL), and increased bilirubin concentration (62.8 µmol/L). Albumin, calcium, and potassium concentrations were decreased. His vital signs and laboratory data are shown in Table 1.
Laboratory parameters on admission and postoperation.

WBCs, white blood cells; PT-INR, prothrombin time-international normalized ratio; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
An abdominal CT scan showed that the portal vein had a widened intrinsic diameter (Figure 1a) and an abnormally dilated appendix (15 mm) with an increased density of surrounding fat spaces, but no perforation or abscess (Figure 1b). To clarify the cause of the elevated bilirubin concentration, an abdominal ultrasound was performed and showed mild dilation of the portal vein without a clear cause of biliary obstruction, such as gallstones or tumours (Figure 1c). A blood culture was positive for Escherichia coli. A histopathological examination of the resected specimen (60 × 15 mm) confirmed acute suppurative appendicitis. After we took into account the patient’s medical history, the final diagnosis was acute appendicitis, pylephlebitis, and septic shock.
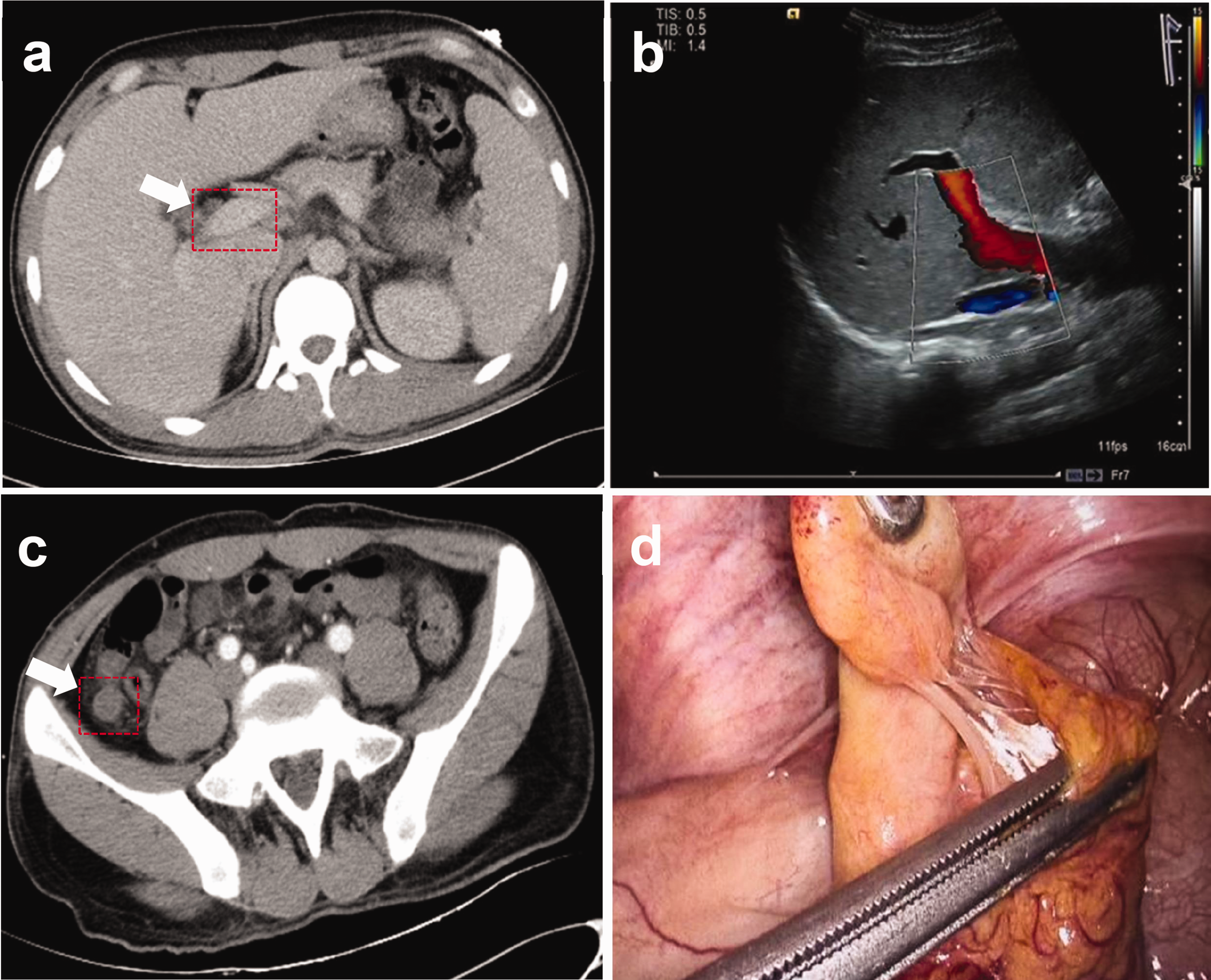
Imaging and macroscopic examinations. (a) Computed tomographic image of the portal vein with a widened intrinsic diameter (13 mm). (b) Ultrasound measurement of the portal vein, which was dilated to 13 mm in diameter. (c) Computed tomographic scan shows an abnormally dilated appendix (15 mm) and (d) an enlarged appendix was visible during surgery, but there was no perforation or abscess.
He was treated with broad-spectrum intravenous antibiotics (piperacillin/tazobactam, chosen empirically) after a blood culture was performed and was quickly admitted to the intensive care unit. At the same time, he was treated with anti-shock therapy, anticoagulation therapy (with enoxaparin for 7 days), and other supportive treatments. A blood culture was positive for E. coli, and piperacillin/tazobactam was administered continuously for targeted therapy. Fourteen days after admission, his condition remained stable, and all indicators of the blood test showed considerable improvement. The blood culture showed no bacterial growth, the D-dimer concentration had decreased to normal, the bilirubin concentration was within the normal range, and a CT scan showed no signs of portal vein dilation or other abnormalities. However, the appendix was still enlarged. A physical examination showed no palpable abdominal pain except at McBurney’s point in the lower right abdomen. After consultation with a multidisciplinary team, all of the experts believed that the patient’s portal vein inflammation had been effectively controlled and that there was no systemic inflammatory response. However, primary acute appendicitis persisted. Therefore, the patient underwent laparoscopic appendectomy and was followed up owing to the possible occurrence of portal vein inflammation after the operation (Figure 1d).
The patient was discharged on the 20th day without complications. He appeared healthy and had no clinical or laboratory abnormalities at a 3-month follow-up visit.
Discussion
Pylephlebitis begins with a suppurative thrombus of the portal vein and/or its branches and is secondary to diverticulitis and appendicitis, which are the most common intra-abdominal infections. 5 The mortality rate of septic pylephlebitis is high, but the total mortality rate of patients diagnosed after 2010 is less than 10%. 6 This considerable decrease in the mortality rate suggests that the identification and treatment of pylephlebitis have improved over time. 7
Unfortunately, although pylephlebitis usually presents as an acute illness, the primary infection is classified as subacute, and approximately one fifth of all cases are associated with appendicitis, resulting in the death of 11% to 32% of patients. 8 Pylephlebitis cannot be diagnosed immediately in most patients because of nonspecific symptoms. 9 Moreover, there is currently no diagnostic criteria for pylephlebitis. 10 Therefore, because of the vague symptoms at presentation, a high level of suspicion must be maintained to avoid fatal complications, and an early radiographic examination is necessary. 5 With blood sampling tests and imaging examinations, such as CT scans, an elevation in bilirubin concentrations can be reviewed to assess the portal system and the underlying abdominal primary pathology.11,12 Air bubbles or thrombi of the portal venous system are important CT findings of pylephlebitis. Therefore, CT is the most reliable initial diagnostic choice. 13 However, importantly, observing a dilated portal vein is unusual and could suggest portal venous thrombus even if the latter is not clearly observed on imaging.
One of the main applications of D-dimer measurement is to exclude the diagnosis of venous thromboembolism. Although there is a lack of specificity, studies have indicated that there is a positive correlation between the clinical severity of pylephlebitis and D-dimer concentrations, with D-dimer concentrations ≥1000 ng/mL. 14 Therefore, an increase in D-dimer concentrations may be a result of pylephlebitis complications in patients with appendicitis. 15 Pylephlebitis is difficult to diagnose in the early stages. However, pylephlebitis can be directly diagnosed on the basis of symptoms and blood test results, especially elevated bilirubin and abnormal D-dimer concentrations. D-dimer is a commonly used auxiliary indicator for venous thrombosis. When venous thrombosis is in the acute phase, D-dimer concentrations are increased. There is a high risk of thrombus detachment in the acute phase. Therefore, promptly adding anticoagulants after a clear diagnosis and rechecking D-dimer concentrations during treatment to clarify the status of the disease are recommended.
The principal treatment for pylephlebitis and sepsis is empiric broad antibiotics 16 until blood culture results are available. Reports have indicated that the infection is mostly polymicrobial and is positive in 62% of patients with pylephlebitis, but blood tests are not mandatory for a diagnosis. 3 The primary therapy for pylephlebitis involves antibiotic treatment to prevent the progression of sepsis. The use of specific and sensitive antibiotics based on blood culture results can quickly control infection. Patients should start taking anticoagulants if there is a thrombus or a positive hypercoagulability workup. 17 Stizenberg et al. reported that laparoscopic appendectomy could be delayed until 3 months after treatment with systemic antibiotics and anticoagulants. 18 The possible reason for this delay is that abscesses or adhesions around the appendix are severe. Moreover, if pylephlebitis is accompanied by septic shock, which is defined on the basis of the International Consensus, 19 a multidisciplinary approach should be undertaken, with early involvement of critical care medicine and haematology teams. Additionally, the patient should be supported with intravenous fluid resuscitation and intensive care treatment as required.
Pylephlebitis caused by acute appendicitis is not uncommon according to a review of the relevant literature. 20 However, our patient with acute appendicitis had no appendiceal gangrene, perforation, or fecalith blockage. In addition, he experienced severe septic shock, which might have been caused by bacteria within the mesoappendix entering the portal vein circulation through the mesoappendiceal vessel, resulting in subsequent septic shock and pylephlebitis. This situation is rare. Imaging showed no obvious portal vein thrombosis and only a dilated portal vein. Therefore, biliary tract disease, liver abscess, and inflammatory bowel disease were excluded. We believe that the diagnosis of presumed pylephlebitis was made primarily because of the finding of a dilated portal vein in the absence of a cause for preexisting portal hypertension in this patient. Elevated bilirubin concentrations and an unusual increase in D-dimer concentrations are important indicators for diagnosing pylephlebitis.
With regard to treatment of pylephlebitis, the cause of portal vein inflammation is acute appendicitis, and if the patient’s circulation is stable after anti-shock treatment, appendectomy should be performed within 72 hours. However, if the patient has severe infection, an unstable circulation, portal vein thrombosis, appendiceal perforation, abscess, or severe abdominal adhesions, appendectomy is not feasible because surgical treatment may worsen the condition and endanger the patient’s life. Patients should first receive conservative treatment, including fluid replacement, antibiotics, anticoagulation, and supportive therapy, and then wait for surgery. Based on previous case reports and our findings, we believe that the timing of surgery should be based on the following criteria. First, the symptoms of portal vein inflammation should completely disappear. An imaging examination should show no abnormalities in the portal vein and its branch system, normal coagulation function, normal blood culture, and there should be no fever or jaundice. Second, the swelling of the appendix should subside, localization should be performed, and the boundary with the surrounding organs should be clearly identified, and the patient’s abdominal pain symptoms should have disappeared. Although there is no unified standard for critically ill patients with pharyngitis, the waiting time for surgery should be at least 3 months or longer.
In our case, the patient underwent conservative treatment and successfully underwent laparoscopic appendectomy in the later stage. A follow-up examination after discharge showed no abnormalities. He was satisfied with the whole treatment process. The successful treatment of this patient can provide a basis for future diagnosis and treatment of pylephlebitis.
Conclusion
A multidisciplinary approach is mandatory for the decision-making process in the presence of pylephlebitis caused by appendicitis to obtain a correct diagnosis and prompt treatment. Timing for surgery is crucial for minimizing intra- and postoperative complications in appendicitis.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241244756 - Supplemental material for Pylephlebitis combined with septic shock secondary to acute nonperforated appendicitis: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605241244756 for Pylephlebitis combined with septic shock secondary to acute nonperforated appendicitis: a case report by Shi-Xing Wu, Hong-De Su and Xin-Jian Xu in Journal of International Medical Research
Footnotes
Author contributions
All of the authors contributed equally to the conception and design of the study, acquisition of the data, and/or the analysis and interpretation of the data for this work. All of the authors participated in drafting the or revising the manuscript for important intellectual content and gave final approval of the submitted manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The patient’s details have been deidentified. Written informed consent for publication was obtained from the patient. The case report was approved by the Ethics Review Committee of the Fifth Affiliated Hospital of Xinjiang Medical University.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.